TOPOGRAPHY OF THE CENTRAL NERVOUS SYSTEM (CNS)
The Nervous System (N/S) is indeed the most complex and highly organized system in the body, responsible for integrating and coordinating nearly all bodily functions.
- Master Control System: It acts as the body's primary communication and control center.
- Coordination with Endocrine System: It works in close conjunction with the endocrine system (hormonal system) to achieve this coordination.
- Nervous System: Functions via rapid electrical impulses transmitted along specialized cells called neurons, leading to immediate, short-lived responses.
- Endocrine System: Functions via slower-acting chemical messengers (hormones) transported through the bloodstream, leading to more widespread and longer-lasting effects.
- Neuroendocrinology: There's significant overlap, with specialized neurons (neurosecretory cells) releasing hormones, and hormones influencing neuronal activity. The hypothalamus, for example, is a crucial bridge between these two systems.
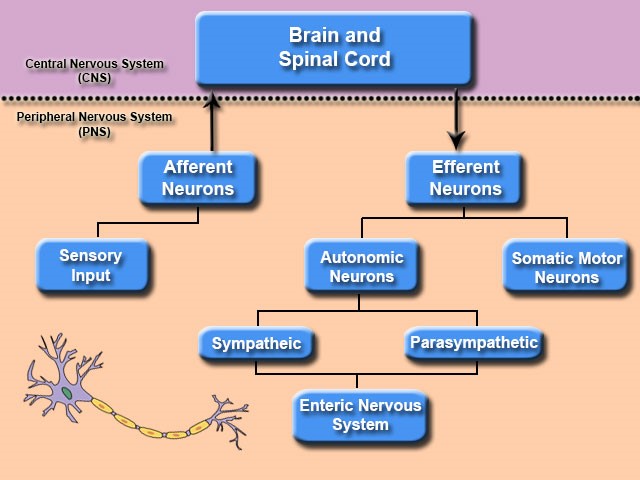
Functional Organization of the Nervous System
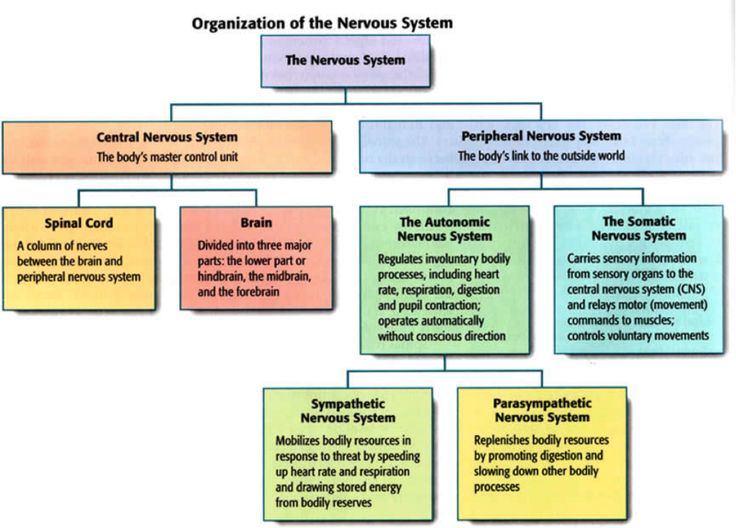
The Nervous System is broadly divided into two main functional components, based on the type of control they exert:
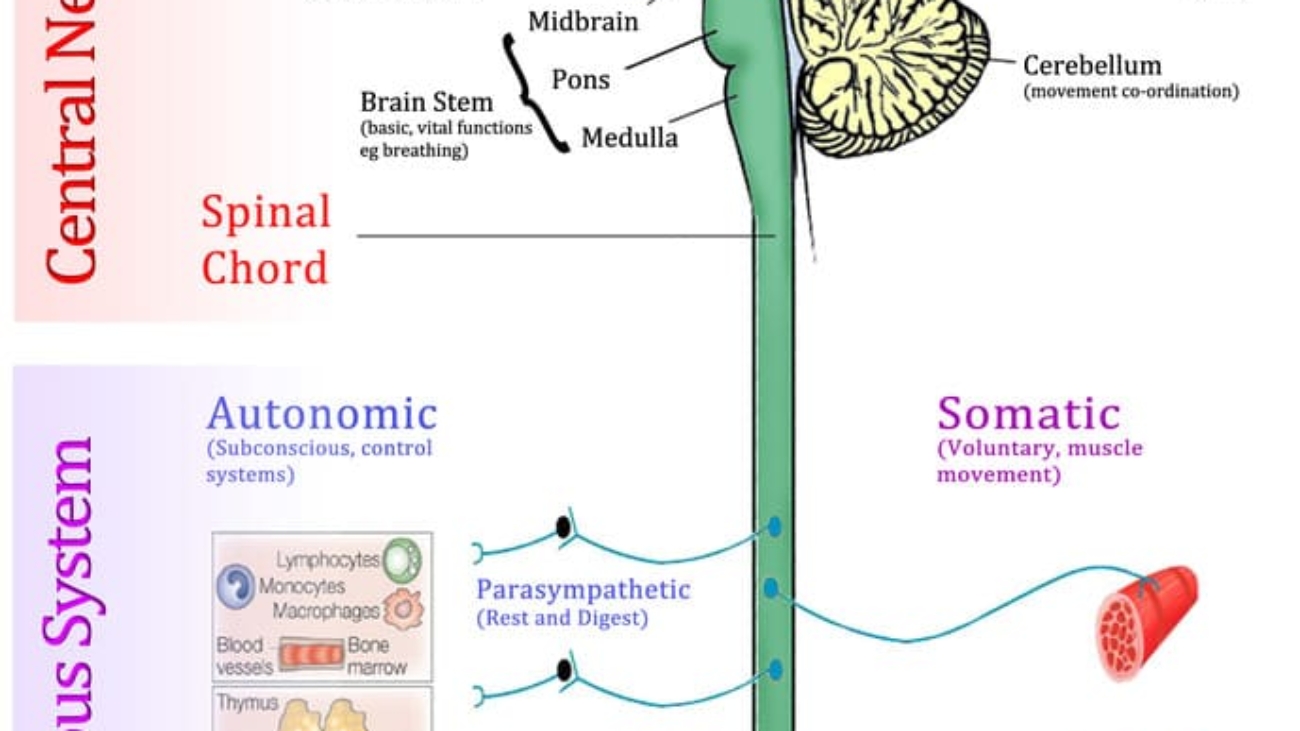
1. Somatic Nervous System (SNS)
- Control: Primarily controls voluntary functions of the body.
- Effectors: Targets skeletal muscles, allowing for conscious movement, posture maintenance, and reflexes.
- Sensory Input: Receives sensory information from the skin, muscles, joints, and special senses (sight, hearing, touch, taste, smell).
