Infections of the Central Nervous System (CNS)
Infections of the Central Nervous System (CNS)
Welcome to CNS Infections! This section is highly tested on exams because recognizing a CNS infection quickly is a matter of life and death.
1. Introduction to CNS Infections
The Central Nervous System (brain and spinal cord) is a highly protected fortress. However, when invaders breach the walls, the results are devastating. Why? Because the cranium (skull) and vertebrae are rigid bones. When infection causes inflammation and swelling, there is nowhere for the tissue to expand. This leads to increased pressure, crushing vital brain structures, resulting in significant morbidity (disability) and mortality (death).
The Monro-Kellie Doctrine
To understand why brain swelling is so lethal, think of the skull as a rigid, closed box containing three things: Brain Tissue (80%), Blood (10%), and CSF (10%). If a bacterial infection causes the brain tissue to swell with edema, it takes up more space. Because the skull cannot expand, the body must squeeze out the blood and CSF to make room. This leads to brain ischemia (lack of blood flow) and eventually pushes the brain out the bottom of the skull (herniation), which is fatal.
- Agents: Viruses, bacteria, fungi, protozoa, and helminths (parasites).
- The Mimics: Not everything that looks like an infection is one. Tumors, medications, and systemic illnesses can present with identical symptoms.
Timeline of Infection:
- Acute: Hours to days (highly virulent organisms, e.g., Bacterial Meningitis).
- Subacute: Days to weeks.
- Chronic: Weeks to months (e.g., Tuberculosis, Fungal infections).
Meningitis vs. Encephalitis
The distinction between these syndromes is technically artificial (since etiology and pathology often overlap—e.g., Tuberculous meningitis can be subacute or chronic), but it is crucial for guiding clinical management.
- Acute Meningitis: Inflammation of the meninges (the protective layers covering the brain). Characterized by the onset of meningeal symptoms over hours to days. Headache is the prominent early symptom, followed later by confusion, stupor, or coma if untreated.
- Chronic Meningitis: Symptoms, signs, and abnormal Cerebrospinal Fluid (CSF) findings last for at least 4 weeks.
- Encephalitis: Infection/inflammation of the brain tissue itself (parenchyma). Distinguished by decreased mentation (confusion, stupor, altered mental status) or seizures EARLY in the course of the disease, with minimal meningeal signs (stiff neck).
Clinical Pearl & Classic Presentation
Most patients with CNS infections present with a classic triad/tetrad: Fever, Headache, Altered Mental Status, and Focal Neurologic Deficits. However, be careful on exams! These are nonspecific, and not every patient will have all of them.
The ER Triage: Meningitis
A 20-year-old college student presents to the ER with a severe, pounding headache, a fever of 103°F, and severe photophobia (light hurts his eyes). When you ask him to touch his chin to his chest, he screams in pain (nuchal rigidity). He knows his name, location, and the date.
Diagnosis: Meningitis. The infection is currently localized to the meningeal wrappers; his actual brain tissue is intact, so his mental status is completely normal right now.
The ER Triage: Encephalitis
A 45-year-old man is brought in by his wife. He has a mild fever. She says he has been acting "bizarrely," talking to people who aren't there, and earlier he had a grand mal seizure. His neck is completely soft and pain-free when bent.
Diagnosis: Encephalitis. The infection has directly attacked the brain tissue (parenchyma), immediately altering his personality and triggering electrical storms (seizures), without inflaming the meninges.
2. Epidemiology and Etiology (The "Who" and "What")
A. Bacterial Meningitis
Bacterial meningitis remains a major global threat. Historically, Haemophilus influenzae type B (HiB) was a leading cause in children, but thanks to the HiB vaccine, its incidence has drastically declined.
The "Big Three" (Account for >80% of cases):
- Haemophilus influenzae (45% historically, capsular type B strains)
- Streptococcus pneumoniae (47%, 18 pneumococcal serotypes)
- Neisseria meningitidis (Serogroups B, C, and Y)
Other important causes:
- Streptococcus agalactiae (Group B Strep - 52% incidence in its specific demographic). Most common cause in neonates!
