Homeostasis
Imagine you're driving a car, aiming to maintain a constant speed of 60 mph. You press the gas going uphill and ease off going downhill. Your goal is to keep that speed constant despite external changes. That's essentially what your body does, constantly, for hundreds of variables.
Homeostasis (from Greek "homoios" meaning "similar" and "stasis" meaning "standing still") is the ability of an organism to maintain a relatively stable internal environment despite continuous changes in the external environment. It's not a static state, but a dynamic equilibrium where conditions fluctuate within narrow, acceptable limits around a set point.
Many physiologists translate this into the saying, “constantly changing to stay the same.” The ability of the human body to quickly adapt to any changes and to re-establish stability is the essence of homeostasis.
The Importance of Homeostasis
Survival itself depends on the body's ability to maintain this internal balance. Deviations outside the normal range can impair cell function, leading to disease or death.
Enzyme and Protein Function
Almost all biochemical reactions are catalyzed by enzymes (proteins), which are highly sensitive to their environment.
Impact of Imbalance: Deviations in temperature or pH can denature enzymes, altering their 3D shape and halting vital metabolic pathways.
Cellular Integrity and Volume
The cell membrane's selective permeability and active transport mechanisms are critical for maintaining appropriate solute concentrations.
Impact of Imbalance: Changes in extracellular fluid osmolarity can cause cells to swell and burst (lysis) or shrink and die (crenation). Disrupted ion gradients incapacitate nerve and muscle function.
Efficient Communication Systems
The nervous and endocrine systems require specific conditions to transmit signals effectively.
Impact of Imbalance: Improper electrolyte balance (Na⁺, K⁺, Ca²⁺) can lead to severe nerve and muscle dysfunction, including seizures, paralysis, and cardiac arrhythmias.
Energy Production (ATP)
Cells require a continuous supply of oxygen and nutrients, and efficient removal of waste, to produce ATP.
Impact of Imbalance: Oxygen deprivation (hypoxia) leads to a cellular energy crisis and buildup of lactic acid. Accumulation of wastes like CO₂ can become toxic and alter pH, leading to organ failure.
Immune System Function
Immune cells and proteins need stable conditions to effectively fight off pathogens without harming healthy tissues.
Impact of Imbalance: Uncontrolled fever can become detrimental to immune cells themselves. Chronic stress and elevated cortisol can suppress the immune system.
Examples of Homeostatically Regulated Variables
The body tightly regulates hundreds of variables to maintain this dynamic equilibrium. Key examples include:
- Body temperature
- Blood pressure
- Blood glucose levels
- Blood pH
- Oxygen and carbon dioxide levels
- Water balance
- Ion concentrations (Na⁺, K⁺, Ca²⁺)
Homeostasis is Maintained by Feedback Loops
The primary way the human body maintains homeostasis is with the use of feedback loops. A feedback loop is a mechanism that allows for continual assessment of the body’s physiology and a way to correct various elements if they should go out of balance. There are two types of feedback loops: negative and positive.
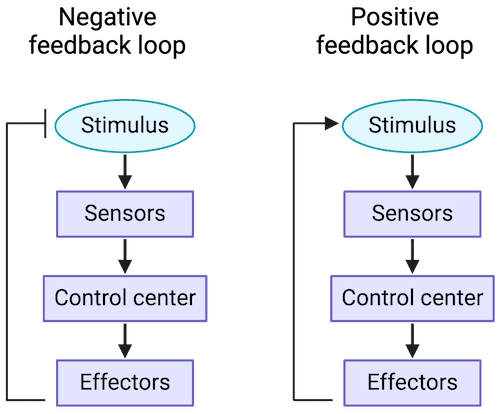
Negative Feedback Loop
The response opposes (or negates) the original stimulus. This is by far the most common type in the human body.
Positive Feedback Loop
The response augments (or intensifies) the original stimulus. The cycle repeats until it is broken. This type is very rare but critically important.