- Pathway: Typically involves a single motor neuron extending from the CNS directly to the skeletal muscle.
2. Autonomic Nervous System (ANS)
- Control: Regulates involuntary (visceral) functions of the body, largely operating unconsciously.
- Effectors: Targets smooth muscle (e.g., in walls of organs, blood vessels), cardiac muscle (heart), and glands (e.g., salivary, sweat, digestive).
- Sensory Input: Receives sensory information from internal organs (viscera).
- Pathway: Involves a two-neuron chain to reach the effector organ: a preganglionic neuron (originating in the CNS) and a postganglionic neuron (originating in a ganglion outside the CNS).
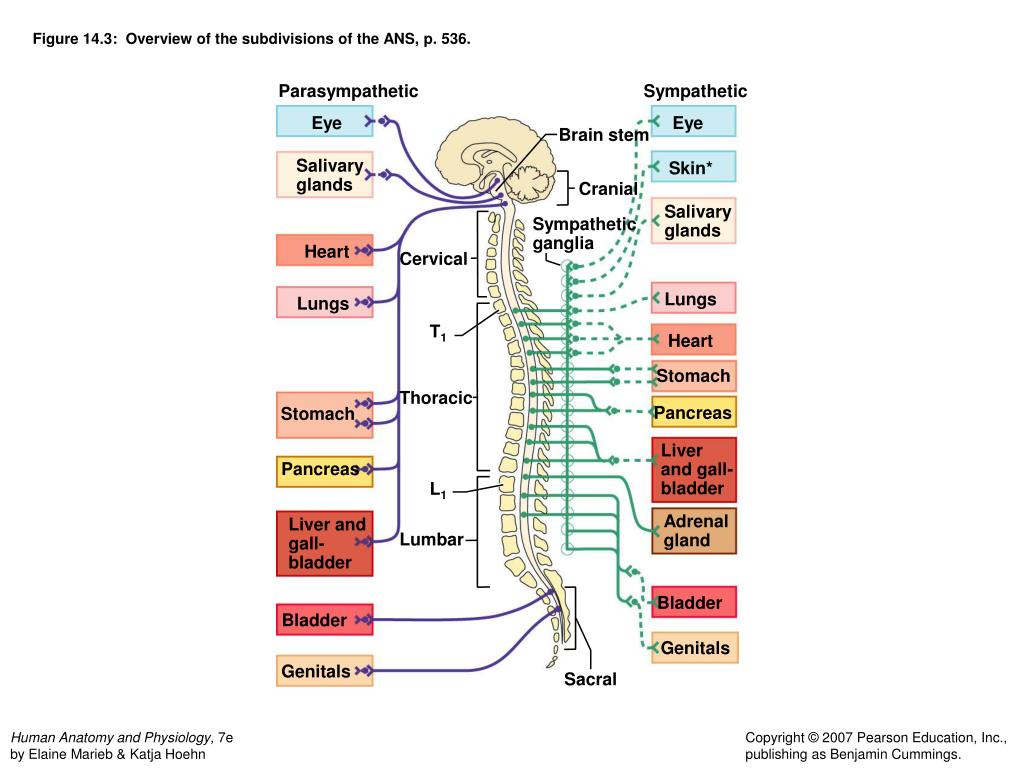
- Subdivisions: The ANS is further subdivided into two main antagonistic branches: the Sympathetic Nervous System and the Parasympathetic Nervous System.
Somatic versus Autonomic Organization: Key Differences Summarized
| Feature | Somatic Nervous System (SNS) | Autonomic Nervous System (ANS) |
|---|---|---|
| Control | Voluntary | Involuntary (visceral) |
| Effectors | Skeletal muscles | Smooth muscle, cardiac muscle, glands |
| Consciousness | Conscious perception and control | Generally unconscious control |
| Number of Neurons | One motor neuron from CNS to effector | Two-neuron chain: preganglionic (CNS) and postganglionic (ganglion) to effector |
| Neurotransmitter | Acetylcholine at neuromuscular junction | Acetylcholine (preganglionic) and Norepinephrine or Acetylcholine (postganglionic) |
| Myelination | Motor neurons are heavily myelinated | Preganglionic are myelinated; Postganglionic are unmyelinated |
| Target Response | Excitation (muscle contraction) | Excitation or Inhibition (depending on target organ and receptor type) |
Subdivisions of the Autonomic Nervous System
The sympathetic and parasympathetic divisions typically act in opposition to each other to maintain homeostasis, like an accelerator and a brake, respectively.
1. The Sympathetic Nervous System (SNS): "Fight or Flight"
- Origin (Thoraco-lumbar Division): Preganglionic neurons originate from the lateral horns of the spinal cord gray matter in segments T1 through L2 (or L3).
- Ganglia:
- Paravertebral Chain Ganglia (Sympathetic Trunk): These are a series of interconnected ganglia located on either side of the vertebral column. Most preganglionic fibers synapse here.
- Prevertebral (Collateral) Ganglia: Located more anteriorly, closer to the abdominal aorta and its major branches (e.g., celiac ganglion, superior mesenteric ganglion, inferior mesenteric ganglion). Some preganglionic fibers pass through the paravertebral ganglia without synapsing and instead synapse in these prevertebral ganglia.
- Neurotransmitters:
- Preganglionic fibers: Release acetylcholine (ACh) at the ganglion (nicotinic receptors).
- Postganglionic fibers: Primarily release norepinephrine (NE) (also known as noradrenaline) at the target organ (adrenergic receptors).
- Exception: Sympathetic postganglionic fibers to sweat glands release ACh. Also, the adrenal medulla acts as a modified sympathetic ganglion, releasing epinephrine (adrenaline) and norepinephrine directly into the bloodstream upon stimulation by preganglionic fibers.
- Physiological Effects: Prepares the body for stressful situations or emergencies: increased heart rate, increased blood pressure, bronchodilation, pupil dilation, shunting blood to skeletal muscles, inhibition of digestion.
2. The Parasympathetic Nervous System (PNS): "Rest and Digest"
- Origin (Cranio-sacral System): Preganglionic neurons originate from two distinct regions:
- Cranial Nerves (CN): Nuclei within the brainstem give rise to preganglionic fibers that travel with specific cranial nerves:
- CN III (Oculomotor): To the ciliary ganglion, innervating intrinsic eye muscles for pupillary constriction and lens accommodation.
- CN VII (Facial): To the pterygopalatine and submandibular ganglia, innervating lacrimal, submandibular, and sublingual glands for tear and saliva production.
- CN IX (Glossopharyngeal): To the otic ganglion, innervating the parotid gland for saliva production.
- CN X (Vagus): The most extensive parasympathetic nerve, carrying about 75% of all parasympathetic fibers. It distributes widely to the thoracic and abdominal viscera (heart, lungs, digestive tract up to the distal transverse colon) via numerous small ganglia within the walls of the target organs (intramural ganglia).
