Nursing Informatics: Batch 2
ICT in Practice, Patient Education, and Research
Test your knowledge with these 30 questions.
Nursing Informatics: Batch 2
Question 1/30
Assessment Complete!
Here are your results, .
Your Score
27/30
90%

Test your knowledge with these 30 questions.
Question 1/30
Here are your results, .
Your Score
27/30
90%
Test your knowledge with these 30 questions.
Question 1/30
Here are your results, .
Your Score
27/30
90%

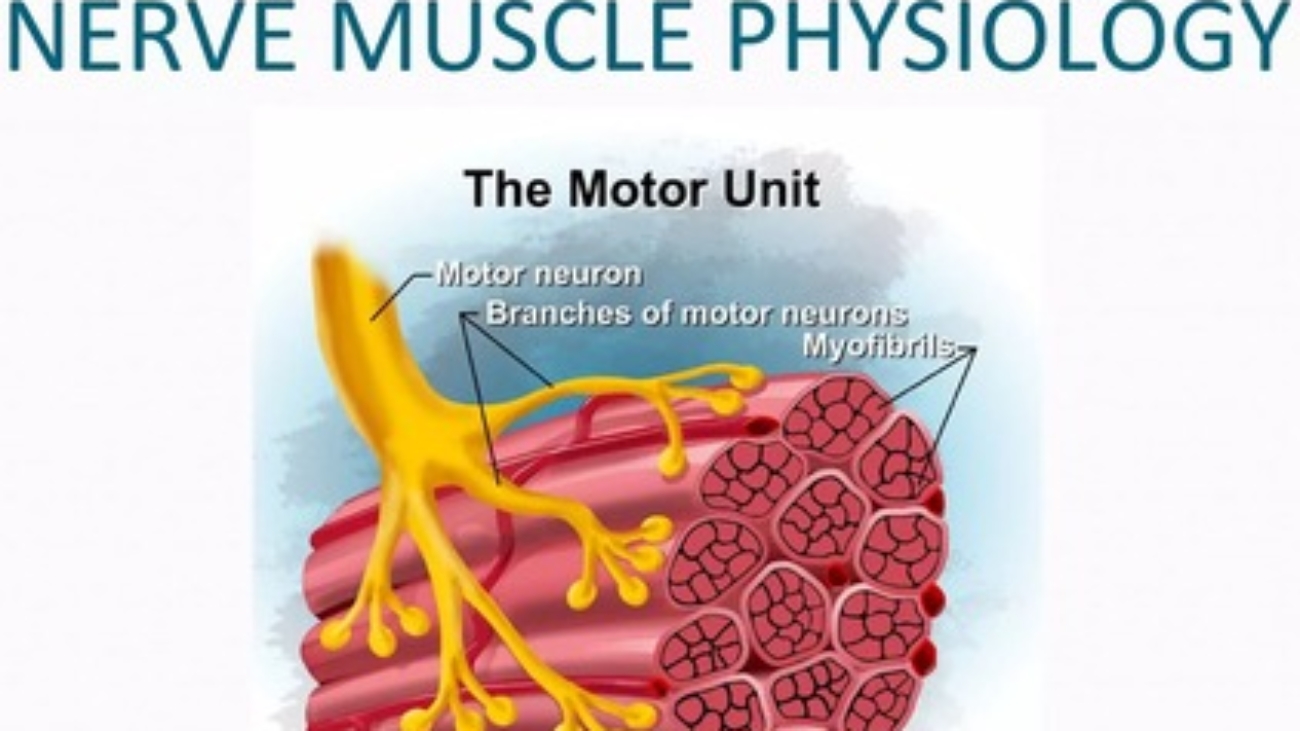
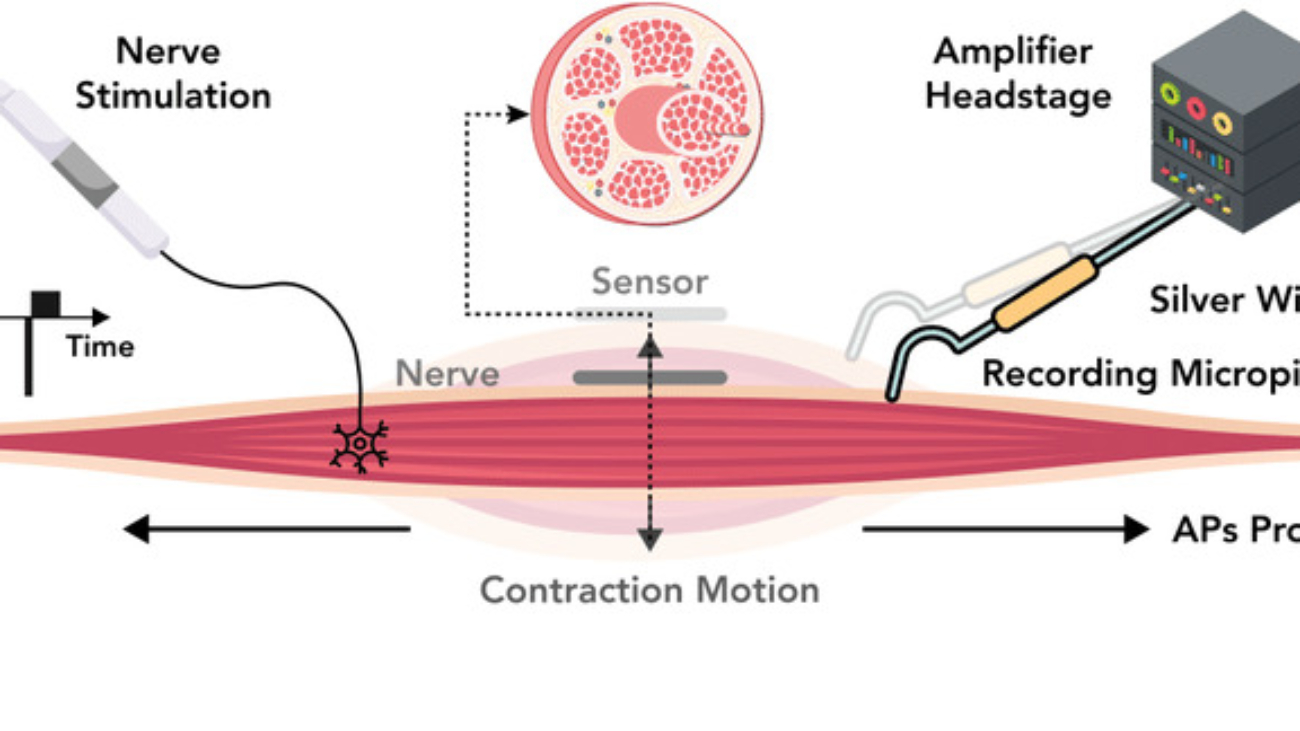
Nerve and muscle physiology is a branch of physiology that specifically studies the function and mechanisms of nervous tissue (nerves) and muscle tissue (muscles).
It explores how these "excitable tissues" generate and transmit electrical signals (like action potentials) and how these electrical signals are converted into specific cellular functions.
It covers how neurons (nerve cells) generate electrical impulses, communicate with each other (synaptic transmission), process information, and transmit signals throughout the body to control various functions, from thought and sensation to movement and organ regulation.
It focuses on how muscle cells (fibers) respond to electrical signals from nerves, leading to contraction (shortening) and the generation of force. This includes the molecular mechanisms of contraction, the regulation of muscle force, and the different types of muscle tissue and their distinct functional characteristics.