- Listeria monocytogenes (8%, serotypes 1/2b and 4b). Affects the very young, very old, and pregnant/immunocompromised.
- Aerobic Gram-Negative Bacilli (Klebsiella, E. coli, Serratia, Pseudomonas, Salmonella).
- Staphylococci (S. aureus, S. epidermidis).
Exam High-Yield: Bacteria by Age & Predisposing Factor
| Age / Risk Factor | Bacterial Pathogens to Suspect | Clinical Logic (Why?) |
|---|---|---|
| < 1 month (Neonate) | S. agalactiae, E. coli, L. monocytogenes, Klebsiella pneumoniae | Baby catches these passing through the mother's birth canal or from maternal blood. |
| 1 - 23 months | S. agalactiae, E. coli, H. influenzae, S. pneumoniae, N. meningitidis | Maternal antibodies wane; baby is exposed to respiratory droplets in daycare. |
| 2 - 50 years (Adults) | S. pneumoniae, N. meningitidis | Standard community-acquired respiratory transmission. (Close quarters like dorms/military barracks highly favor N. meningitidis). |
| > 50 years (Elderly) | S. pneumoniae, N. meningitidis, L. monocytogenes, Gram-negative bacilli | Aging immune system allows Listeria (from unpasteurized foods) and gut bacteria to invade. |
| Immunocompromised | S. pneumoniae, N. meningitidis, L. monocytogenes, Gram-negatives (incl. P. aeruginosa) | Lack of T-cell/B-cell function allows opportunistic bugs to thrive. |
| Basilar Skull Fracture | S. pneumoniae, H. influenzae, Group A Strep | Fracture connects the nasopharynx directly to the brain, allowing respiratory flora to leak in. |
| Head Trauma / Neurosurgery | S. aureus, S. epidermidis, P. aeruginosa | Skin flora and resistant hospital bugs get pushed directly into the skull. |
Listeria monocytogenes is unique because it grows extremely well in cold temperatures (like inside a refrigerator). This is why pregnant women, the elderly, and immunocompromised patients are explicitly warned to avoid unpasteurized soft cheeses, cold deli meats, and hot dogs. Eating these can introduce Listeria into the gut, which then crosses into the blood and preferentially attacks the meninges.
B. Viral Meningitis
Viruses are the major cause of "Aseptic Meningitis". "Aseptic" means the patient has meningitis symptoms and lymphocytic pleocytosis (high lymphocyte white blood cells in CSF), but routine bacterial cultures come back negative.
- Enteroviruses: The most common cause overall.
- Herpesviruses: HSV-1, HSV-2, VZV (Chickenpox/Shingles), CMV, EBV, HHV-6/7/8. (Exam note: HSV-1 is the most common cause of fatal, sporadic viral encephalitis, notoriously destroying the temporal lobes of the brain).
- HIV: Can cross the meninges early during primary infection or persist in already infected patients.
- Others: Arboviruses (mosquito/tick-borne), Mumps virus, Lymphocytic Choriomeningitis Virus (LCMV).
C. Spirochetal, Protozoal, and Helminthic Infections
- Spirochetes:
- Treponema pallidum (Syphilis): Disseminates early. Neurosyphilis has 4 syndromes:
- Syphilitic meningitis: Peaks first 2 years (0.3 - 2.4% of untreated cases).
- Meningovascular syphilis: Strokes/vascular issues months to years later (peaks ~7 years).
- Parenchymatous neurosyphilis: General paresis (insanity) and Tabes dorsalis (spinal cord demyelination), appears 10-20 years later.
- Gummatous neurosyphilis: Late tertiary manifestation, tumors in the brain.
- Borrelia burgdorferi: Causes Lyme disease (tick-borne).
- Treponema pallidum (Syphilis): Disseminates early. Neurosyphilis has 4 syndromes:
- Protozoa: Amebas (Naegleria fowleri [brain-eating ameba from warm lakes], Acanthamoeba).
- Helminths (Worms): Angiostrongylus cantonensis, Baylisascaris procyonis.