- Sacral Spinal Cord: Preganglionic neurons arise from the lateral horns of the sacral spinal cord (segments S2, S3, S4). These fibers form the pelvic splanchnic nerves (pelvic nerves). They distribute to the pelvic organs (distal colon, rectum, bladder, reproductive organs) and associated structures.
- Cranial Nerves (CN): Nuclei within the brainstem give rise to preganglionic fibers that travel with specific cranial nerves:
- Ganglia: Parasympathetic ganglia are typically located very close to, or within the walls of, the target organs (intramural or terminal ganglia). This results in very long preganglionic fibers and very short postganglionic fibers.
- Neurotransmitters:
- Preganglionic fibers: Release acetylcholine (ACh) at the ganglion (nicotinic receptors).
- Postganglionic fibers: Release acetylcholine (ACh) at the target organ (muscarinic receptors).
- Physiological Effects: Promotes body maintenance, energy conservation, and "housekeeping" activities: decreased heart rate, decreased blood pressure, pupillary constriction, increased digestive activity, emptying of bladder and rectum.
The Differences (SNS vs. PNS)
- Location of Preganglionic Neuron Cell Bodies (Origin):
- SNS: Thoraco-lumbar (T1-L2/L3 spinal cord).
- PNS: Cranio-sacral (Brainstem nuclei of CN III, VII, IX, X and S2-S4 spinal cord).
- Length of Fibers:
- SNS: Short preganglionic, long postganglionic.
- PNS: Long preganglionic, short postganglionic.
- Location of Ganglia:
- SNS: Ganglia are generally near the spinal cord (paravertebral chain or prevertebral ganglia).
- PNS: Ganglia are generally near or within the target organs (terminal/intramural ganglia).
- Neurotransmitter at the Ganglion (Synapse between Pre- and Post-ganglionic neurons):
- Both SS and PS preganglionic axons are in the PNS and release acetylcholine (ACh). This ACh acts on nicotinic receptors on the postganglionic neuron. This is a commonality and an important point to remember.
- Neurotransmitter at the Effector Organ (Synapse between Post-ganglionic neuron and Target):
- SNS: Postganglionic fibers primarily release norepinephrine (NE) (adrenergic transmission) at the target organ. (Exception: ACh to sweat glands).
- PNS: Postganglionic fibers release acetylcholine (ACh) (cholinergic transmission) at the target organ. This ACh acts on muscarinic receptors.
Anatomical Organization of the Nervous System
The nervous system is anatomically divided into two major components based on their physical location:
1. Central Nervous System (CNS)
- Composition: The CNS is composed of the brain and the spinal cord.
- Function: It is the main processing center of the body; it receives information from the PNS, integrates it, and sends out commands to the PNS. It is responsible for higher functions like thought, memory, emotion, and complex motor control.
- Protection: Both the brain and spinal cord are encased in bone (cranium and vertebral column, respectively) and protected by meninges and cerebrospinal fluid (CSF).
2. Peripheral Nervous System (PNS)
- Composition: The PNS consists of all the neural structures outside the brain and spinal cord. This includes:
- 31 pairs of spinal nerves: These emerge from the spinal cord at different levels and innervate the trunk and limbs.
- 12 pairs of cranial nerves: These emerge directly from the brain (mostly the brainstem) and primarily innervate structures of the head, neck, and some visceral organs (e.g., vagus nerve).
- Ganglia: Collections of neuron cell bodies located outside the CNS.
- Plexuses: Networks of nerves (e.g., brachial plexus, lumbar plexus).
- Function: It serves as the communication link between the CNS and the rest of the body. It carries sensory information from the periphery to the CNS (afferent pathways) and motor commands from the CNS to muscles and glands (efferent pathways).
Spinal Cord
The spinal cord is a vital component of the CNS. It is an elongated, cylindrical part of the CNS that extends from the foramen magnum (where it is continuous with the brainstem) down to roughly the level of the L1 or L2 vertebra in adults. It's much shorter than the vertebral column itself.
- Protection: It is protected by the vertebral column, meninges (dura mater, arachnoid mater, pia mater), and cerebrospinal fluid.
- Key Functions:
- Center for Reflex Actions: The spinal cord houses many neural circuits that mediate rapid, involuntary responses to stimuli, known as spinal reflexes. These reflexes do not require direct input from the brain for their basic execution (e.g., withdrawal reflex from a painful stimulus).
- Pathways for Ascending Nerve Tracts: It contains bundles of axons (white matter tracts) that transmit sensory information (touch, pain, temperature, proprioception) from the body up to the brain.
- Pathways for Descending Nerve Tracts: It also contains bundles of axons (white matter tracts) that transmit motor commands from the brain down to the muscles and glands of the body.
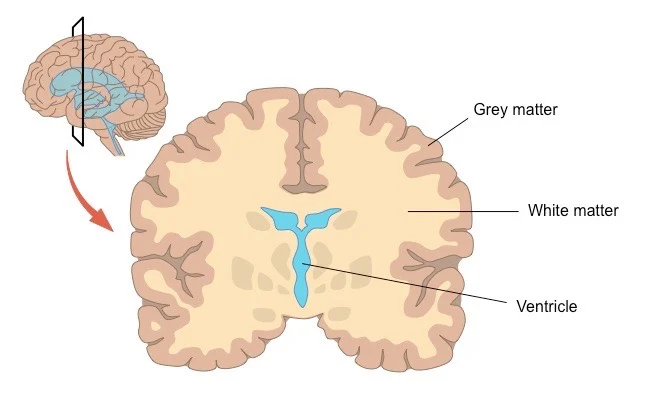
Forms and Quantity of Grey Matter
The spinal cord, like the brain, is composed of gray matter and white matter.
- Gray Matter:
- Composition: Primarily consists of neuron cell bodies, dendrites, unmyelinated axons, and glial cells.
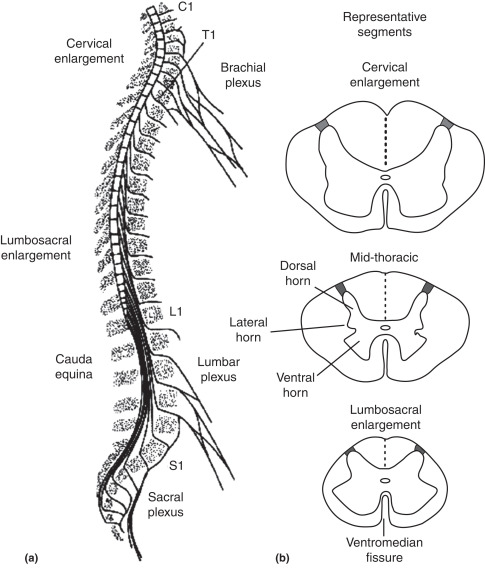
- Shape: In a cross-section of the spinal cord, the gray matter has a characteristic H- or butterfly-shape, with projections called horns.