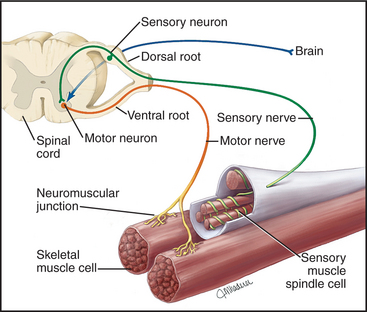
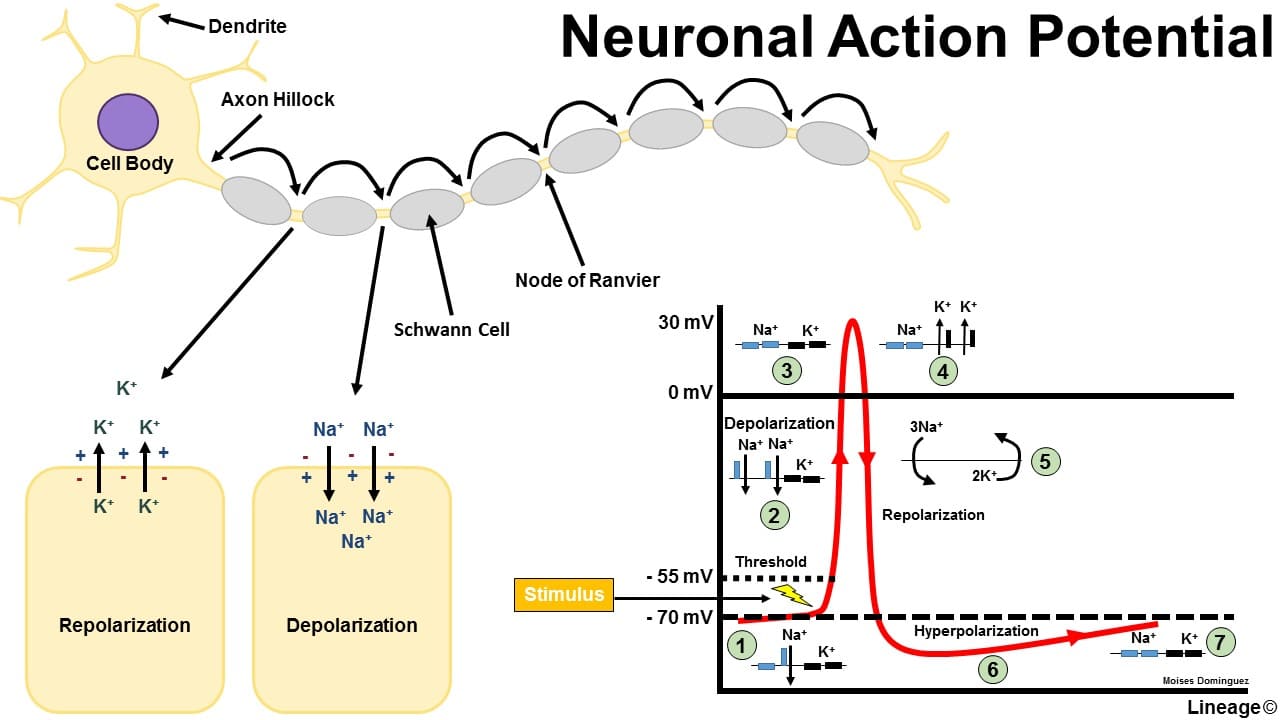
Nervous system excitability is the ability of nerve cells (neurons) to respond to a stimulus by generating and propagating an action potential, a self-propagating electrical impulse.
This property is fundamental to the nervous system's function and depends on the neuron's membrane's selective permeability, ion channels, and pumps. A change in membrane potential can lead to this event, which is essential for transmitting information throughout the body. The physiology of the nervous system involves its main divisions (the Central Nervous System (CNS) and Peripheral Nervous System (PNS)), which use neurons and electrochemical signals to sense stimuli, integrate information, and produce coordinated responses.
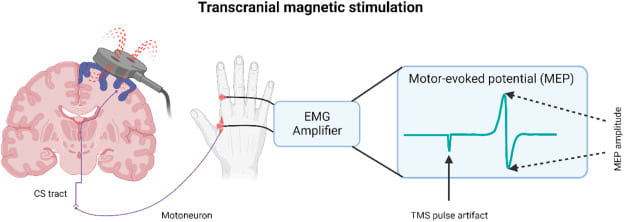
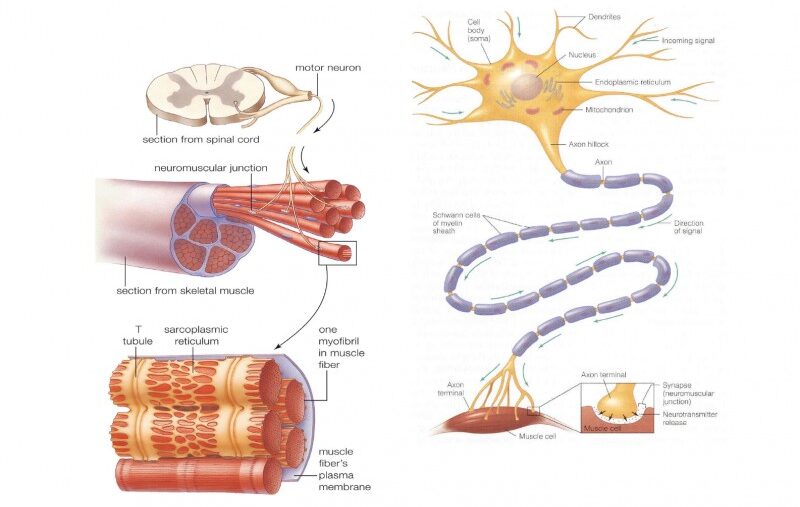
A motor neuron is a specialized nerve cell that transmits electrical signals from the central nervous system (brain and spinal cord) to muscles or glands, thereby initiating movement or secretion. It acts as the "final common pathway" by which the nervous system controls effector organs.
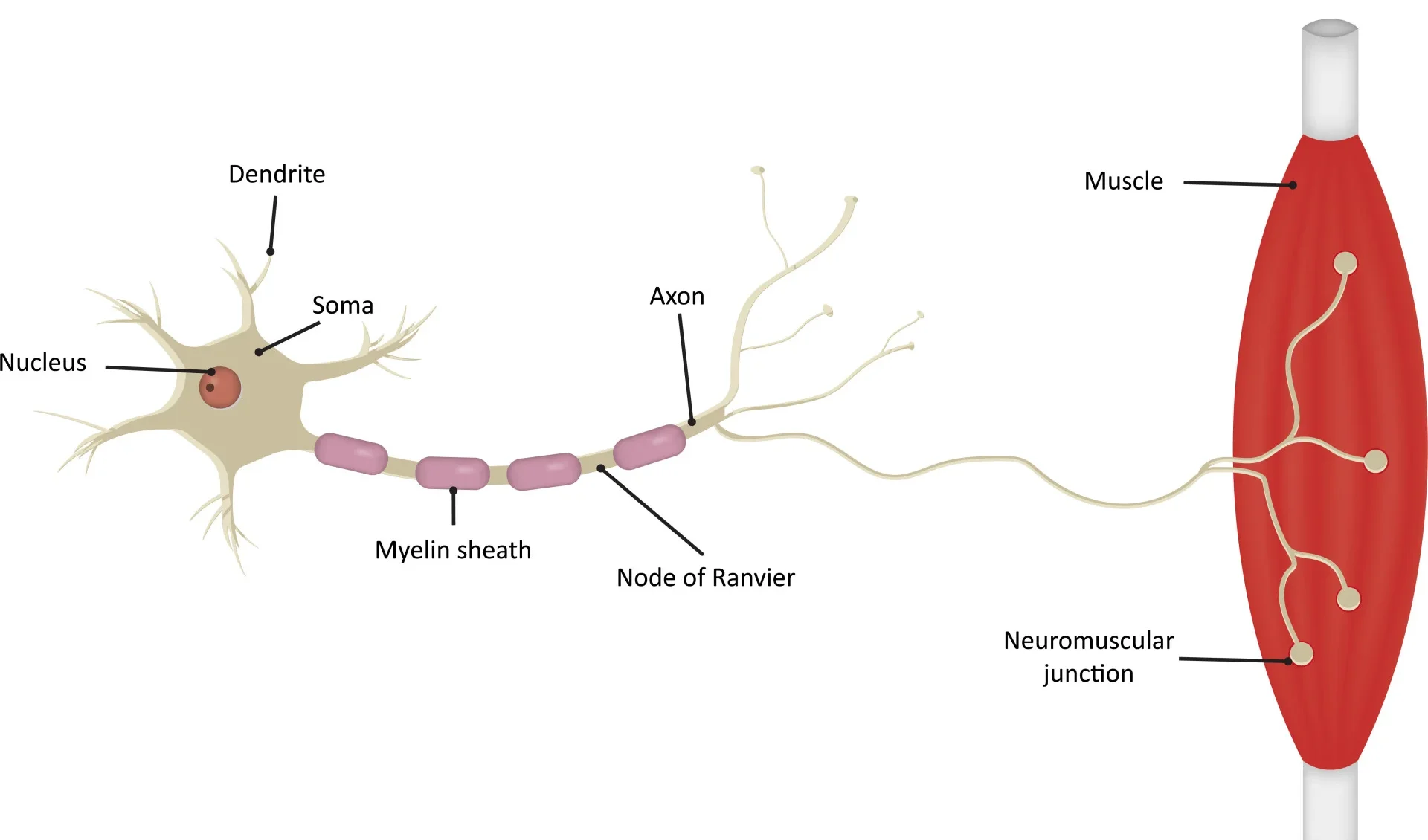
The metabolic center of the neuron, containing the nucleus and other organelles. It synthesizes neurotransmitters and proteins and receives synaptic inputs from other neurons.