Clinical Scenario: Chronic Meningitis
If a patient presents with meningitis symptoms lasting over a month, suspect chronic agents. TB and Syphilis are classic. If they have HIV/AIDS, suspect Cryptococcosis or Histoplasmosis. If they are an outdoorsman, consider Lyme disease or fungal infections like Coccidioidomycosis or Blastomycosis.
3. Pathogenesis and Pathophysiology (The "How")
How does a bacteria sitting in your nose end up destroying your brain? This is a highly tested sequence of events.
A. Bacterial Meningitis Pathogenesis Steps
Step 1: Mucosal Colonization and Systemic Invasion
- Attachment: The bacteria first land in the nasopharynx. They use fimbriae (or pili) to grab onto nasopharyngeal epithelial cells. N. meningitidis specifically attaches to a host cell surface receptor called CD46.
- Invasion: Once attached, they trick the cell into swallowing them in a phagocytic vacuole. H. influenzae takes a different route: it breaks down the tight junctions between epithelial cells, invading intercellularly.
- Evasion at the mucosa: The host produces secretory IgA to fight them, but bacteria produce IgA proteases to chop up these defensive antibodies.
Step 2: Intravascular Survival (Surviving the Bloodstream)
- Once in the blood, bacteria must avoid neutrophils and the complement system. The ultimate weapon is the Bacterial Polysaccharide Capsule (found in H. influenzae, N. meningitidis, S. pneumoniae, E. coli, S. agalactiae). The capsule acts like a slippery shield, preventing phagocytosis.
- Host counter-attack: The host uses the alternative complement pathway. The capsular polysaccharide of S. pneumoniae triggers the cleavage of C3, which attaches to the bacterial surface. This acts as a tag (opsonization) to help macrophages eat them.
Step 3: Meningeal Invasion (Crossing the Blood-Brain Barrier - BBB)
To cross into the brain, bacteria must achieve a sustained, high-grade bacteremia (a massive amount of bacteria in the blood).
- Where do they cross? Via the dural venous sinus system, above the cribriform plate, or primarily the choroid plexus (which produces CSF and has a massive blood flow of 200 mL/g/min).
- How do they cross?
- N. meningitidis expresses PilC protein to adhere to the endothelium.
- They manipulate host cell skeletons using microtubule/microfilament-dependent pathways to force the BBB open.
- Expression of specific virulence genes like OmpA and ibe10 (in E. coli).
- Trojan Horse mechanism: Hitching a ride inside migrating monocytes.
- L. monocytogenes is directly taken up by endothelial cells.
- Pneumococci interact with the PAF (Platelet-Activating Factor) receptor to be transcytosed across the cell.
Step 4: Bacterial Survival within the Subarachnoid Space (CSF)
- The CSF is an immunological desert. It has zero or minimal complement components and very low immunoglobulins (IgG ratio blood-to-CSF is 800:1).
- Because capsules require complement and antibodies (opsonization) to be defeated, the bacteria multiply rapidly to huge concentrations without interference.
- The Inflammatory Cascade: The presence of bacteria eventually calls in White Blood Cells (neutrophilic pleocytosis). The alarm bells are:
- Complement component C5a (a powerful chemotactic factor).
- Macrophage Inflammatory Proteins (MIP-1α and MIP-2).