- Horns:
- Anterior (Ventral) Horns: Contain motor neuron cell bodies that innervate skeletal muscles. These are generally larger in regions associated with limb innervation (cervical and lumbar enlargements).
- Posterior (Dorsal) Horns: Receive sensory input from the body via afferent fibers. They contain interneurons and projection neurons involved in processing sensory information.
- Lateral Horns: Present only in the thoracic and upper lumbar (T1-L2/L3) and sacral (S2-S4) segments. They contain preganglionic autonomic neuron cell bodies (sympathetic in thoraco-lumbar, parasympathetic in sacral).
- Quantity: The amount of gray matter varies along the length of the spinal cord. It is most abundant in the cervical and lumbar enlargements, which correspond to the areas that innervate the upper and lower limbs, respectively. This is because these regions require a greater density of motor neurons for complex limb movements and a greater amount of sensory processing.
Ascending Fiber Systems (Sensory Pathways)
| Name | Function | Origin | Ending | Location in Cord |
|---|---|---|---|---|
| Dorsal column system | Fine touch, proprioception, two-point discrimination | Skin, joints, tendons | Dorsal column nuclei. Second-order neurons project to contralateral thalamus (cross in medulla at lemniscal decussation) | Dorsal column |
| Spinothalamic tracts | Sharp pain, temperature, crude touch | Skin | Dorsal horn. Second-order neurons project to contralateral thalamus (cross in spinal cord close to level of entry) | Ventrolateral column |
| Dorsal spinocerebellar tract | Movement and position mechanisms | Muscle spindles, Golgi tendon organs, touch and pressure receptors (via nucleus dorsalis [i.e., Clarke's column]) | Cerebellar paleocortex (via ipsilateral inferior cerebellar peduncle) | Lateral column |
| Ventral spinocerebellar | Movement and position mechanisms | Muscle spindles, Golgi tendon organs, touch and pressure receptors | Cerebellar paleocortex (via contralateral and ipsilateral superior cerebellar peduncle) | Lateral column |
| Spinoreticular pathway | Deep and chronic pain | Deep somatic structures | Reticular formation of brain stem | Polysynaptic, diffuse pathway in ventrolateral column |
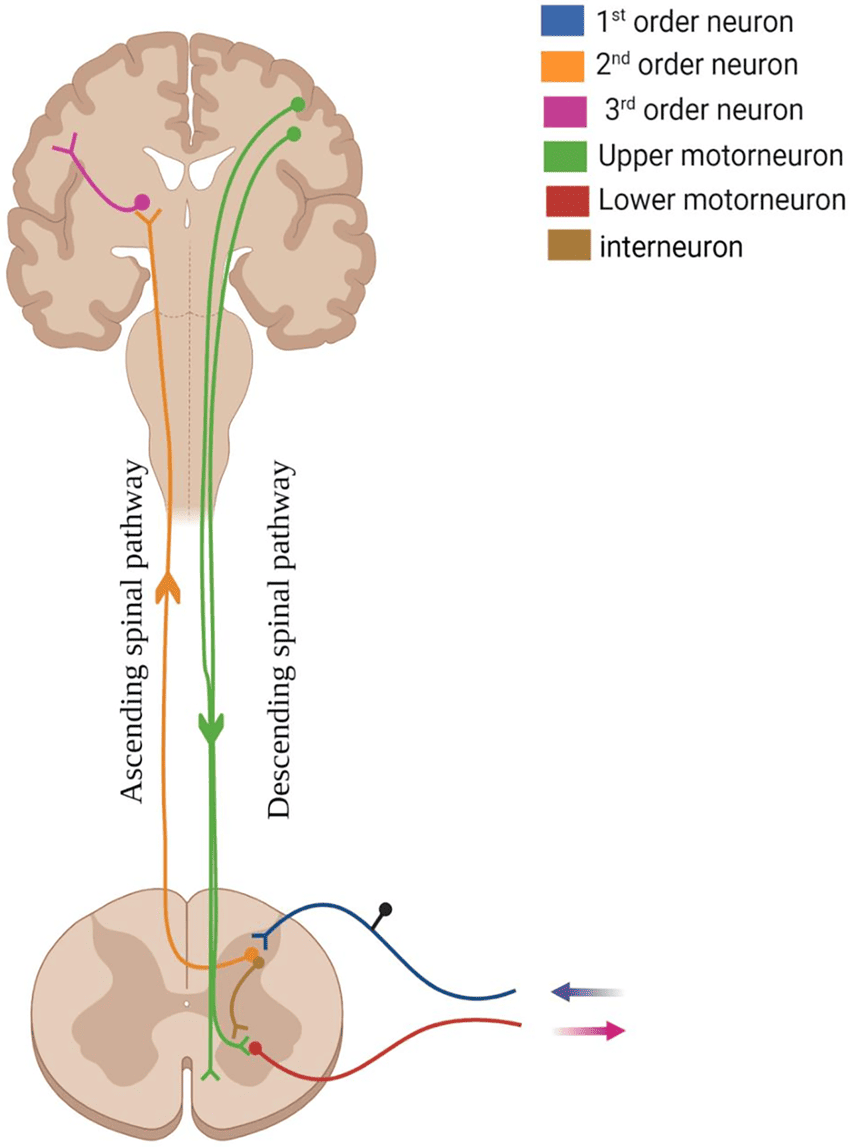
Descending Fiber Systems
| System | Function | Origin | Ending | Location in Cord |
|---|---|---|---|---|
| Lateral corticospinal (pyramidal) tract | Fine motor function (controls distal musculature), Modulation of sensory functions | Motor and premotor cortex | Anterior horn cells (interneurons and lower motor neurons) | Lateral column (crosses in medulla at pyramidal decussation) |
| Anterior corticospinal tract | Gross and postural motor function (proximal and axial musculature) | Motor and premotor cortex | Anterior horn neurons (interneurons and lower motor neurons) | Anterior column (uncrossed until after descending, when some fibers decussate) |
| Vestibulospinal tract | Postural reflexes | Lateral and medial vestibular nucleus | Anterior horn interneurons and motor neurons (for extensors) | Ventral column |