Branching, tree-like extensions that are the primary receptive (input) regions. They contain ligand-gated ion channels that receive chemical signals and generate graded potentials (EPSPs and IPSPs).
A cone-shaped region where the axon originates. This is the critical "trigger zone" with the highest density of voltage-gated Na⁺ channels. It integrates all incoming potentials, and if the sum reaches threshold, an action potential is generated.
A single, long projection that transmits the action potential (the output signal) away from the cell body. Its length can exceed a meter.
A fatty, insulating layer that surrounds many axons, formed by Schwann cells in the PNS and oligodendrocytes in the CNS. It is crucial for increasing the speed of action potential conduction.
Gaps in the myelin sheath that contain a high concentration of voltage-gated Na⁺ and K⁺ channels. The action potential is regenerated at these nodes, "jumping" from one to the next in a process called saltatory conduction.
The branched ends of the axon that form synapses with other cells. They contain synaptic vesicles filled with neurotransmitters and are specialized for converting the electrical signal (action potential) into a chemical signal (neurotransmitter release).
We can map these anatomical components to four distinct functional zones, illustrating the flow of information:
Motor neurons are often referred to as the "final common pathway" in motor control. This term emphasizes a fundamental principle: all the complex neural computations happening in higher brain centers (e.g., planning and coordination in the cerebral cortex, basal ganglia, and cerebellum) ultimately converge onto these lower motor neurons.
It is only through the firing of a lower motor neuron that a skeletal muscle can be activated and a movement can occur. Regardless of whether a movement is voluntary or reflexive, the command signal ultimately travels down a lower motor neuron to its target muscle fibers. This makes the motor neuron a critical bottleneck and the ultimate determinant of muscle activity and all bodily movements.
Synaptic transmission is the fundamental process by which one neuron (the presynaptic neuron) communicates with another neuron (the postsynaptic neuron) or an effector cell. Most synapses in the nervous system are chemical synapses, meaning they utilize chemical messengers called neurotransmitters to bridge the microscopic gap between cells.
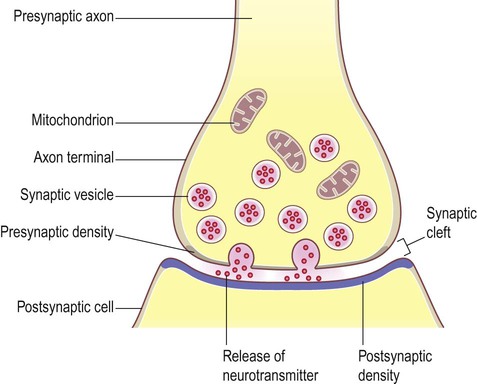
A chemical synapse consists of three main components:
Neurotransmitters are synthesized via distinct pathways and then packaged into synaptic vesicles. This packaging protects them from degradation, concentrates them for efficient release, and ensures their availability.
This phase converts the electrical signal into a chemical signal:
Once in the cleft, neurotransmitters diffuse across and bind reversibly to their specific receptors on the postsynaptic membrane, causing a response.
The receptor itself is an ion channel. Binding of the neurotransmitter causes an immediate opening, allowing ion flow and a rapid change in the postsynaptic membrane potential. This can generate:
The receptor activates an intracellular G-protein, which then initiates a slower but more widespread and long-lasting signaling cascade. This can lead to:
These events generate graded potentials (EPSPs or IPSPs). If the combined effect of these graded potentials at the axon hillock reaches threshold, a new action potential is triggered in the postsynaptic neuron.
To ensure precise and discrete signaling, the action of neurotransmitters must be swiftly terminated. This happens through several mechanisms:
The motor neuron is constantly bombarded with chemical signals from thousands of other neurons. These signals cause small, localized changes in the membrane potential, which the neuron must integrate to decide whether to fire an "all-or-nothing" action potential.
When a presynaptic neuron releases neurotransmitters, they bind to ligand-gated ion channels on the motor neuron, leading to a change in its membrane potential.
A depolarization of the postsynaptic membrane, making it less negative and more likely to fire. Typically caused by the influx of positive ions, most commonly Na⁺, when an excitatory neurotransmitter (e.g., glutamate) binds.
A hyperpolarization or stabilization of the membrane potential, making it more negative and less likely to fire. Typically caused by the influx of negative ions (Cl⁻) or the efflux of positive ions (K⁺) when an inhibitory neurotransmitter (e.g., GABA, glycine) binds.
A single EPSP is usually too weak to trigger an action potential. Motor neurons integrate thousands of inputs:
The axon hillock acts as the integrator. If the algebraic sum of all incoming EPSPs and IPSPs reaches the threshold potential (typically around -55 mV), an action potential is generated.
Once generated at the axon hillock, the action potential propagates along the axon without losing strength.
Muscle tissue is specialized for contraction, generating force and movement. Here, we'll focus on skeletal muscle.
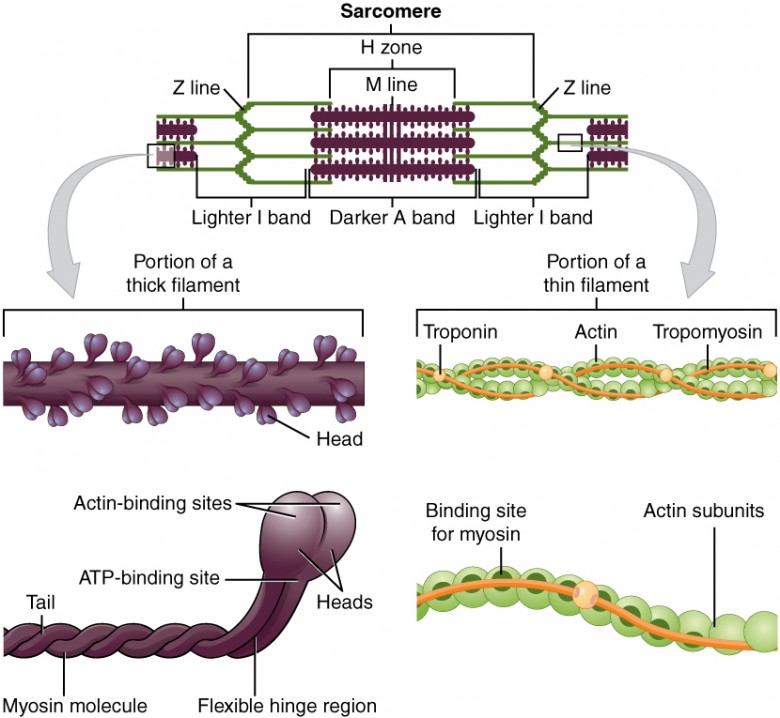
The sarcomere is the fundamental, repeating contractile unit of a myofibril, extending from one Z-disc to the next.

The neuromuscular junction (NMJ) is the specialized chemical synapse where a motor neuron's axon terminal meets a skeletal muscle fiber.