Parameters and Set Points
For any feedback loop, there is a parameter that is being monitored, and it has a set point, or a ‘normal range’ in which it exists when the body is in balance. The stimulus that starts the feedback loop is a change in that parameter that pushes it above or below its normal set point range.
| Table 1.1: Examples of Blood Parameters and Their Set Points | |
|---|---|
| Osmolarity of Blood | 295-310 mOsM |
| pH of Blood | 7.35-7.45 |
| Arterial PCO₂ | 35-46 mmHg |
| Arterial PO₂ | 80-100 mmHg |
| Glucose (fasting) | 70-100 mg/dL |
| Sodium (Na⁺) | 135-145 mM |
| Potassium (K⁺) | 3-5 mM |
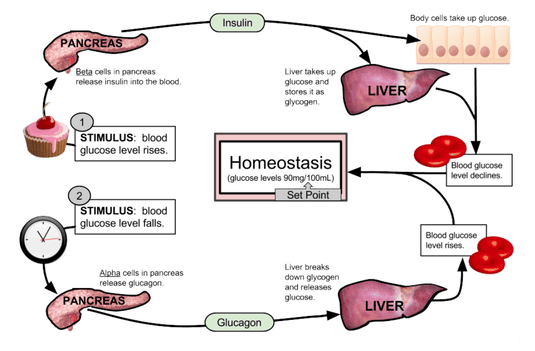
Example: Blood Glucose Regulation (Between Meals)
A person’s blood glucose (parameter) has a normal range (set point) of 70 to 100 mg/dL. If a person has not eaten in a while, their blood glucose decreases. If it goes below 70 mg/dL, the person will have hypoglycemia (low blood sugar). This decrease is the stimulus.
This decrease is detected by receptors in the pancreas, which responds by releasing the hormone glucagon into the bloodstream. Glucagon travels to the liver and stimulates hepatocytes (liver cells) to break down their glycogen