| Rubrospinal | Motor function | Red nucleus | Ventral horn interneurons | Lateral column |
| Reticulospinal | Modulation of sensory transmission (especially pain), Modulation of spinal reflexes | Brain stem reticular formation | Dorsal and ventral horn | Anterior column |
| Descending autonomic | Modulation of autonomic functions | Hypothalamus, brain stem nuclei | Preganglionic autonomic neurons | Lateral columns |
| Tectospinal | Reflex head turning | Midbrain | Ventral horn interneurons | Ventral column |
| Medial longitudinal fasciculus | Coordination of head and eye movements | Vestibular nuclei | Cervical gray | Ventral column |
The Brain
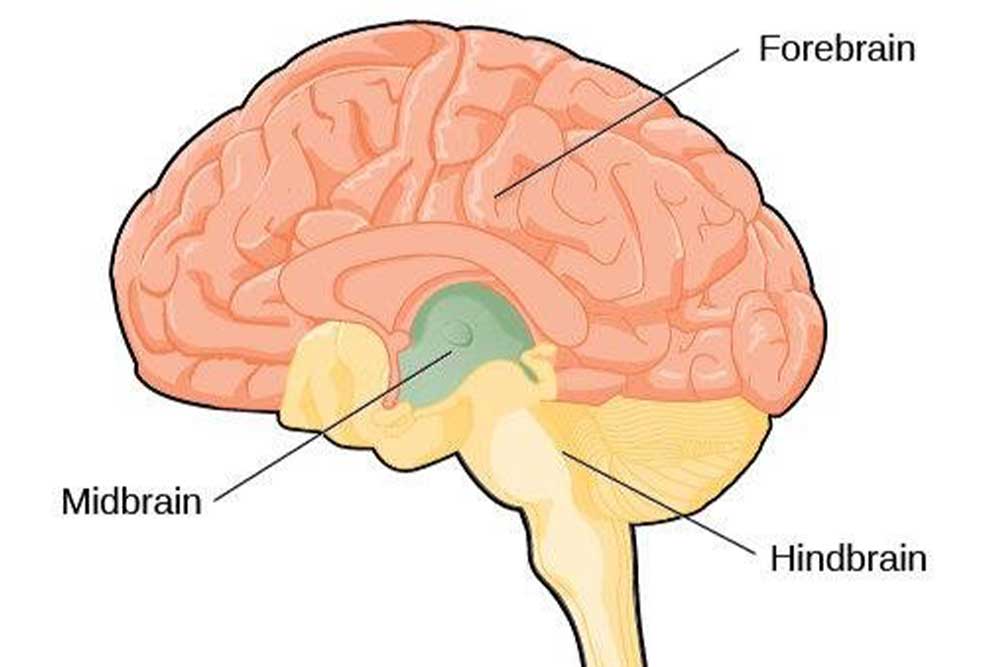
Divisions of the Brain
The primary divisions of the brain are crucial for understanding its organization and function.
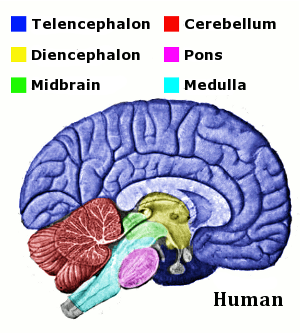
- Forebrain (Prosencephalon):
- This is the largest and most complex part of the brain.
- It is further subdivided into:
- Telencephalon:
- Cerebrum: This includes the cerebral cortex (the highly folded outer layer), the white matter underlying it, and the basal ganglia (deep nuclei involved in motor control).
- Key Functions: Responsible for higher-level functions like thought, language, memory, consciousness, voluntary movement, sensory perception, and executive functions.
- Diencephalon:
- Thalamus: The major sensory relay station for most sensory information (except olfaction) en route to the cerebral cortex. It also plays a role in motor control, emotion, and arousal.
- Hypothalamus: Crucial for homeostasis, regulating vital functions such as body temperature, hunger, thirst, sleep-wake cycles, and endocrine system control (via the pituitary gland). It also influences emotions and behavior.
- Epithalamus: Includes the pineal gland (produces melatonin, involved in sleep-wake cycles) and the habenular nuclei (involved in limbic system functions).
- Subthalamus: Involved in motor control, closely linked with the basal ganglia.
- Telencephalon:
- Midbrain (Mesencephalon):
- This is the smallest part of the brainstem.
- It connects the forebrain to the hindbrain.
- Key Structures:
- Tectum: Contains the superior colliculi (visual reflexes, eye movements) and inferior colliculi (auditory reflexes, sound localization).
- Tegmentum: Contains nuclei involved in motor control (e.g., red nucleus, substantia nigra – crucial for dopamine production and implicated in Parkinson's disease), and parts of the reticular formation.
- Cerebral Peduncles: Contain descending motor tracts from the cerebrum to the brainstem and spinal cord.
- Key Functions: Involved in visual and auditory reflexes, motor control, sleep/wake, arousal, and temperature regulation.
- Hindbrain (Rhombencephalon): cerebellum, pons, and medulla oblongata.
Hindbrain Components:
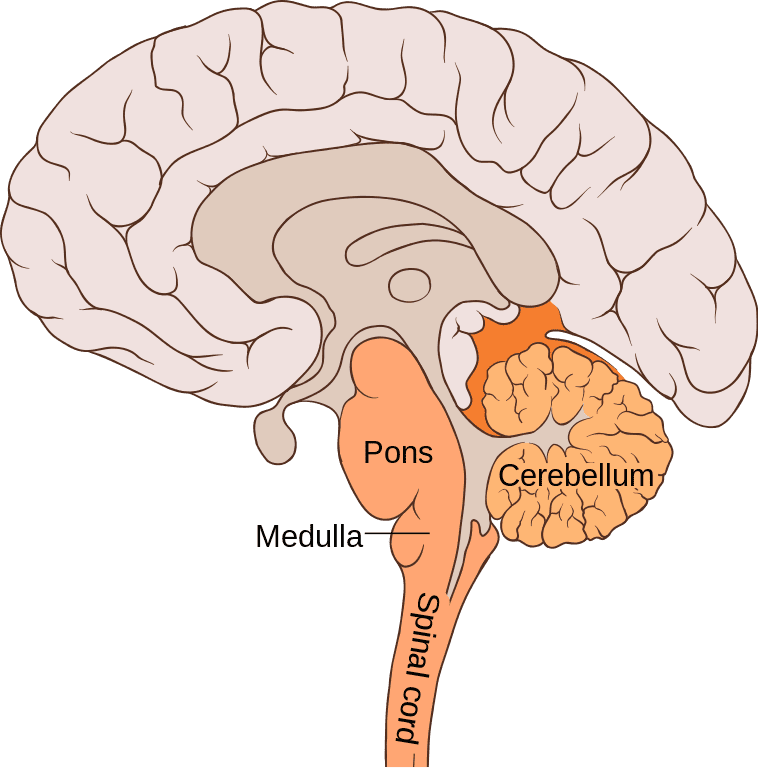
A. Cerebellum:
- Location: Occupies the posterior cranial fossa, situated inferior to the occipital and temporal lobes of the cerebrum, and posterior to the pons and medulla oblongata.
- Structure:
- Two hemispheres joined by the vermis (a central constricted region).