This is the muscle's initial, graded electrical response at the motor end plate:
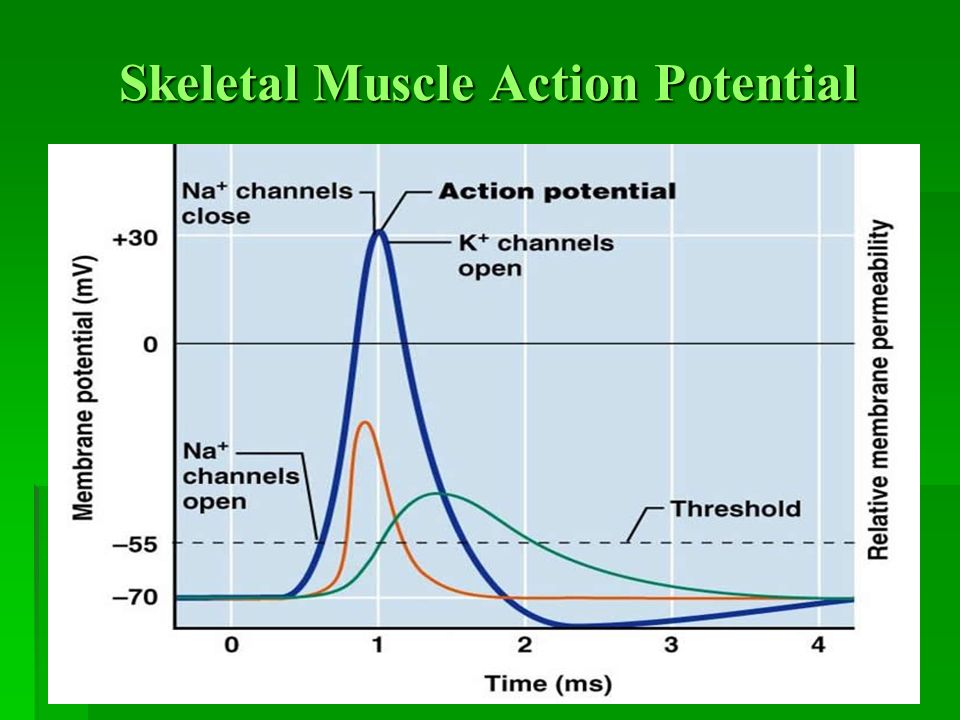
The muscle action potential is an "all-or-nothing" electrical signal that rapidly spreads across the entire muscle fiber membrane. Its characteristics are very similar to the neuronal action potential, but its purpose is specifically to initiate muscle contraction.
The muscle action potential propagates in two critical ways:
This is the physiological process by which an electrical signal (the muscle action potential) is converted into a mechanical event (muscle contraction).
The Sliding Filament Theory proposes that muscle shortening occurs by the thick and thin filaments sliding past one another, thereby increasing their overlap.
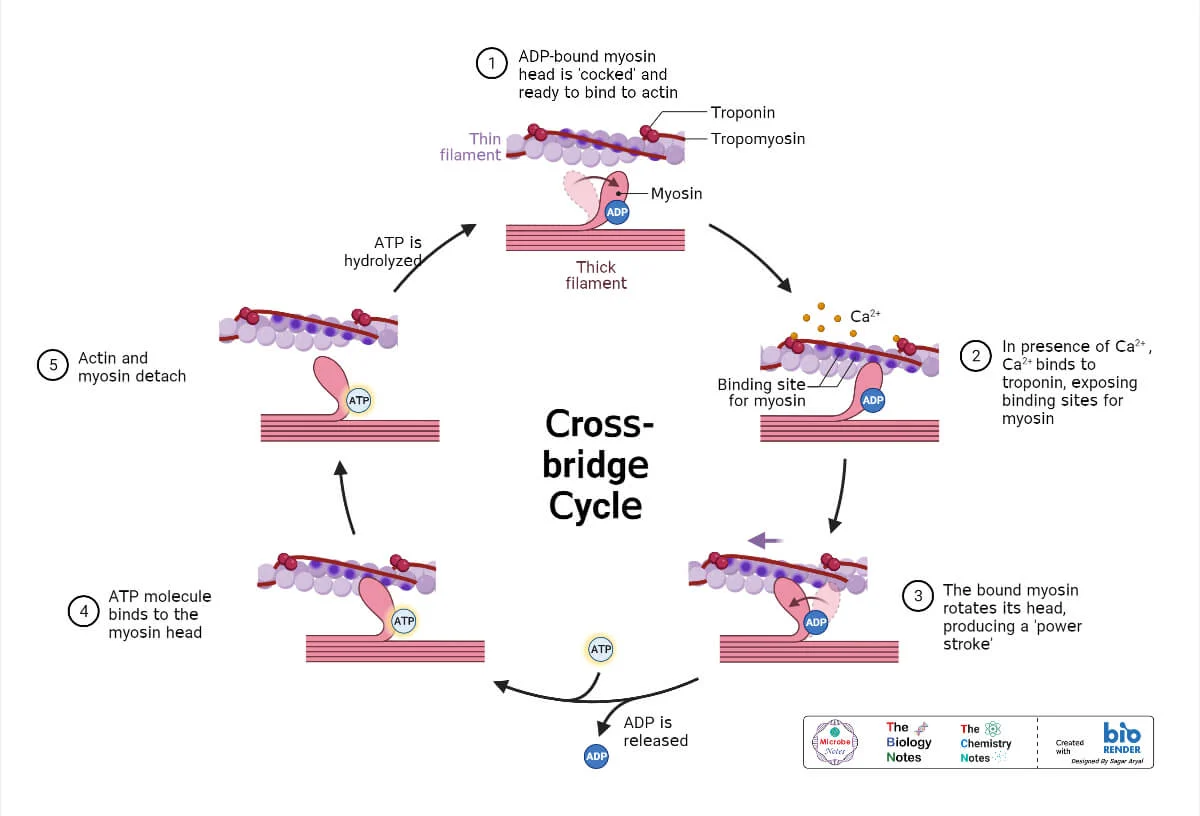
The cross-bridge cycle is a repetitive series of events that causes the thin filaments to slide over the thick filaments.
The energized ("cocked") myosin head, which is already holding onto ADP and inorganic phosphate (Pi) from the previous cycle, has a strong chemical attraction (affinity) for the actin filament. This binding can only occur if the myosin-binding sites on the actin are exposed. Once the sites are uncovered by the movement of tropomyosin (triggered by Ca²⁺ binding to troponin), the myosin head immediately forms a strong physical link with the actin. This connection is the "cross-bridge."
The formation of the cross-bridge triggers the release of the inorganic phosphate (Pi) from the myosin head. This release unleashes the stored energy, causing the myosin head to pivot forcefully from its high-energy 90° angle to a low-energy 45° angle. This pivotal movement is the power stroke. Because it is firmly attached, the myosin head drags the entire thin filament a short distance (~10 nm) toward the center of the sarcomere. Immediately after the pivot, the ADP molecule is also released, leaving the myosin head in a low-energy state, still tightly bound to actin.
After the power stroke, the myosin head is "stuck" to the actin in a low-energy state (the "rigor" state). The only way for it to let go is for a new molecule of ATP to bind to the ATP-binding site on the myosin head. This binding causes a conformational change that weakens the bond between myosin and actin, reducing their affinity for each other and causing the myosin head to detach. Without a fresh supply of ATP, this detachment cannot occur, which is the molecular basis for the muscle stiffness seen in rigor mortis after death.
The myosin head, now with ATP bound, immediately acts as an enzyme (myosin ATPase) and hydrolyzes the ATP back into ADP and inorganic phosphate (Pi). The energy released from breaking this ATP bond is captured by the myosin head and used to change its shape, moving it from its low-energy bent position back to its high-energy, upright, "cocked" position. It is now energized and reset, ready to begin the cycle again by binding to another active site further down the actin filament (if Ca²⁺ is still present).
Repeated cycles of the cross-bridge cycle cause:
When thousands of sarcomeres shorten simultaneously, the entire muscle shortens and generates force.
Muscle relaxation is an active, energy-requiring process.
Excitability: The Ability to Respond and Communicate
Excitability refers to the ability of a cell to respond to a stimulus by generating an electrical signal called an action potential. It can be defined as a physical chemical change that occurs when a stimulus is applied on a tissue. A stimulus is an external agent that produces excitation in a tissue. This electrical signal is then propagated along the cell membrane or transmitted to other cells, leading to a specific physiological response.
The action potential is a transient, rapid, and self-propagating reversal of the electrical potential across the cell membrane. This electrical signal is the medium through which cells rapidly transmit information, either along the length of an individual cell or to other cells via specialized junctions. This property is crucial for rapid communication and coordination within the body, underpinning virtually every complex physiological function, from perception and thought to movement and visceral regulation.
Think of an excitable cell like a highly sensitive electrical tripwire or alarm system. The resting state is the armed system waiting for a trigger. The stimulus is the pressure that activates the tripwire. The action potential is the immediate, swift, and uniform "alarm bell" that rings loudly and clearly, sending its message through the system to orchestrate a coordinated response.