stores and release glucose molecules into the blood. This increases blood glucose levels, opposing the original stimulus. Once glucose is restored to its normal range, the signal for glucagon release dissipates. This "off switch" is a key element of negative feedback.
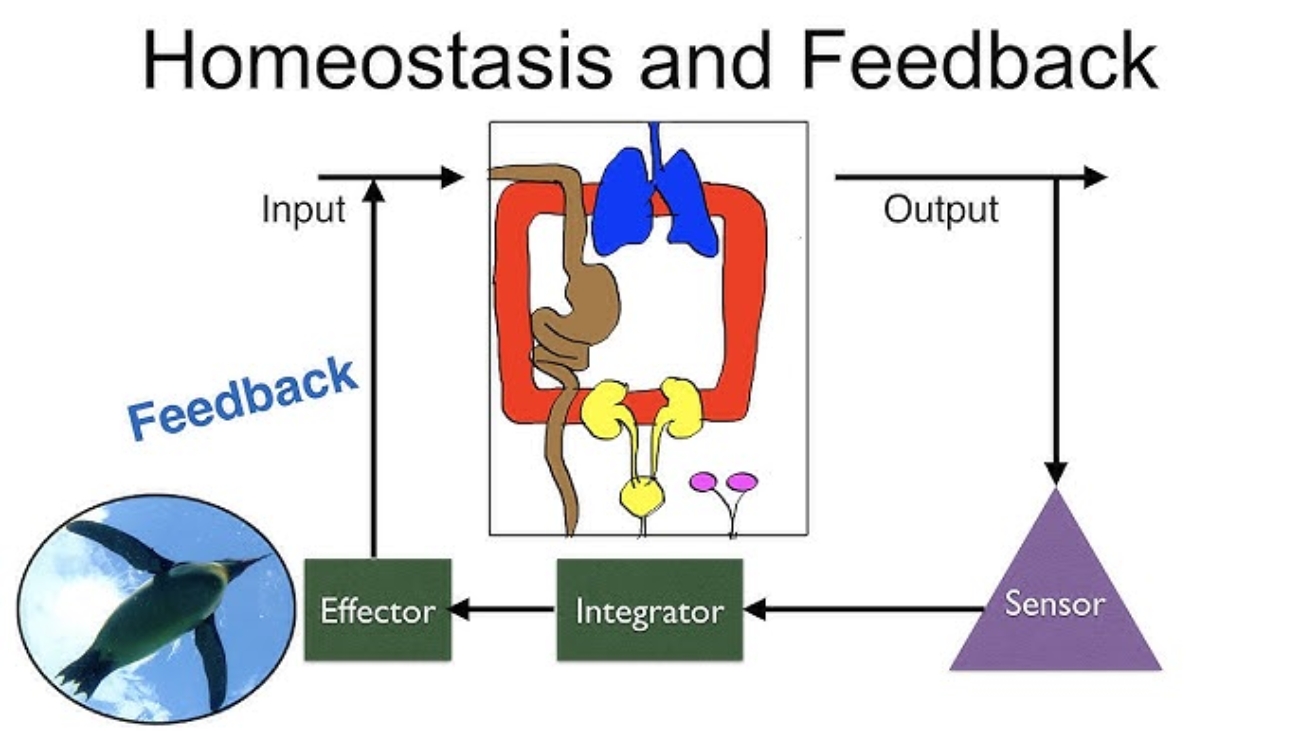
The Nitty Gritty of the Feedback Loop
To describe feedback loops with consistent terms, we can identify seven general components that create the loop.
Homeostatic Control Mechanisms (The "Feedback Loops")
To maintain homeostasis, the body uses control systems, most of which involve feedback loops. These loops constantly monitor conditions, detect changes, and initiate responses to bring variables back to their set point.
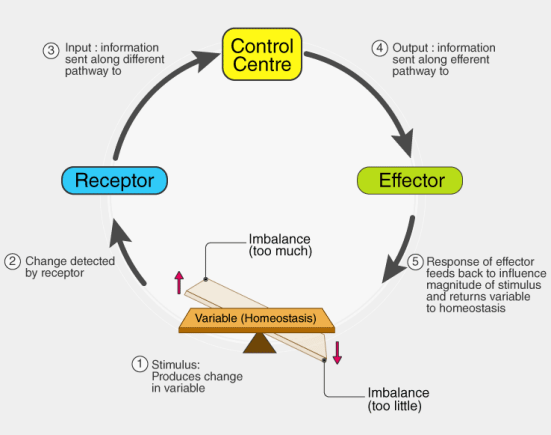
Every feedback loop has three basic components:
1. Receptor (Sensor)
Function: Monitors the environment and responds to changes (stimuli). It detects the deviation from the set point.
Action: Sends information (input) along an afferent pathway (e.g., nerve impulses) to the control center.
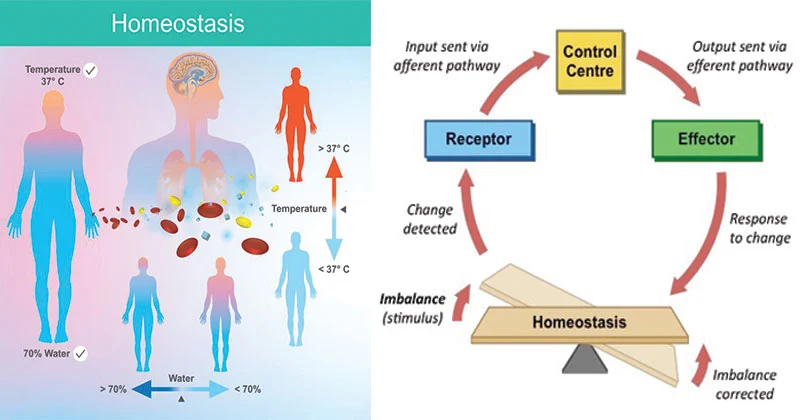
Example: Thermoreceptors in the skin and hypothalamus detect changes in body temperature.
2. Control Center (Integrator)
Function: Receives and analyzes the input from the receptor. It compares the input to the set point (the ideal value) and determines the appropriate response.
Action: Sends commands (output) along an efferent pathway (e.g., nerve impulses, hormones) to the effector.
Example: The hypothalamus in the brain acts as the body's thermostat, comparing current body temperature to the set point of ~37°C (98.6°F).
3. Effector
Function: Carries out the control center's response. It provides the means for the control center's output to affect the stimulus.
Action: Its action either reduces the stimulus (negative feedback) or enhances it (positive feedback).
Example: Sweat glands, blood vessels in the skin, and skeletal muscles (shivering) are effectors that help regulate body temperature.
The Communication Pathway
RECEPTOR
Afferent Pathway
CONTROL CENTER
Efferent Pathway
EFFECTOR
Types of Feedback Loops
Negative Feedback Loops
(Most Common and Essential for Homeostasis)
Mechanism: The output of the system shuts off or reduces the intensity of the original stimulus, bringing the variable back toward the set point. It works to counteract the change.
Goal: To prevent severe changes and maintain stability.
Analogy: A thermostat controlling a furnace. When the temperature drops, the furnace turns on. Once the temperature reaches the set point, the furnace turns off (negative feedback).
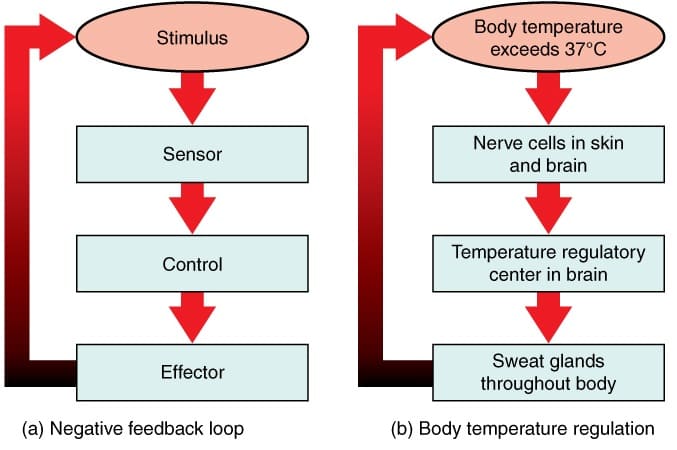
Specific Example: Increased Body Temperature
If a person has been digging in the garden on a hot day, their body temperature rises above its set point of about 98.6°F. This is the stimulus. Thermoreceptors in the skin detect this change and send afferent information to the hypothalamus (the integration center). The hypothalamus then sends efferent signals to the effector tissues: sweat glands and cutaneous blood vessels. The response is diaphoresis (sweating) and cutaneous vasodilation (widening of blood vessels in the skin). Evaporation of sweat and increased blood flow to the skin dissipate heat, causing body temperature to decrease back to its set point.