- Surface is characterized by numerous folds called folia (similar to gyri on the cerebrum, but smaller and more tightly packed), separated by fissures.
- Connects to the brainstem via three pairs of cerebellar peduncles (superior, middle, inferior), which contain both afferent (input) and efferent (output) fibers.
- Functions (as you stated, but with emphasis):
- Motor Coordination: This is its primary role. It compares intended movements with actual movements and makes adjustments to ensure smooth, precise, and coordinated voluntary movements. It helps refine movements by influencing timing, force, and extent.
- Balance and Posture: Receives proprioceptive information from muscles and joints and vestibular information from the inner ear to maintain equilibrium.
- Motor Learning: Involved in adapting and refining motor skills through practice.
- Muscle Tone: Helps regulate muscle tone.
Disorders (Cerebellar Ataxia):
- Hypotonia: Decreased muscle tone.
- Pendulous knee jerk: Exaggerated and prolonged swing of the leg after patellar reflex.
- Intention tremors: Tremors that become more pronounced as the individual attempts to perform a voluntary movement.
- Alteration of gait (ataxic gait): Wide-based, unsteady, staggering walk, often described as "drunk-like."
- Dysmetria: Inability to accurately judge the distance or range of a movement (e.g., overshooting or undershooting a target).
- Dysdiadochokinesia: Impaired ability to perform rapid alternating movements (e.g., pronation/supination of the forearm).
- Nystagmus: Involuntary, rhythmic eye movements.
- Scanning speech: Slow, monotonous speech with each syllable spoken separately.
Causes: trauma, tumors, toxins (heavy metals, alcohol), hereditary conditions, infections, developmental abnormalities (hypoplasia, agenesis).
B. Pons:
- Location: Sits superior to the medulla oblongata and anterior to the cerebellum. It forms a prominent bulge on the ventral surface of the brainstem.
- Structure: Contains many transverse fibers that connect the two cerebellar hemispheres, and longitudinal fibers that run between the cerebrum and spinal cord.
- Key Nuclei and Tracts:
- Pontine nuclei: Relay information from the cerebral cortex to the cerebellum, crucial for motor learning and coordination.
- Cranial Nerve Nuclei: Contains nuclei for several cranial nerves (V, VI, VII, VIII).
- Respiratory Centers: Contains the pneumotaxic and apneustic centers, which work with the medulla to regulate the rate and depth of breathing.
- Ascending and Descending Tracts: All major tracts (sensory and motor) pass through the pons.
- Functions:
- Relay Station: Connects the cerebrum to the cerebellum via the middle cerebellar peduncles.
- Respiration Control: Modifies respiratory rhythm.
- Sleep and Arousal: Involved in regulating sleep stages and consciousness.
- Facial Sensation and Movement: Houses nuclei for sensory input from the face and motor control of facial expressions, eye movements, and chewing.
C. Medulla Oblongata:
- Location: The most inferior part of the brainstem, continuous with the spinal cord at the foramen magnum.
- Structure:
- Pyramids: Two large, anterior bulges formed by the corticospinal tracts (major motor pathways). The decussation of the pyramids (crossing over of these tracts) occurs here, explaining why each side of the brain controls the opposite side of the body.
- Olives: Lateral to the pyramids, contain the inferior olivary nuclei, which play a role in motor control and learning (relay to cerebellum).
- Reticular Formation: Extensive network of nuclei and fibers, extending throughout the brainstem, involved in arousal, sleep, muscle tone, and pain modulation.
- Key Nuclei and Tracts:
- Vital Reflex Centers: Contains critical autonomic centers:
- Cardiovascular Center: Regulates heart rate and force of contraction.
- Vasomotor Center: Controls blood vessel diameter (and thus blood pressure).
- Respiratory Rhythmicity Center: Sets the basic rhythm of breathing (in conjunction with the pons).
- Other Reflex Centers: Vomiting, swallowing, coughing, sneezing, hiccupping.
- Cranial Nerve Nuclei: Contains nuclei for cranial nerves (IX, X, XI, XII).
- Nucleus Gracilis and Cuneatus: Relay sensory information for fine touch, proprioception, and vibration to the thalamus (via the medial lemniscus).
- Vital Reflex Centers: Contains critical autonomic centers:
- Functions:
- Life-Sustaining Functions: Controls many essential involuntary activities. Damage to the medulla is often fatal.
- Sensory and Motor Relay: All ascending and descending tracts pass through the medulla, connecting the spinal cord to higher brain centers.
Overall Functions of the Brainstem:
- Conduit for Tracts: All major ascending (sensory) and descending (motor) pathways pass through the brainstem, acting as a crucial communication link.
- Cranial Nerve Nuclei: Houses the nuclei for most of the cranial nerves (III through XII), which control sensory and motor functions of the head, face, and neck, and some visceral organs.
- Integrative Functions: Contains vital centers for:
- Respiration
- Cardiovascular control
- Consciousness and Arousal (via the Reticular Activating System - RAS)
- Sleep-wake cycles
- Pain modulation
- Control of posture and balance
Forebrain (Prosencephalon)
The forebrain is the most anterior and largest part of the brain, responsible for higher-order functions. It develops from the prosencephalon in the embryonic brain. It can be broadly divided into:
- Telencephalon: This includes the cerebral cortex, white matter, and basal ganglia.
- Diencephalon: This includes the thalamus, hypothalamus, epithalamus, and subthalamus.
1. Cerebral Hemispheres and Cerebral Cortex
- Structure: The cerebrum consists of two large cerebral hemispheres (right and left) that are largely mirror images of each other but specialize in different functions (hemispheric lateralization).
- They are separated by the longitudinal fissure and connected by a large commissure called the corpus callosum.
- The outer layer is the cerebral cortex, which is highly convoluted (folded) into gyri (ridges) and sulci (grooves), which vastly increases its surface area.
- Beneath the cortex lies the cerebral white matter, which contains myelinated axons connecting different parts of the brain.
- Corpus Callosum: A massive bundle of white matter (around 200-250 million axonal projections) that ensures communication and coordination between the two cerebral hemispheres. Without it, the hemispheres would operate largely independently.