While all living cells exhibit some degree of responsiveness, only a select group possess the highly specialized machinery to generate and propagate rapid electrical signals. These are the "excitable cells."
Expanded Role: Neurons are the fundamental units of the nervous system. Their primary function is the transmission of electrical and chemical signals for sensory input, integration, motor output, cognition, and emotion.
Unique Features: They possess specialized structures like dendrites (to receive signals), a cell body (soma), and a long axon (to transmit signals), often insulated by a myelin sheath to speed conduction.
Muscle cells are specialized for contraction, which generates force and movement. Their excitability is the prerequisite for this mechanical action.
Responsible for all voluntary movements (walking, speaking, breathing). When a motor neuron sends an action potential, it triggers a muscle action potential, leading to contraction.
Found only in the heart, responsible for the rhythmic and involuntary pumping of blood. They possess autorhythmicity and have distinctively long action potentials for coordinated contractions.
Mediate involuntary movements in the walls of internal organs like the digestive tract, blood vessels, and urinary bladder. Their excitability is influenced by stretch, local chemicals, and the autonomic nervous system.
Role Expansion: Many glandular cells (e.g., in the adrenal medulla, pancreas) exhibit excitability. They can respond to an electrical stimulus from a neuron by generating their own electrical event (depolarization or action potential).
Excitability Link: This electrical event is typically coupled to the release of their secretions (e.g., hormones, digestive enzymes). For example, adrenal medullary cells depolarize in response to a neuronal signal, triggering Ca²⁺ influx and the exocytosis of epinephrine. This ensures precise and rapid control over hormone release.
The capacity of these cells to generate electrical signals rests entirely on the idea of membrane potential.
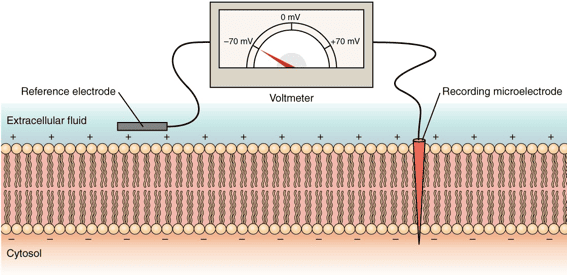
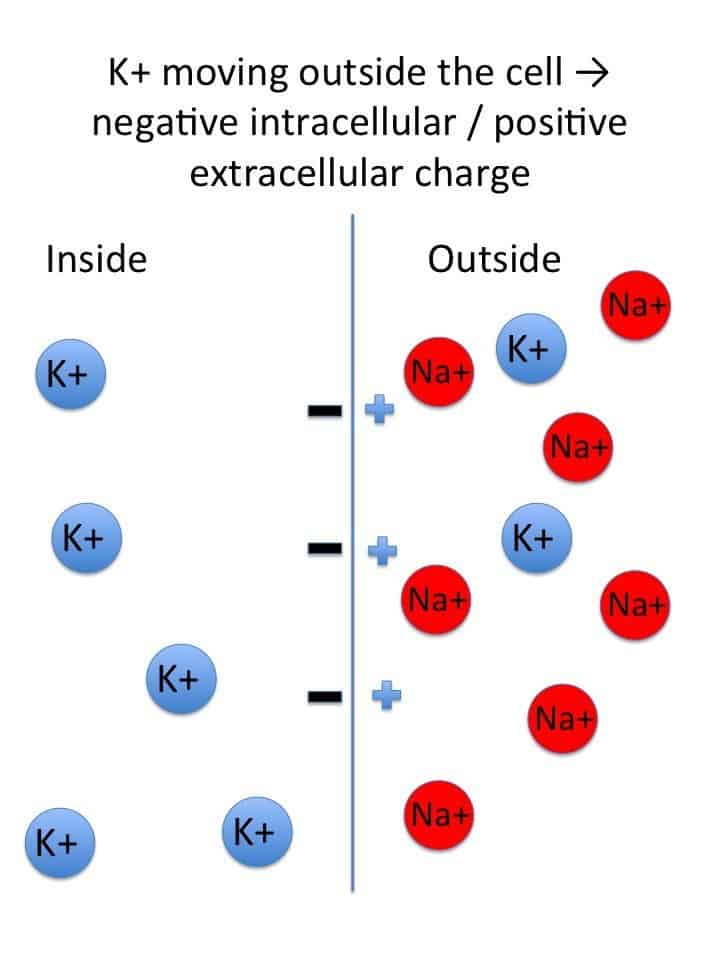
This is the voltage difference across the cell's outer boundary, a stored electrical energy created by an uneven distribution of ions (electrically charged particles) inside the cell (ICF) and outside the cell (ECF).
When an excitable cell is quiet, it maintains a stable, baseline electrical charge called the Resting Membrane Potential (RMP). In this state, the inside of the cell consistently holds a negative charge relative to the outside (e.g., -70 mV in neurons, -90 mV in skeletal muscle).
The RMP is a dynamic state, constantly maintained by an interplay of three factors:
The equilibrium potential for a specific ion is the membrane voltage at which there is no net movement of that ion across the membrane. At this voltage, the electrical force is perfectly balanced by the chemical (concentration) force. The Nernst Equation calculates this value:
E_ion = (RT / zF) * ln([ion]out / [ion]in)
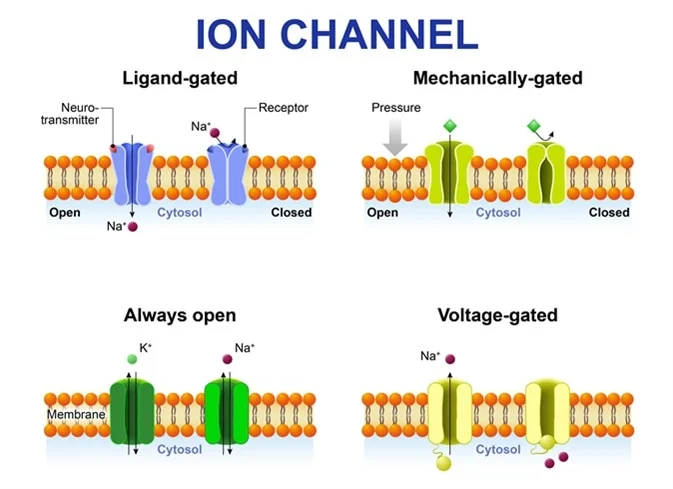
These are specialized proteins that form pores for specific ions to cross the membrane.
These channels open or close only in response to a particular trigger and are essential for generating action potentials.
Open or close in direct response to changes in membrane voltage. They are the key drivers of the action potential.
Open or close when a specific chemical messenger (a ligand), such as a neurotransmitter, binds to them.
Open or close when they are physically deformed or stretched, critical for sensory perception like touch and pressure.
A stimulus is any detectable change (electrical, chemical, or mechanical) in the cell's environment that has the potential to alter its RMP.
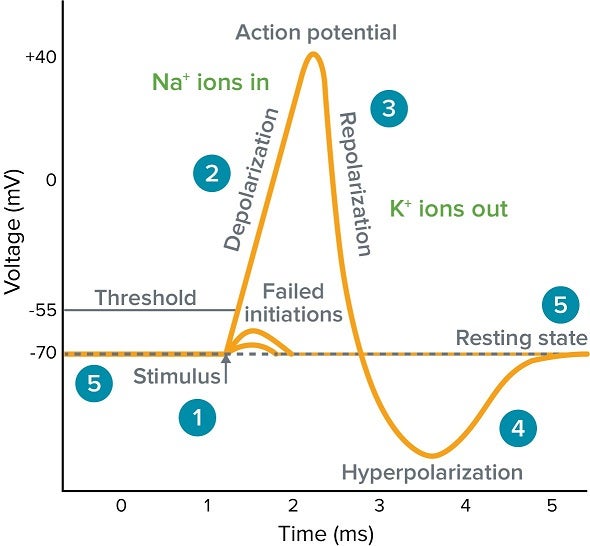
Threshold is the crucial voltage level that depolarization must reach for an action potential to fire (typically around -55 mV in neurons). It is an "all-or-none" event: if a stimulus causes a depolarization that reaches threshold, a full action potential fires. If it does not, nothing happens.
The action potential is the primary electrical signal employed by excitable cells to swiftly transmit information across significant distances. It stands as an "all-or-nothing" phenomenon: once initiated, it proceeds through its entire sequence with consistent strength, never diminishing.