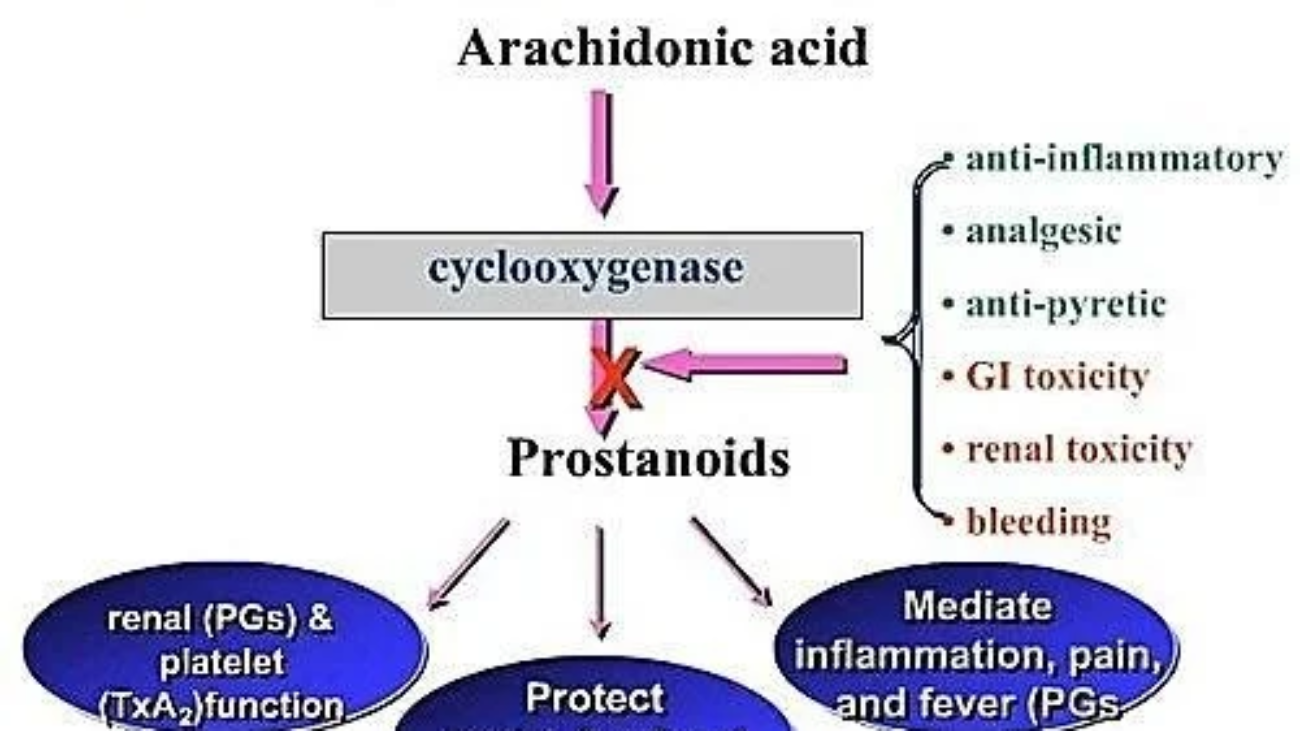
- Prostaglandin E2 (PGE2).
- Chemokines: IL-8, growth-related gene product-α, monocyte chemotactic protein 1.
- Leukocytes use Selectins to roll along blood vessels, and adhesion molecules (ICAM-1, Endothelial leukocyte adhesion molecule 1) to squeeze into the CSF. However, without opsonins, they are mostly useless at eating the bacteria.
Step 5: Pathophysiologic Consequences (The Damage)
It isn't just the bacteria causing damage; it's the host's massive, unregulated inflammatory response to bacterial lytic products (cell wall components like peptidoglycan, LPS/lipo-oligosaccharide).
*Note: When you give antibiotics, bacteria explode. By bursting the bacteria, massive amounts of these toxic cell wall products (LPS) are suddenly released into the CSF, which temporarily worsens the massive inflammatory fire!
The Fix: This is why in suspected bacterial meningitis (especially S. pneumoniae), we administer Dexamethasone (a powerful steroid) 15 minutes BEFORE or exactly WITH the first dose of antibiotics. The steroid blunts the host's inflammatory response to the exploding bacteria, reducing brain damage, deafness, and mortality.
- Alteration of the BBB: Cytokines (IL-1, TNF-α) and bacterial products cause the BBB to break down. Tight junctions separate, pinocytosis increases, and large proteins like albumin leak into the CSF. Matrix Metalloproteinases (MMPs) degrade the extracellular matrix, destroying the barrier further.
- Increased Intracranial Pressure (ICP): Driven by massive cerebral edema (brain swelling) which can cause fatal brain herniation. Three types of edema occur simultaneously:
- Vasogenic Edema: Fluid leaks from leaky blood vessels (due to BBB breakdown).
- Cytotoxic Edema: Brain cells swell and die from toxic factors (neutrophil toxins, peptidoglycan).
- Interstitial Edema: Pus and inflammation block the normal drainage of CSF, causing hydrocephalus.