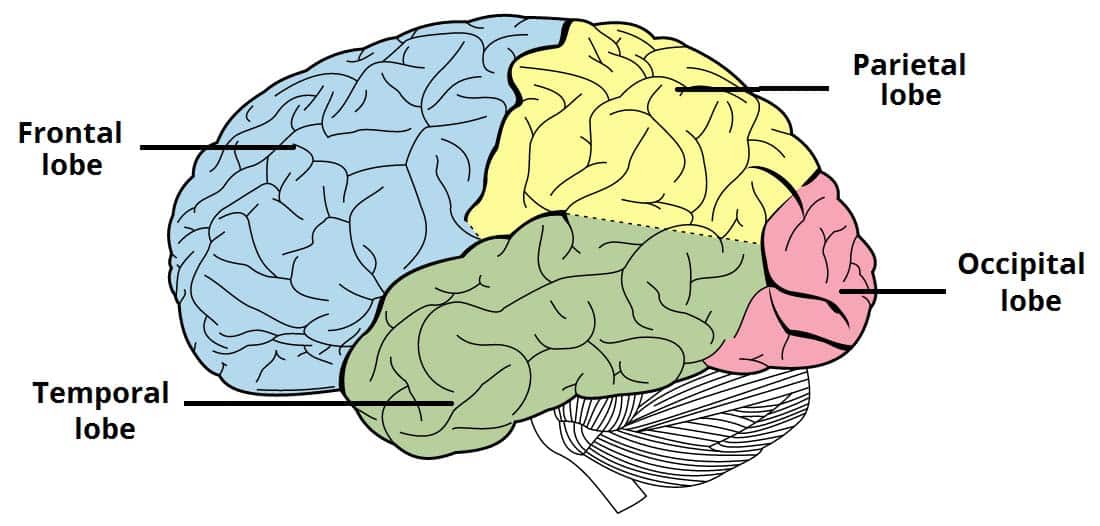
- Cerebral Cortex - Lobes: Each hemisphere is further divided into four major lobes, generally named after the overlying skull bones:
1. Frontal Lobe:
- Location: Anterior to the central sulcus.
- Key Areas:
- Primary Motor Cortex (Precentral Gyrus): Initiates voluntary movements.
- Premotor Cortex and Supplementary Motor Area: Plan and coordinate complex movements.
- Prefrontal Cortex: Higher-order cognitive functions – planning, decision-making, social behavior, personality, working memory, impulse control. Often considered the "executive center."
- Broca's Area: (Usually in the left hemisphere) Involved in speech production.
- Functions: Voluntary movement, executive functions, reasoning, problem-solving, personality, language production.
2. Parietal Lobe:
- Location: Posterior to the central sulcus, superior to the temporal lobe.
- Key Areas:
- Primary Somatosensory Cortex (Postcentral Gyrus): Receives and processes tactile (touch), proprioceptive (body position), temperature, and pain information from the body.
- Somatosensory Association Area: Interprets and integrates sensory information.
- Functions: Processing sensory information, spatial awareness, navigation, integration of sensory and motor information.
3. Temporal Lobe:
- Location: Inferior to the lateral sulcus.
- Key Areas:
- Primary Auditory Cortex: Processes sound.
- Wernicke's Area: (Usually in the left hemisphere) Crucial for language comprehension.
- Hippocampus: Deep within, vital for memory formation (especially new long-term memories).
- Amygdala: Deep within, involved in processing emotions (especially fear) and emotional memories.
- Functions: Auditory processing, memory, emotion, language comprehension.
4. Occipital Lobe:
- Location: Most posterior lobe.
- Key Areas:
- Primary Visual Cortex: Processes visual information (color, form, motion).
- Visual Association Areas: Interpret and recognize visual stimuli.
- Functions: Visual processing.
Insula (or Insular Cortex): Often considered a fifth lobe, tucked away deep within the lateral sulcus. Involved in taste, visceral sensation, pain processing, and interoception (awareness of internal body states).
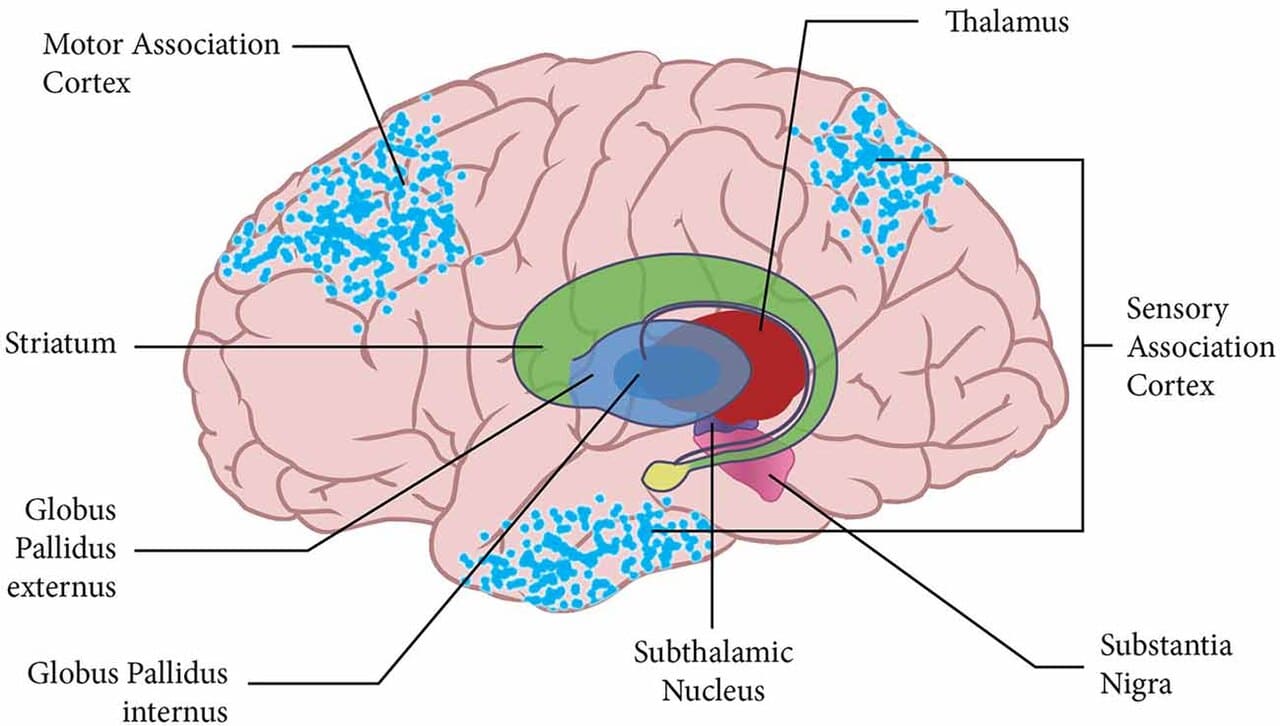
2. Basal Ganglia (or Basal Nuclei)
- Location: A group of subcortical nuclei located deep within the cerebral white matter of the forebrain, adjacent to the diencephalon.
- Key Components:
- Caudate nucleus
- Putamen (together, the caudate and putamen are called the striatum)
- Globus pallidus
- (Functionally associated nuclei often included are the subthalamic nucleus and substantia nigra from the midbrain)
- Functions:
- Motor Control: Primarily involved in the initiation and modulation of voluntary movement. They help select appropriate movements, suppress unwanted movements, and regulate muscle tone. They do not directly initiate movement (that's the motor cortex) but rather influence it.
- Cognition and Emotion: Also play roles in procedural learning, habit formation, motivation, and some aspects of cognition and emotion.
- Disorders: Damage to the basal ganglia can lead to various movement disorders:
- Parkinson's Disease: Characterized by tremors, rigidity, bradykinesia (slow movement), and postural instability, due to degeneration of dopamine-producing neurons in the substantia nigra.
- Huntington's Disease: Characterized by involuntary, jerky movements (chorea), cognitive decline, and psychiatric problems, due to degeneration in the striatum.
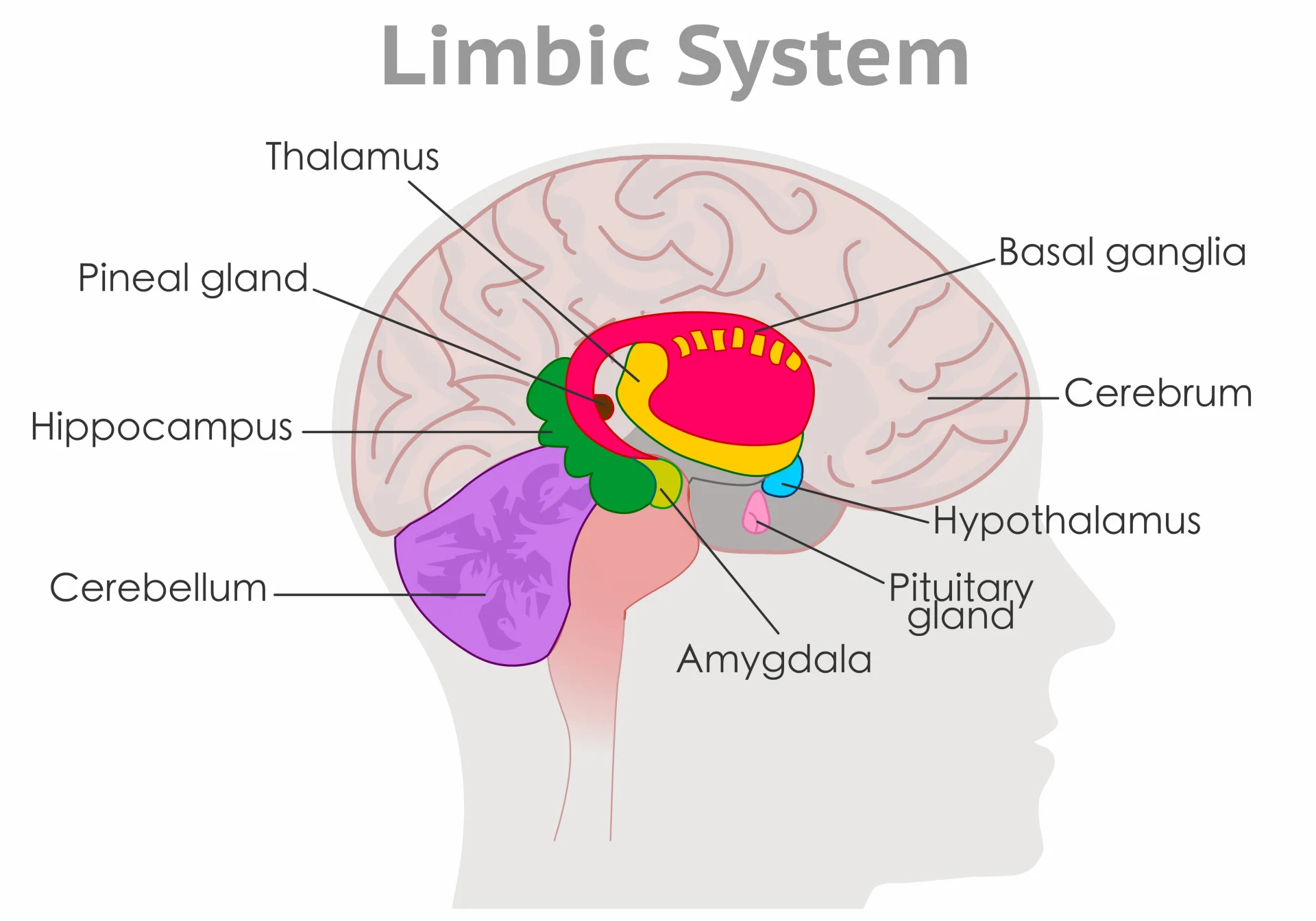
3. Limbic System
- Nature: This is a functional system, not a distinct anatomical structure located in one specific place. It is a collection of interconnected brain structures located around the medial edge of the cerebrum and diencephalon.
- Key Structures (simplified):
- Hippocampus: Memory formation (converting short-term to long-term memory).
- Amygdala: Processing emotions (especially fear, anger), emotional memory.
- Hypothalamus: (part of diencephalon) Autonomic and endocrine responses to emotional states.
- Cingulate Gyrus: Involved in emotion formation and processing, learning, and memory.
- Thalamus: (part of diencephalon) Relays sensory information to the limbic system.
- Olfactory Bulb: Sense of smell, which has strong connections to memory and emotion.
- Functions:
- Emotion: Crucial for emotional experience and expression.
- Memory: Plays a vital role in learning and memory formation.
- Motivation and Reward: Involved in the brain's reward system.
- Olfaction: Strong links between smell and limbic system.
4. Diencephalon
- Location: Centrally located, deep within the brain, superior to the brainstem, and surrounded by the cerebral hemispheres. It acts as a primary relay and processing center for sensory information and autonomic control.
- Key Components:
- Thalamus: Two egg-shaped masses of gray matter, one in each hemisphere.
- Function: The major relay station for nearly all sensory information (except olfaction) ascending to the cerebral cortex. It acts as a "gateway" to the cortex, filtering and processing information. Also involved in motor control, arousal, and consciousness.
- Hypothalamus: Small but incredibly vital structure located inferior to the thalamus. Connected to the pituitary gland.
- Function: The primary control center for homeostasis. Regulates body temperature, hunger, thirst, sleep-wake cycles (circadian rhythm), sexual drive, and controls the endocrine system by influencing the pituitary gland. It also influences emotional responses.
- Epithalamus: Smallest part of the diencephalon, posterior to the thalamus.
- Function: Contains the pineal gland, which secretes melatonin (involved in sleep-wake cycles and circadian rhythms). Also contains the habenular nuclei (involved in limbic system functions and olfaction).
- Subthalamus:
- Description: Located inferior to the thalamus and lateral to the hypothalamus.
- Function: Functionally associated with the basal ganglia and involved in motor control. Damage can lead to hemiballismus (violent, flinging movements of one side of the body).
- Thalamus: Two egg-shaped masses of gray matter, one in each hemisphere.