All voltage-gated Na⁺ and K⁺ channels are closed. The RMP is maintained by K⁺ leak channels and the Na⁺/K⁺ pump.
A local stimulus causes a few voltage-gated Na⁺ channels to open, allowing a small amount of Na⁺ to enter. If enough Na⁺ enters to raise the membrane potential to the threshold level, an action potential is triggered.
Once threshold is reached, a vast number of voltage-gated Na⁺ channels open very rapidly. A massive and swift surge of Na⁺ into the cell causes the inside of the membrane to become positive.
At the peak, the voltage-gated Na⁺ channels inactivate (their inactivation gates close), stopping Na⁺ influx. Simultaneously, the slower voltage-gated K⁺ channels are now fully open, allowing a significant outflow of K⁺, which rapidly restores the membrane's negative charge.
The voltage-gated K⁺ channels close slowly, allowing K⁺ to continue exiting for a brief period. This causes the membrane to become temporarily more negative than the RMP.
The slow K⁺ channels finally close, and the ever-active Na⁺/K⁺ pump helps to re-establish the original ion concentration gradients, returning the membrane to its stable RMP.
The electrical shift at one point on the membrane triggers the opening of voltage-gated Na⁺ channels in the immediately adjacent area. This process repeats, moving the signal along the length of the nerve or muscle fiber.
Many nerve fibers are insulated by a fatty myelin sheath. Action potentials therefore appear to "jump" from one uninsulated gap (a node of Ranvier) to the next. This rapid "jumping" process is termed saltatory conduction and dramatically increases the signal's speed.
To truly appreciate the dynamics of body fluids, we first need to understand where all this fluid is located within the body. Imagine your body as a system of interconnected containers, each holding a specific type of fluid. These "containers" are what we call body fluid compartments.
The human body is largely composed of water, and this water isn't just free-flowing; it's meticulously organized into various functional compartments. This compartmentalization is key to maintaining cellular and systemic homeostasis.
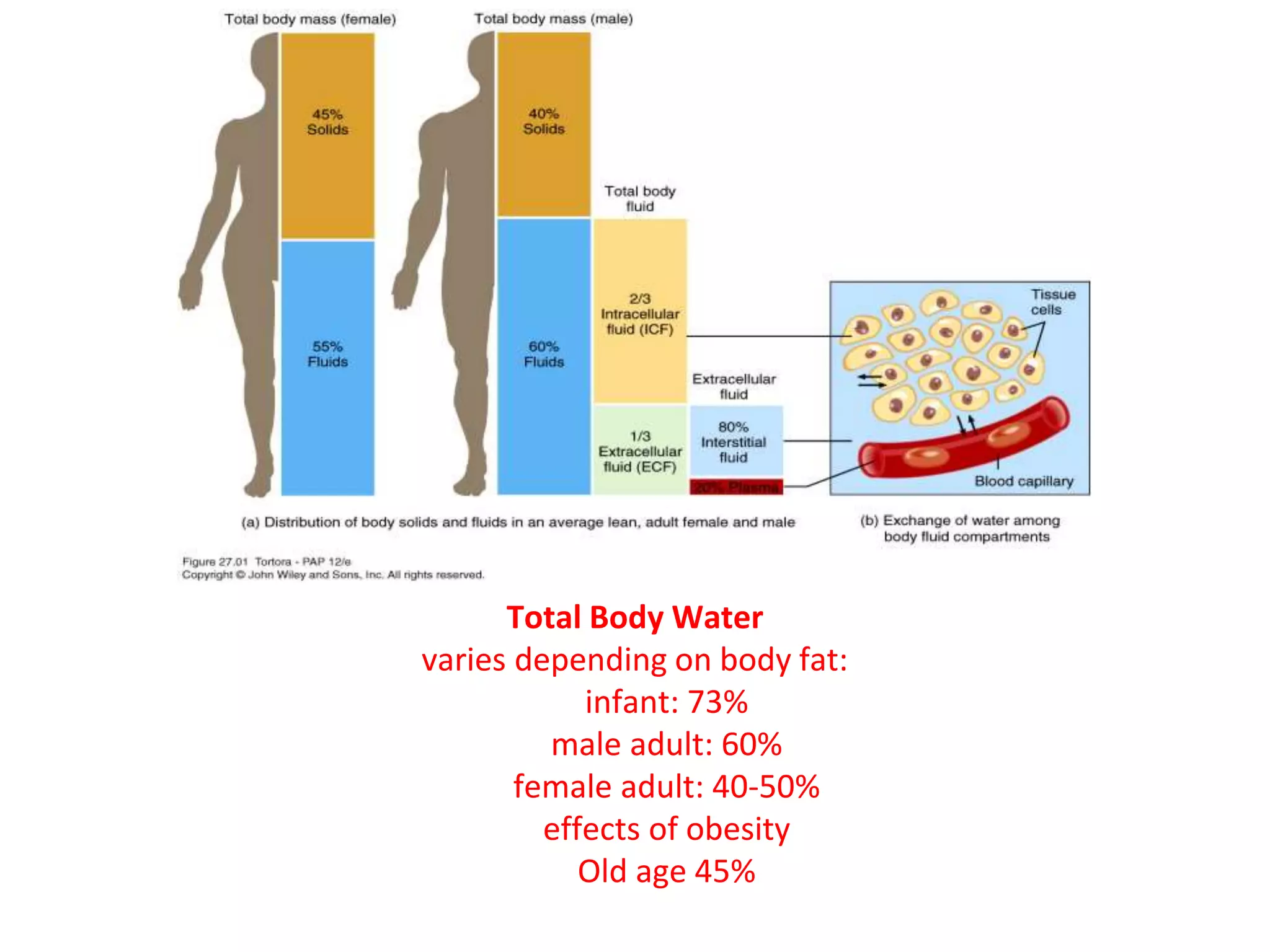
TBW refers to all the water contained within the body. It represents a significant proportion of body mass.
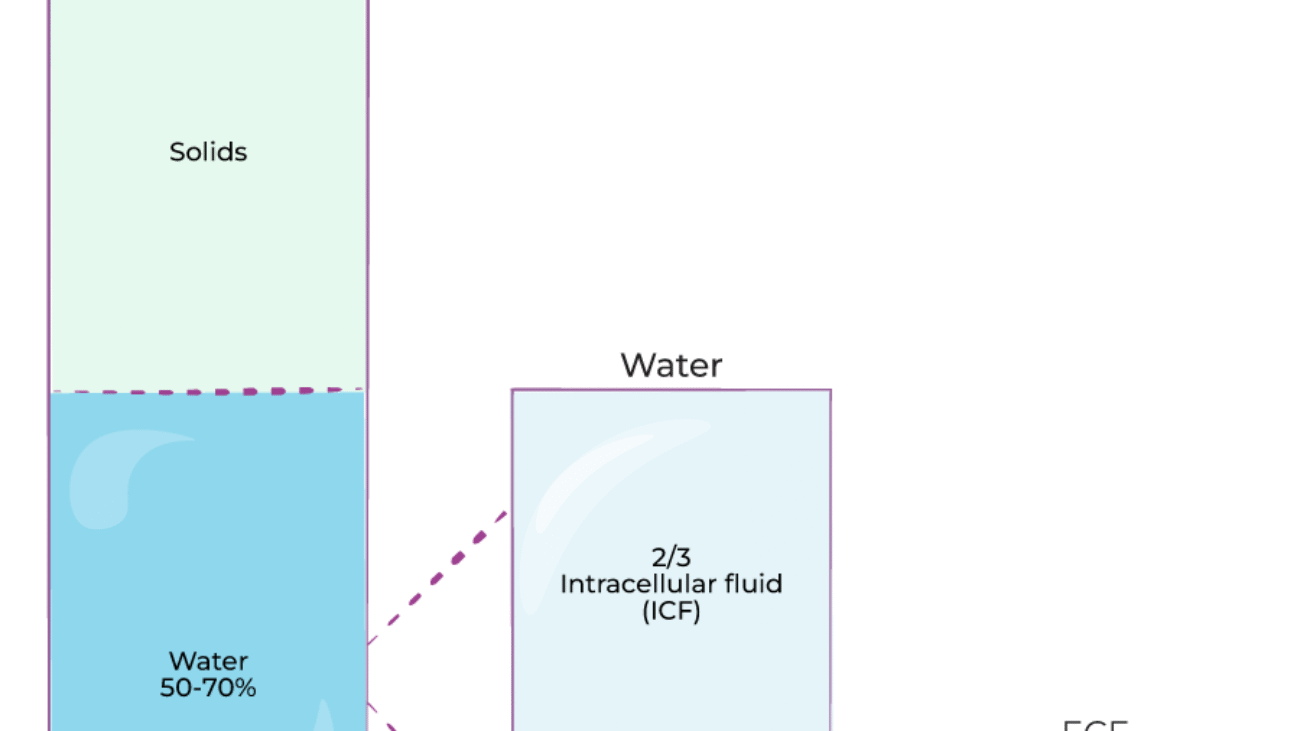
Approximately 60% of an adult's body weight is water. This percentage can vary significantly based on several factors:
TBW is not pure water; it contains numerous dissolved solutes, including electrolytes, proteins, nutrients, gases, and waste products. The total amount of water in an adult human body constitutes about 50-70% of the total body weight. This water is not uniformly distributed but is divided into two primary compartments, which are further subdivided:
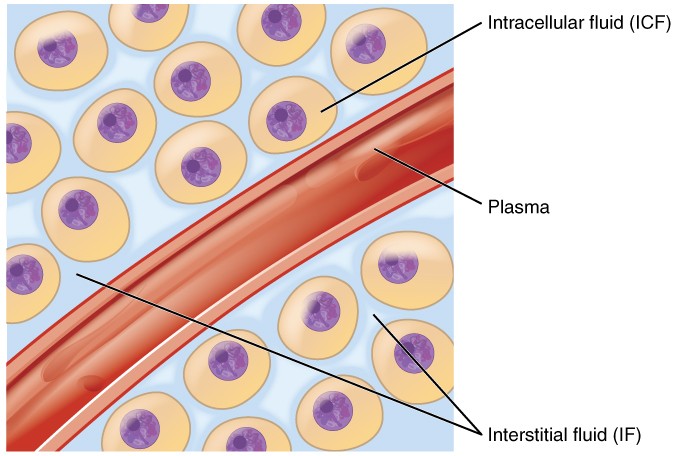
Location: The ICF is the fluid found within the cells of the body. It is the immediate environment where the vast majority of cellular metabolic activities take place.