- Alterations in Cerebral Blood Flow: The inflammation causes vasculitis (blood vessel swelling), leading to thrombosis (clots), ischemia, and infarction (strokes). The brain suffers from hypoperfusion (not enough blood, mediated by endothelin) or hyperperfusion. Venous engorgement worsens the high ICP.
- Neuronal Injury: Brain cells die due to:
- Oxygen free radicals.
- TNF-α triggering apoptosis (programmed cell death).
- Bacterial toxins like pneumolysin.
- Activation of PARP enzyme and caspase-3.
- Reactive nitrogen intermediates (Nitric oxide, Peroxynitrite).
- Release of excitatory, toxic amino acids (Glutamate, aspartate).
B. Viral Pathogenesis
- Initiation: Viruses face barriers: mucociliary elevator (sweeps them out of lungs), alveolar macrophages, gastric acidity, and GI bile/enzymes. (Acid-resistant viruses like Enteroviruses survive the gut). Secretory IgA tries to neutralize them.
- Viremia & Invasion: If they survive, they multiply in extraneural sites (e.g., tonsils, Peyer's patches in the gut via M cells). They enter the blood (primary viremia), go to the liver/spleen, multiply heavily, and re-enter the blood (secondary viremia).
- CNS Entry: They cross the BBB by infecting endothelial cells directly, hiding in leukocytes (Trojan horse), crossing the choroid plexus, or crawling up nerves (olfactory or peripheral spinal nerves).
- Spread & Clearance: Spread via CSF or jumping across synapses (axons/dendrites). Unlike bacteria, the body handles viruses better using Sensitized Lymphocytes and cytokines (IL-6, IFN-γ, TNF-α, IL-1β). Local B cells make plasma cells in the CSF. T-cell response is the most critical for viral clearance. (Patients with poor T-cell immunity get chronic viral infections).
4. Clinical Features and Diagnosis
A. History and Presentation (Bacterial)
Symptoms are sudden and severe. Look for:
- Headache: ≥ 90% frequency.
- Fever: ≥ 90% frequency.
- Meningismus (Stiff Neck / Nuchal Rigidity): ≥ 85%. Clinical signs include Kernig's sign (pain on leg extension while hip is flexed) and Brudzinski's sign (neck flexion causes involuntary knee bending).
- Altered Sensorium: > 80%.
- Other signs: Vomiting (~35%), Seizures (~30%), Focal neurologic findings (10-20%), Papilledema (<5% - swelling of optic disc).
B. Diagnostic Workup (The Lumbar Puncture)
The definitive test is examining the CSF via a lumbar puncture (spinal tap). Here is what you will find in Bacterial Meningitis:
| CSF Parameter | Typical Bacterial Finding | Why? (Pathophysiology) |
|---|---|---|
| Opening Pressure | Very High: 200 - 500 mm H2O | Massive brain edema and blocked CSF outflow. |
| White Blood Cell Count | 1,000 - 5,000 / mm³ | Massive immune recruitment. |
| Cell Type | ≥ 80% Neutrophils (PMNs) | Neutrophils are the body's first responders to bacteria. |
| Protein | High: 100 - 500 mg/dL | The BBB is destroyed; large serum proteins leak into CSF. |
| Glucose | Very Low: ≤ 40 mg/dL (CSF-to-serum ratio ≤ 0.4) |
Bacteria and thousands of active neutrophils are consuming all the glucose for energy. |
Other Tests: Gram stain is positive 60-90% of the time. Culture is positive 70-85%. PCR is highly promising.
You perform a lumbar puncture on a sick patient. The results show:
WBC: 150 (mildly elevated)
Cell Type: 90% Lymphocytes
Protein: 60 mg/dL (slightly high)
Glucose: 65 mg/dL (Normal ratio to blood)
Diagnosis: Viral Meningitis. (See below for details on why!)
C. Diagnosis of Viral Meningitis
- CSF Findings: Lower WBC (100-1,000). Initially, neutrophils may dominate, but by 48 hours, Lymphocytes predominate. Protein is only mildly elevated. Glucose is usually NORMAL (because viruses don't eat glucose).