Other Physiological Examples:
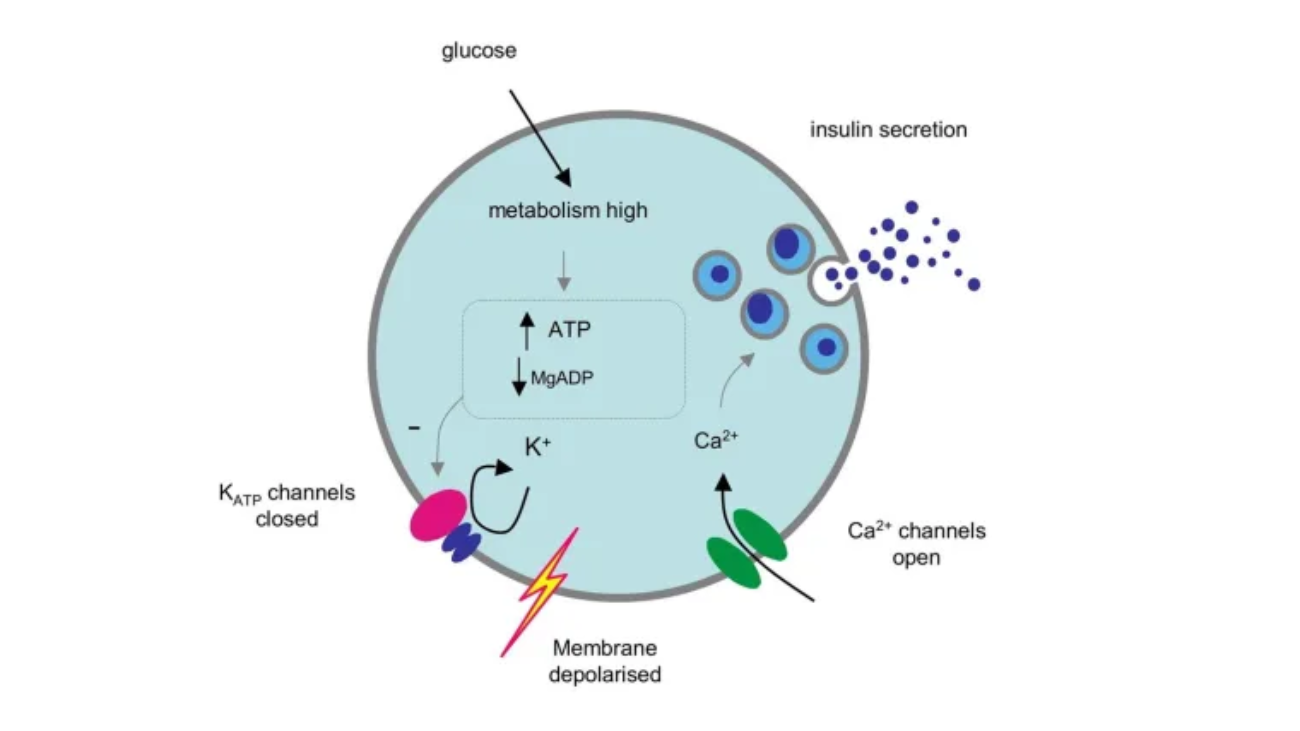
- Blood Glucose Regulation: After a meal, high blood glucose stimulates the pancreas to release insulin. Insulin causes cells to take up glucose, lowering blood glucose levels.
- Blood Pressure Regulation: Baroreceptors detect high blood pressure, signal the brain, which then slows heart rate and dilates blood vessels to lower pressure.
Positive Feedback Loops
(Rare, but Important for Specific Events)
Mechanism: The output of the system enhances or exaggerates the original stimulus, driving the variable further away from the initial set point. This is often part of a process that needs to be completed quickly.
Goal: To amplify a process until a specific event is completed.
Analogy: A microphone picking up sound, which is amplified and fed back into the microphone, creating a loop of increasing volume.
Specific Example: Childbirth
When a baby is ready to be born, its head pushes down upon the cervix, increasing pressure. This stretch (the stimulus) is detected by mechanoreceptors, which send an afferent signal to the brain. The brain (integration center) signals the posterior pituitary to release the hormone oxytocin. Oxytocin (efferent pathway) travels in the blood to the uterus (effector tissue), causing its smooth muscle to contract more forcefully. This pushes the baby’s head harder against the cervix, intensifying the original stimulus and triggering more oxytocin release. This cycle repeats, with contractions becoming stronger and more frequent, until the baby is born, which breaks the loop.
Other Physiological Examples:
- Blood Clotting: Platelets at an injury site release chemicals that attract more platelets, rapidly forming a plug.
- Generation of an Action Potential: An initial depolarization opens some Na⁺ channels, causing more Na⁺ to enter, which opens even more Na⁺ channels, leading to a rapid, all-or-nothing spike.








 Superficial Layer
Superficial Layer