Proportion and Significance: The ICF constitutes the largest single fluid compartment, accounting for approximately two-thirds (2/3) of the Total Body Water (TBW). In an adult male weighing 70 kg, this would be roughly 28 liters (40% of body weight). This large volume underscores its critical role: it directly bathes the cellular machinery, providing the aqueous medium for all intracellular biochemical reactions.
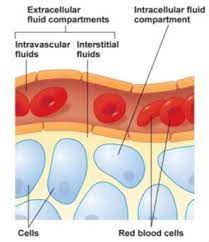
Location: The ECF is all the fluid found outside the cells. It acts as the body's internal environment that bathes all cells.
Proportion: The ECF constitutes approximately one-third (1/3) of the TBW, which is roughly 14 liters (20% of body weight) in a 70 kg adult.
The ECF is not a monolithic entity; it is further subdivided into several distinct yet interconnected compartments:
This is the "tissue fluid," filling the microscopic spaces between the cells. It is the largest component of the ECF, comprising about 80% of ECF volume. Its ionic composition is similar to plasma, but it has a significantly lower protein concentration. The ISF is the critical medium for the exchange of nutrients, gases, and waste between the blood and the cells.
This is the fluid component of blood, circulating within the cardiovascular system. It accounts for about 20% of ECF volume. Its defining characteristic is its high concentration of plasma proteins (e.g., albumin). Plasma is the primary transport medium for blood cells, nutrients, hormones, and waste products.
A small, specialized component of the ECF, representing only 1-2% of body weight. It consists of fluids secreted by specific cells into distinct, epithelial-lined spaces. The composition of these fluids is often unique and tailored to their specific function.
Examples: Cerebrospinal Fluid (CSF), Intraocular Fluid, Synovial Fluid, Serous Fluids (pleural, pericardial), and Gastrointestinal Secretions.
The precise movement of water and solutes between the body's fluid compartments is a cornerstone of physiological homeostasis. This dynamic equilibrium is meticulously regulated by physical forces, membrane properties, and complex neurohormonal systems.
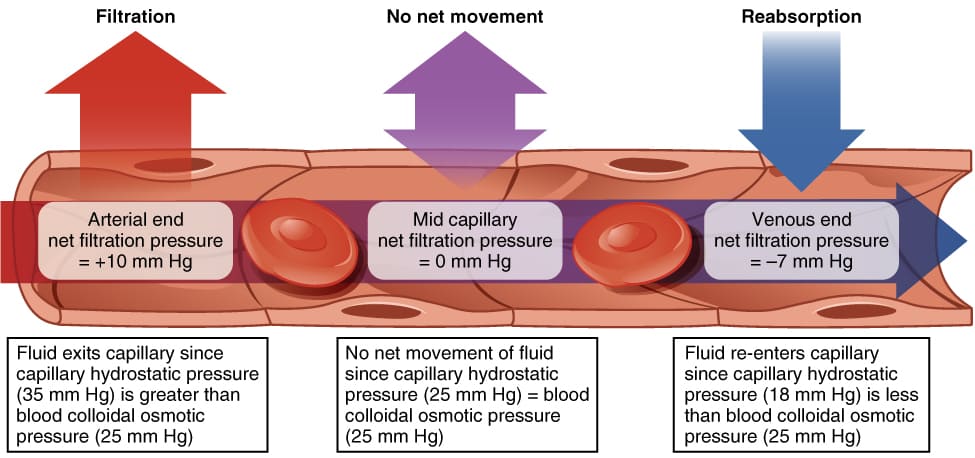
The exchange of fluid, nutrients, gases, and waste products between the blood (plasma) and the cells (via the ISF) occurs primarily across the thin walls of the capillaries. This movement is governed by Starling Forces, which represent the interplay of hydrostatic and oncotic pressures.
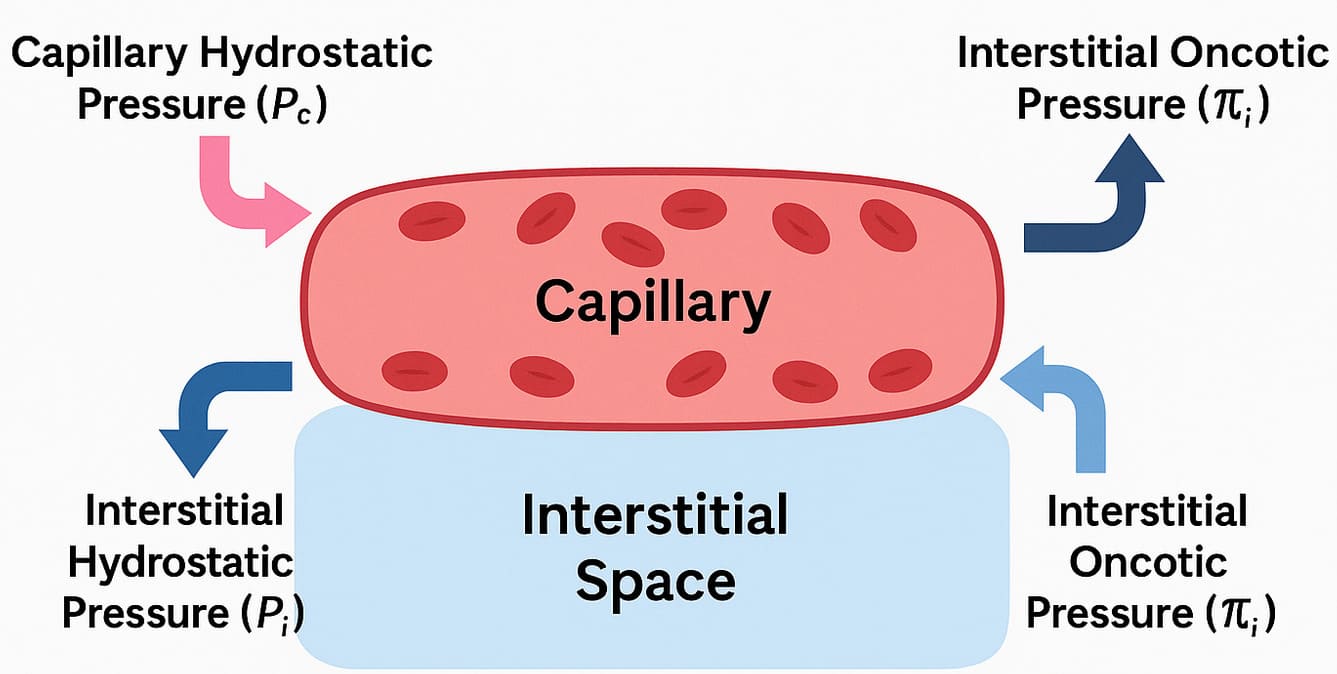 Starling Forces - The Drivers of Capillary Exchange:
Starling Forces - The Drivers of Capillary Exchange:The net movement of fluid is determined by the balance of these forces, expressed by the Starling equation: NFP = (Pc - Pif) - (πc - πif)
There is a slight imbalance where filtration slightly exceeds reabsorption. This excess fluid and any leaked proteins are collected by the lymphatic system, which acts as a drainage system, returning this "lymph" to the circulation. This is vital for preventing interstitial edema. Failure of this system results in lymphedema.