- Viral Specifics: Enteroviral immunoassay is tough because of too many serotypes. PCR is the gold standard for enteroviral meningitis (Sensitivity 86-100%, Specificity 92-100%).
5. Treatment and Prevention
A. Treatment of Bacterial Meningitis
This is a medical emergency. Do not wait for cultures to result before starting antibiotics!
- Haemophilus influenzae type B: Third-generation cephalosporin (e.g., Ceftriaxone). If β-Lactamase negative: Ampicillin.
- Neisseria meningitidis: Penicillin G or Ampicillin.
- Streptococcus pneumoniae: Vancomycin PLUS a 3rd-generation cephalosporin. (Why? Pneumococcus is highly resistant to penicillin globally, so you must use Vanco to be safe).
- Listeria monocytogenes: Ampicillin or Penicillin G. (Exam pearl: Cephalosporins DO NOT kill Listeria. You must add Ampicillin for elderly/neonates).
- Streptococcus agalactiae (GBS): Ampicillin or Penicillin G.
- Escherichia coli / Enterobacteriaceae: Third-generation cephalosporin.
- Pseudomonas aeruginosa: Ceftazidime or Cefepime.
- Staphylococcus aureus: Nafcillin/Oxacillin (if methicillin-sensitive) or Vancomycin (if MRSA).
- Spirochetes / Protozoa: Syphilis = Penicillin G. Lyme = 3rd gen Ceph. Naegleria = Amphotericin B + Rifampin + Doxycycline.
If you don't know the bug yet, you treat empirically based on age!
- Neonates (<1 mo): Ampicillin (for Listeria/GBS) + Cefotaxime (for Gram negatives). Note: Do not use Ceftriaxone in neonates, it causes jaundice/kernicterus!
- Adults (2-50 yrs): Ceftriaxone + Vancomycin (Covers S. pneumo and N. meningitidis).
- Elderly (>50 yrs): Ceftriaxone + Vancomycin + AMPICILLIN (must add Ampicillin back in because Listeria risk returns!).
B. Prevention
- Viral: Mumps live-attenuated vaccine (given in 2nd year of life, >97% protection).
- Bacterial Vaccines:
- HiB: Conjugate vaccines (PRP-OMP / PedvaxHIB).
- N. meningitidis: Quadrivalent vaccine covering serogroups A, C, Y, and W135.
- S. pneumoniae: 23-valent pneumococcal vaccine.
- Chemoprophylaxis: Giving antibiotics to close contacts of a sick patient to eradicate nasopharyngeal carriage. Used for HiB, but not widely recommended for all bugs.
6. Cerebrospinal Fluid (CSF) Shunt Infections
Hydrocephalus (excess CSF) is treated by putting a plastic tube (shunt) into the brain ventricles to drain fluid to the belly (VP shunt), lungs, or heart. Infection incidence is 5% to 41%.
Pathogenesis & Risk Factors
Four ways they get infected: Retrograde (crawling up from the belly), Skin breakdown over the tubing, Hematogenous (bloodstream), or Colonization at the time of surgery (most common).
Risk Factors: Premature birth, prior shunt infection, inexperienced neurosurgeon, high number of people walking through the OR, long surgical procedure, shaving the skin, huge skin exposure.
The Culprits (Microbiology)
- Staphylococci (esp. Coagulase-Negative Staph - CONS like S. epidermidis): Account for 65 - 85%!
- Gram-negatives (E. coli, Klebsiella, Pseudomonas): 6-20%.
- Streptococci (8-10%), Corynebacteria (1-14%), Anaerobes (6%).
Why is S. epidermidis so dangerous here? (Virulence Factors)
- It binds to host proteins like fibronectin and collagen coating the plastic.
- It literally excavates and hydrolyzes the plastic polymer as food!
- It produces an extracellular slime substance (Biofilm). This slime protects them from antibiotics like an invisible forcefield and alters neutrophil function. Neutrophils stick poorly to the catheter, release oxygen radicals that damage host tissue, but fail to eat the bacteria inside the slime.
Clinical Features
Can be subtle: Headache, nausea, lethargy, change in mental status, fever. Pain often occurs at the distal end (e.g., belly pain if the infection is in the peritoneal cavity VP shunt).
7. Brain Abscess
A brain abscess is a localized, focal intracerebral infection. It starts as a diffuse brain inflammation (cerebritis) and walls off into a collection of pus surrounded by a well-vascularized capsule. It acts exactly like a growing brain tumor.
Microbiology
- Streptococci (70%): Especially the S. anginosus (milleri) group. Normal flora of the mouth.
- Anaerobes (20-40%): Bacteroides and Prevotella.
- Staphylococcus aureus (15%): Especially after head trauma or surgery.
- Enteric Gram-Negatives (23-33%): Proteus, E. coli, Klebsiella.
- Fungal/Parasitic: Candida, Aspergillus, Mucormycosis, T. gondii (Classic in HIV patients), T. solium (pork tapeworm).
Pathogenesis (How does it get there?)
- Contiguous Spread (Most Common): Infection eats through the skull from right next door.
- Otitis media / Mastoiditis (Ear infections) → Temporal lobe or Cerebellar abscess. (Usually Strep, Bacteroides).
- Frontal/Ethmoid Sinusitis → Frontal lobe abscess.
- Dental sepsis → Mixed flora (Fusobacterium, Prevotella).
- Hematogenous Spread (Bloodstream): Distant infection embolizes to the brain. Often causes multiple abscesses.
- Lung issues: Lung abscess, empyema, bronchiectasis, cystic fibrosis.
- Heart issues: Bacterial endocarditis (S. aureus), Congenital heart defects.
- Trauma: Open cranial fracture, neurosurgery.
Clinical Presentation
Symptoms are due to a space-occupying lesion (pressure), NOT systemic infection. Fever is present in less than 50% of patients! The classic triad (Headache, fever, focal deficit) is seen in <50%.
- Headache (~70%), Mental status changes (≤70%), Focal deficits (>60%).
- Frontal Lobe: Drowsiness, personality changes, hemiparesis (weakness on one side), motor speech issues.
- Temporal Lobe: Aphasia (can't understand/speak), visual field defect (upper homonymous quadrantanopsia).
- Cerebellum: Ataxia (clumsiness), nystagmus (eye darting), vomiting.
- Brainstem: Facial weakness, dysphagia (trouble swallowing).
CRITICAL EXAM WARNING: Diagnosis
If you suspect a Brain Abscess (focal signs, papilledema), DO NOT DO A LUMBAR PUNCTURE. The abscess creates massive pressure inside the brain. If you puncture the lower spine, you create a pressure vacuum, and the brain will instantly herniate out of the base of the skull, killing the patient on the table.
Diagnosis Workup
- Imaging: CT or Magnetic Resonance Imaging (MRI) is the test of choice. You will see a classic "Ring-enhancing lesion" (the vascular capsule lights up). (Exam Pearl: If you see multiple ring-enhancing lesions in an HIV+ patient, Toxoplasmosis is the #1 suspect).
- Microbiology: CT-guided aspiration (stick a needle in and drain it) or surgical biopsy.
- Stains: Gram stain, aerobic/anaerobic cultures. Special stains: Acid-fast (Mycobacteria), Modified acid-fast (Nocardia), Mucicarmine/Methenamine silver (Fungi).
8. Other CNS Infections
A collection of pus specifically in the space between the dura mater and the arachnoid mater. Since this is an unconstrained potential space, pus can spread quickly over the entire hemisphere of the brain.
A localized collection of pus between the dura mater and the overlying skull or vertebral column bone. Because the dura is tightly attached to the skull, these are physically confined and don't spread as fast in the head, but are VERY dangerous when occurring in the spinal cord, threatening paralysis.
Venous thrombosis (clot) mixed with suppuration (pus) in the brain's veins. Usually starts after a facial, sinus, ear, or throat infection. It spreads discontinuously and often happens alongside epidural/subdural abscesses or meningitis.
Quick Quiz
CNS Infections Quiz
Microbiology - mobile-friendly and focused practice.
Privacy: Your details are used only for quiz tracking and certificates.
CNS Infections Quiz
Microbiology
Preparing questions...
Choose your answer and keep your streak alive.
Great effort.
Here is your quick performance summary.