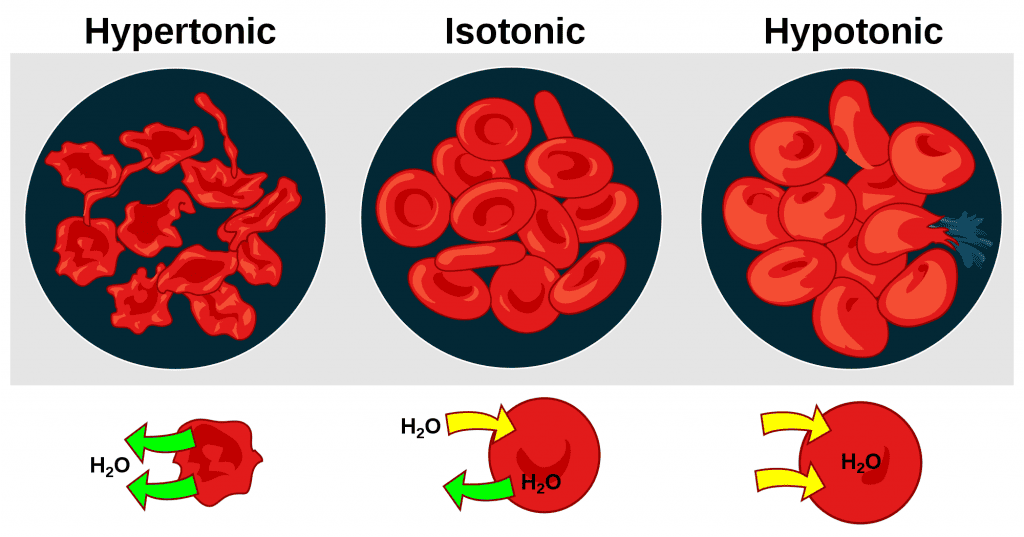
The exchange between the ISF and the ICF is driven primarily by osmosis. The cell membrane is highly permeable to water (largely via aquaporins) but relatively impermeable to most solutes.
Tonicity describes the effect a solution has on cell volume, based on its concentration of non-penetrating solutes.
While water movement is passive, the maintenance of the osmotic gradients is dependent on active transport. The Na⁺/K⁺ ATPase pump is critical. By constantly pumping 3 Na⁺ out and 2 K⁺ in, it counters the natural tendency of water to enter the cell (due to the high concentration of trapped intracellular proteins), thereby maintaining cell volume and preventing lysis.
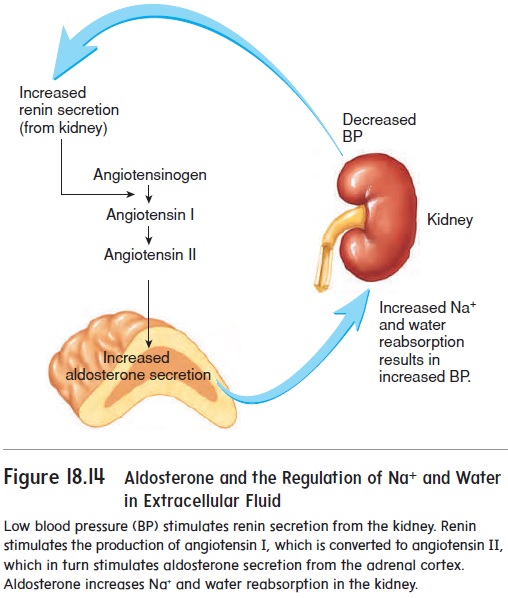
This is achieved through complex, interconnected neurohormonal feedback systems.
ECF volume is primarily determined by its sodium content, as "where Na⁺ goes, water follows."
ECF osmolarity is primarily determined by the concentration of solutes relative to water, and is tightly controlled to stay within 280-300 mOsm/L.
Disturbances in fluid regulation can have profound and life-threatening consequences.
The volume of a compartment is calculated as: Volume = Mass of Indicator Injected / Concentration of Indicator in Sample. The key is choosing an indicator that distributes only in the target compartment.
The human body is an intricate system highly dependent on the precise balance of water and solutes across its various compartments. Understanding the concepts of osmolarity and tonicity, and their clinical implications, particularly with intravenous (IV) fluid administration, is fundamental to effective medical practice.
These two terms are often used interchangeably, but they possess distinct physiological meanings that are critical when considering fluid shifts across cell membranes.
A solution can be isosmotic but hypotonic. A classic example is 5% Dextrose in Water (D5W). Initially, its osmolarity is ~252 mOsm/L (isosmotic). However, once cells metabolize the glucose, it leaves behind pure water, which is hypotonic to cells, causing water to shift into them. Therefore, tonicity, not just osmolarity, is what truly matters for predicting cell volume changes.
Their safe and effective administration requires a deep understanding of their tonicity and how they distribute.
Products like packed red blood cells (PRBCs) are considered isotonic. Their distribution primarily expands the intravascular compartment (plasma volume) and directly increases the oxygen-carrying capacity of the blood.
| IV Fluid Type | Tonicity | Final Distribution | Effect on Cells | Primary Clinical Use |
|---|---|---|---|---|
| Isotonic | Isotonic | Expands ECF (Plasma + ISF) | No change | ECF volume expansion (shock, dehydration) |
| Hypotonic | Hypotonic | Shifts from ECF to ICF | Swell | Cellular rehydration (hypernatremia) |
| Hypertonic | Hypertonic | Shifts from ICF to ECF | Shrink | Reduce cerebral edema, treat severe hyponatremia |
| Colloids | Isotonic | Primarily remains in Plasma | No change | Plasma volume expansion (severe shock) |
| Blood Products | Isotonic | Primarily remains in Plasma | No change | Replace blood loss, improve O₂ carrying capacity |
At the heart of all physiological processes involving fluids is the interaction between solutes and solvents, and their movement across various compartments.
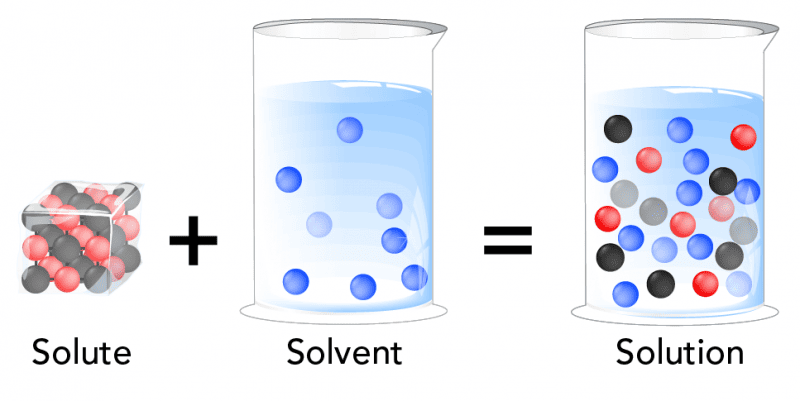
The primary and overwhelmingly abundant solvent in all body fluids is WATER (H₂O).
Water's unique properties make it an ideal biological solvent:
Body fluids are complex solutions containing a vast array of solutes:
The movement of substances is primarily governed by passive processes that do not require cellular energy (ATP).
These passive movements are essential for: