Muscles of the Axial Skeleton
A. Muscles of the Head and Face
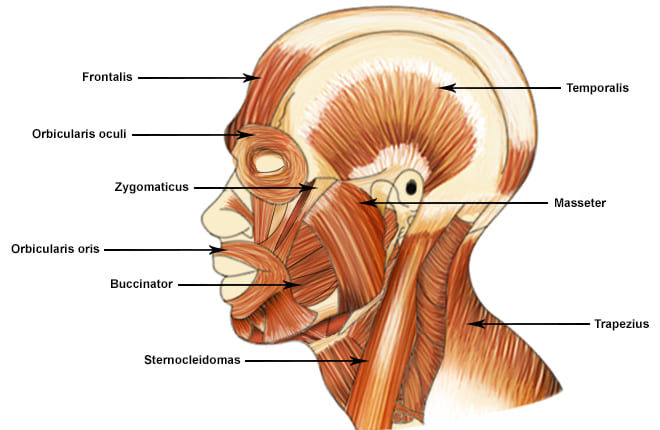
The muscles of the head can be broadly categorized into muscles of facial expression and muscles of mastication (chewing).
1. Muscles of Facial Expression
These unique muscles insert into the skin or other muscles, allowing us to show a wide range of emotions. They are all innervated by the Facial Nerve (Cranial Nerve VII).
a. Occipitofrontalis (Epicranius)
A broad muscle covering the top of the skull with two bellies. The Frontal belly raises the eyebrows and wrinkles the forehead, while the Occipital belly pulls the scalp posteriorly.
b. Orbicularis Oculi
A ring-like muscle encircling the eye. Its primary action is to close the eye (blinking, winking) and squint.
c. Orbicularis Oris
A complex muscle encircling the mouth. It closes and protrudes the lips, as in puckering or kissing.
d. Zygomaticus Major and Minor
Extend from the cheekbone to the corner of the mouth. They are the primary "smiling" muscles, raising the lateral corners of the mouth upward.
e. Buccinator
A thin, flat muscle of the cheek. It compresses the cheek for whistling or sucking and holds food between the teeth during chewing.
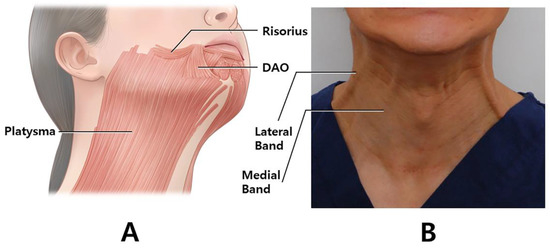
f. Platysma
A broad, superficial sheet of muscle in the neck. It tenses the skin of the neck, depresses the mandible, and pulls the lower lip down.
2. Muscles of Mastication (Chewing)
These four pairs of muscles are responsible for moving the mandible for chewing. They are all innervated by the Mandibular division of the Trigeminal Nerve (Cranial Nerve V3).
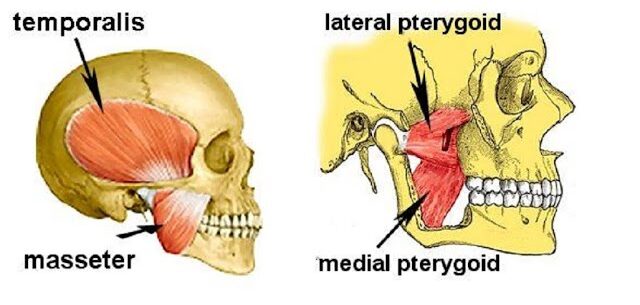
a. Masseter
A powerful muscle on the side of the jaw. It is the primary elevator of the mandible (closes the jaw).
b. Temporalis
A fan-shaped muscle in the temporal fossa. It elevates and retracts the mandible.
c. Medial Pterygoid
Located deep to the mandible. It elevates the jaw and assists in side-to-side grinding movements.
d. Lateral Pterygoid
Located deep in the jaw. It protracts the mandible (pulls it forward), moves it side-to-side, and is the only muscle of mastication that helps open the jaw.
Summary Table of Head & Face Muscles
| Muscle | Origin | Insertion | Action |
|---|---|---|---|
| FACIAL EXPRESSION (CN VII) | |||
| Occipitofrontalis | Galea aponeurotica (Frontal); Occipital bone (Occipital) | Skin of eyebrows; Galea aponeurotica | Raises eyebrows, wrinkles forehead, pulls scalp |
| Orbicularis Oculi | Frontal and maxillary bones | Tissue of eyelid | Closes eye, squints, blinks |
| Orbicularis Oris | Maxilla and mandible | Skin and muscle at angles of mouth | Closes and protrudes lips (puckering) |
| Zygomaticus Major/Minor | Zygomatic bone | Skin and muscle at angle of mouth | Raises lateral corners of mouth (smiling) |
| Buccinator | Molar region of maxilla and mandible | Orbicularis oris | Compresses cheek (whistling, sucking) |
| Platysma | Fascia of chest | Base of mandible; skin at corner of mouth | Tenses skin of neck, depresses mandible |
| MASTICATION (CN V3) | |||
| Masseter | Zygomatic arch | Angle and ramus of mandible | Elevates mandible (closes jaw) |
| Temporalis | Temporal fossa | Coronoid process of mandible | Elevates and retracts mandible |
| Medial Pterygoid | Sphenoid and palatine bones | Medial surface of ramus of mandible | Elevates mandible, moves side-to-side |
| Lateral Pterygoid | Sphenoid bone | Condylar process of mandible; TMJ capsule | Protracts and depresses (opens) jaw |
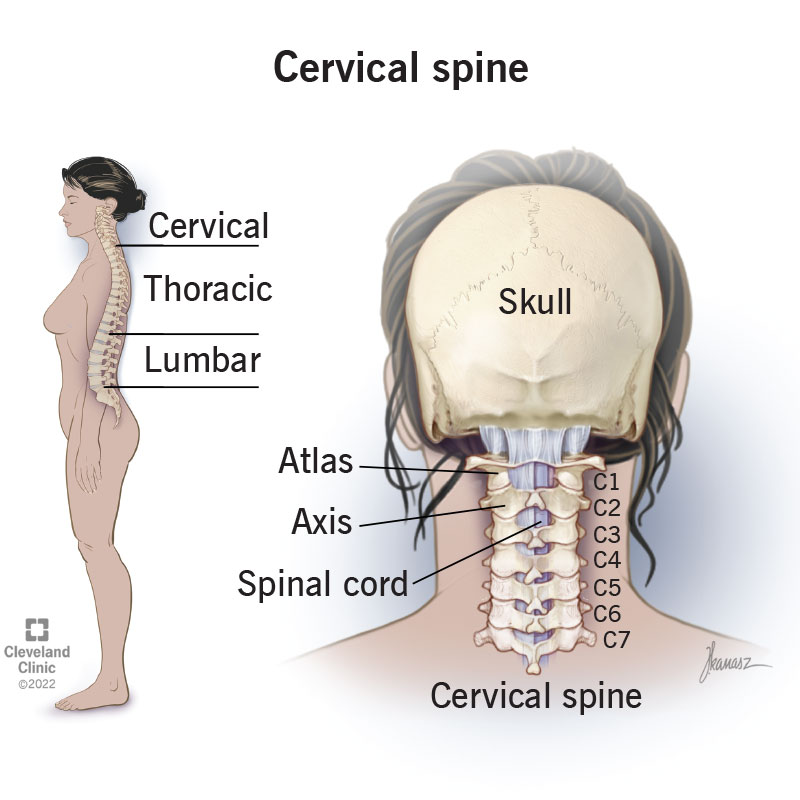
B. Muscles of the Neck
The muscles of the neck are diverse, responsible for moving the head, stabilizing the cervical spine, assisting in breathing, and facilitating swallowing and speech. They are categorized here based on location and primary actions.
1. Superficial Anterior Neck Muscles
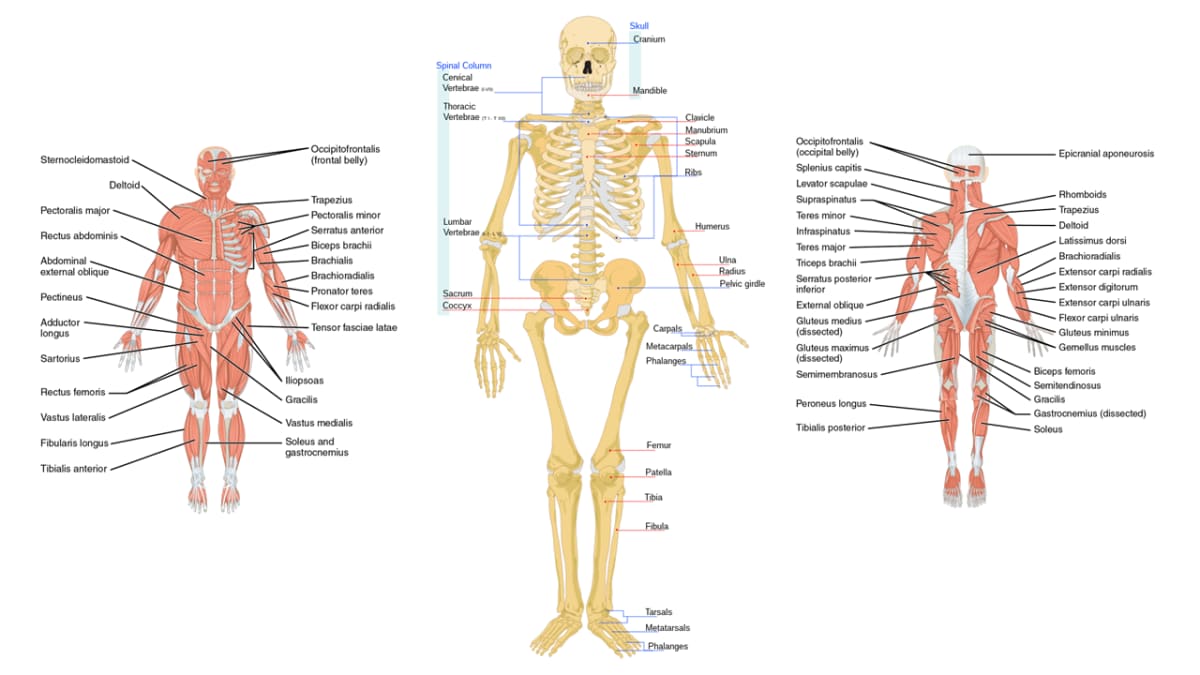
a. Sternocleidomastoid (SCM)
A large, two-headed muscle on each side of the neck. When acting alone (unilaterally), it rotates the head to the opposite side and flexes it to the same side. When both act together (bilaterally), they flex the neck (chin to chest).
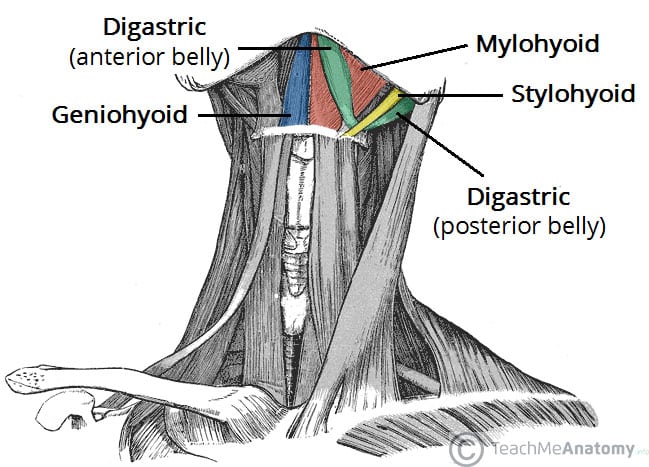
2. Suprahyoid Muscles (Above the Hyoid Bone)
These muscles form the floor of the mouth and are primarily responsible for elevating the hyoid bone during swallowing and speaking.
a. Digastric
Two-bellied muscle that elevates the hyoid or depresses the mandible (opens the mouth).
b. Mylohyoid
Forms the floor of the mouth; elevates hyoid and floor of mouth.
c. Geniohyoid
Elevates and protracts the hyoid bone.
d. Stylohyoid
Elevates and retracts the hyoid bone.
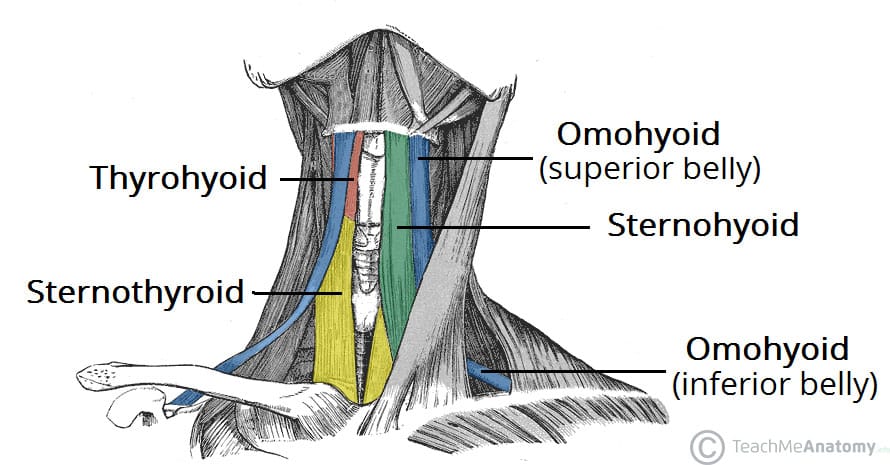
3. Infrahyoid Muscles (Strap Muscles - Below the Hyoid)
These "strap-like" muscles primarily depress the hyoid bone and larynx during swallowing and speaking.
a. Sternohyoid
Depresses the hyoid bone and larynx.
b. Omohyoid
Two-bellied muscle that depresses and retracts the hyoid.
c. Sternothyroid
Depresses the larynx and hyoid bone.
d. Thyrohyoid
Depresses the hyoid bone but elevates the larynx.
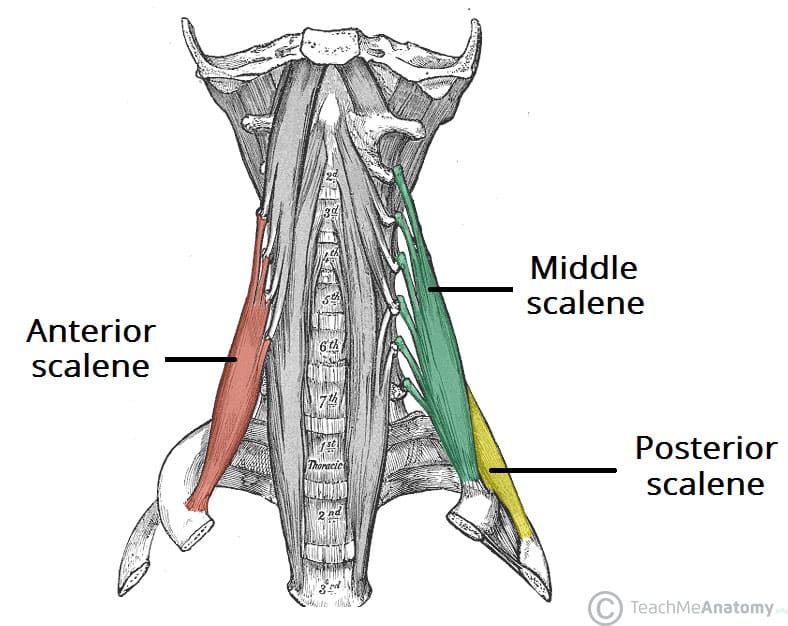
4. Deep Lateral Neck Muscles (Scalenes)
The Anterior, Middle, and Posterior Scalene muscles are important for lateral flexion of the neck. They also act as accessory muscles of inspiration by elevating the first two ribs.
Summary Table of Neck Muscles
| Muscle | Origin | Insertion | Innervation | Action |
|---|---|---|---|---|
| Sternocleidomastoid | Manubrium & Clavicle | Mastoid process | CN XI, C2-C3 | Unilateral: Rotates head opp., flexes same side. Bilateral: Flexes neck. |
| Digastric | Mandible & Mastoid process | Hyoid bone | CN V3 & CN VII | Elevates hyoid, depresses mandible. |
| Mylohyoid | Mandible | Hyoid bone | CN V3 | Elevates hyoid & floor of mouth. |
| Sternohyoid | Manubrium & Clavicle | Hyoid bone | Ansa cervicalis | Depresses hyoid and larynx. |
| Omohyoid | Scapula | Hyoid bone | Ansa cervicalis | Depresses and retracts hyoid. |
| Sternothyroid | Manubrium | Thyroid cartilage | Ansa cervicalis | Depresses larynx and hyoid. |
| Thyrohyoid | Thyroid cartilage | Hyoid bone | C1 via CN XII | Depresses hyoid, elevates larynx. |
| Scalenes (Ant, Mid, Post) | Cervical vertebrae (C2-C7) | First & Second ribs | Cervical spinal nerves | Flexes neck, elevates ribs for inspiration. |
C. Muscles of the Torso (Trunk)
The muscles of the trunk are vital for maintaining posture, protecting internal organs, facilitating respiration, and enabling a wide range of movements.
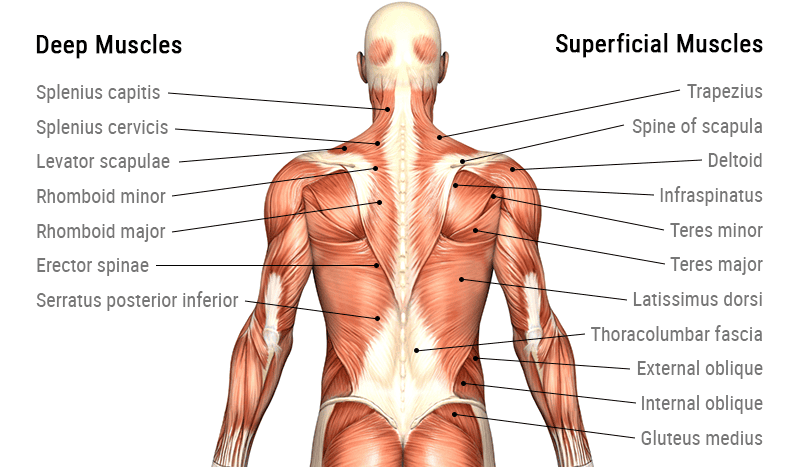
1. Muscles of the Back
These complex, layered muscles move and stabilize the vertebral column, head, and shoulders.
a. Superficial Back Muscles
Primarily act on the upper limbs. Includes the large Trapezius (moves scapula), Latissimus Dorsi (extends and adducts arm), and the deeper Rhomboids and Levator Scapulae (retract and elevate scapula).
b. Intermediate Back Muscles
Respiratory muscles. The Serratus Posterior Superior elevates ribs for inspiration, while the Serratus Posterior Inferior depresses ribs for expiration.
c. Deep (Intrinsic) Back Muscles
Responsible for posture and vertebral column movement. The main group is the massive Erector Spinae (Iliocostalis, Longissimus, Spinalis), the prime mover of back extension. Deeper still is the Transversospinalis group, which stabilizes vertebrae.
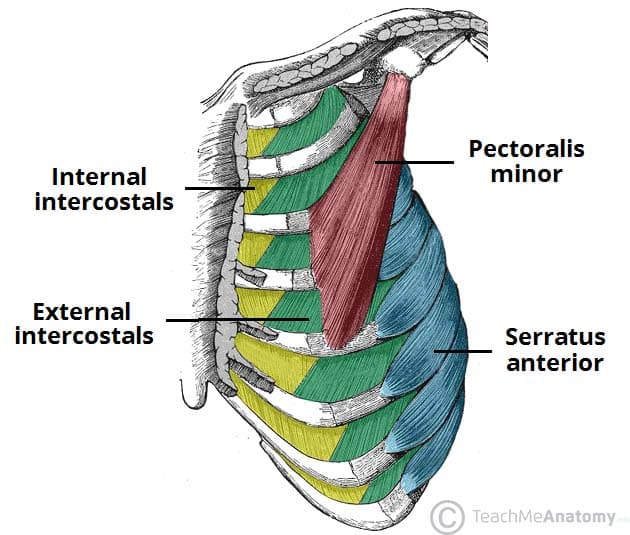
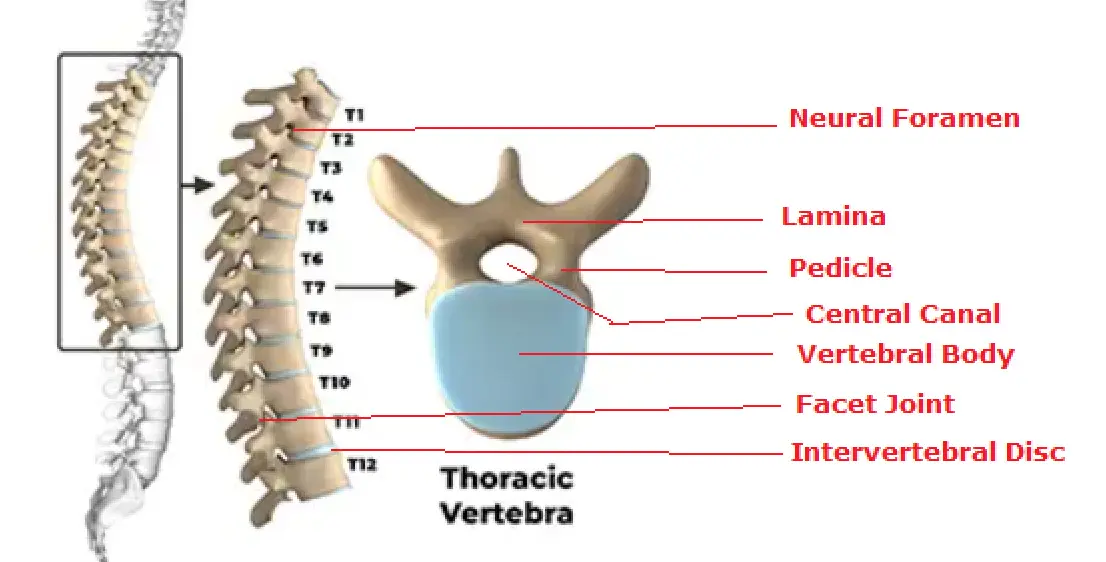
2. Muscles of the Thorax (Chest Wall)
These muscles are primarily involved in the mechanics of breathing.
a. Intercostal Muscles
The External Intercostals elevate the ribs for inspiration. The Internal and Innermost Intercostals depress the ribs for forced expiration.
b. Diaphragm
The primary muscle of respiration. This large, dome-shaped muscle separates the thoracic and abdominal cavities. It contracts and flattens to increase thoracic volume, causing inspiration.
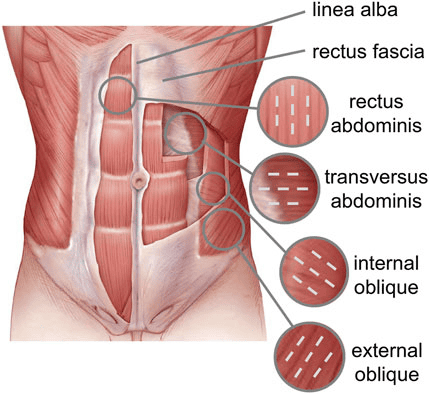
3. Muscles of the Abdominal Wall
Form a strong, flexible wall that protects viscera, moves the trunk, and compresses the abdominal cavity.
a. Rectus Abdominis
The vertical "six-pack" muscle, segmented by tendinous intersections. It is the primary flexor of the vertebral column (as in sit-ups).
b. Obliques & Transversus Abdominis
Three layers of flat muscles that wrap the abdomen. The External Oblique (fibers run down and in), Internal Oblique (fibers run up and in), and the deepest Transversus Abdominis (fibers run horizontally). They work together to rotate and flex the trunk and compress the abdominal contents.
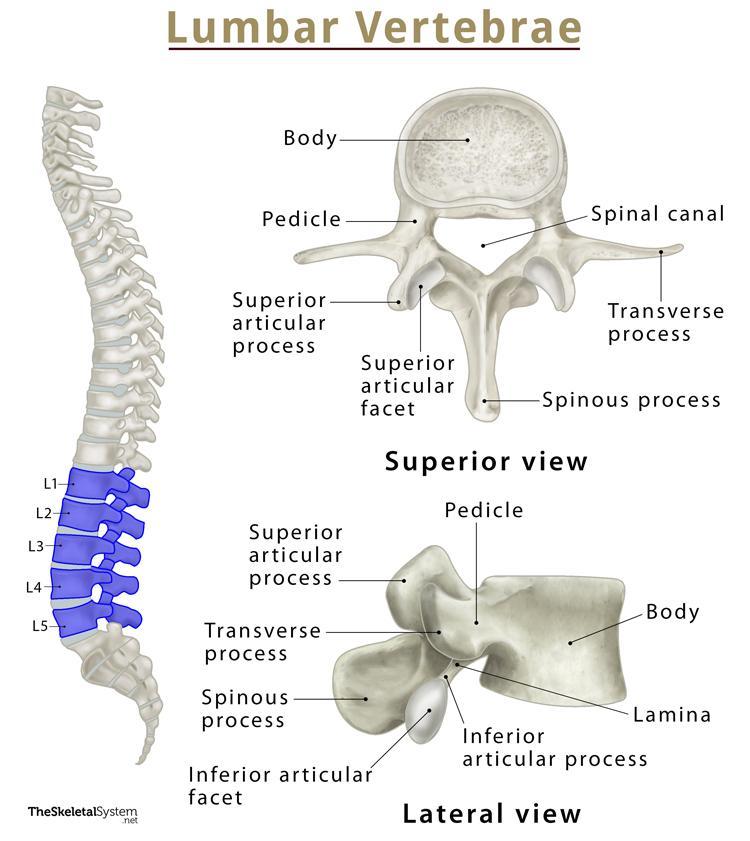
c. Quadratus Lumborum
A deep, square-shaped muscle of the posterior abdominal wall that laterally flexes the trunk.
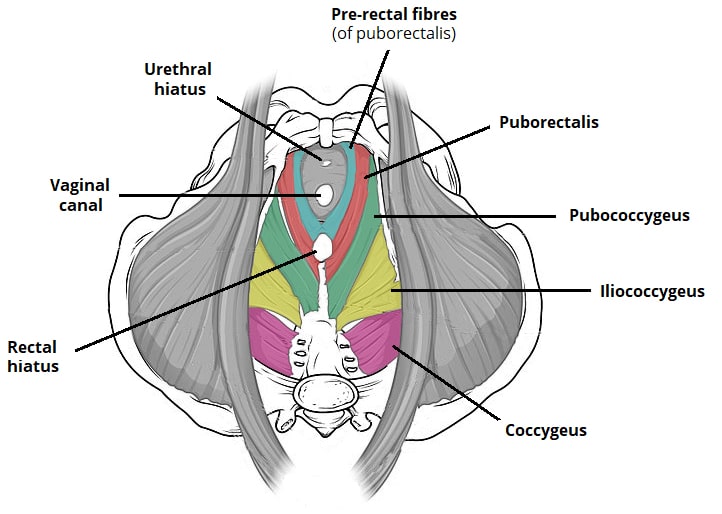
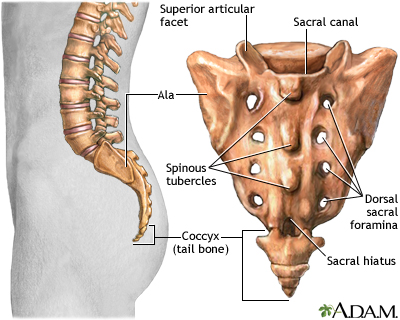
4. Pelvic Floor Muscles (Pelvic Diaphragm)
Close the inferior outlet of the pelvis, supporting pelvic organs and controlling continence.
a. Levator Ani Group & Coccygeus
This broad, funnel-shaped muscle group forms the major part of the pelvic floor, supporting pelvic organs and resisting increases in intra-abdominal pressure.
Summary Table of Torso Muscles
| Muscle | Origin | Insertion | Innervation | Main Actions |
|---|---|---|---|---|
| TRAPEZIUS | Occipital bone, C7-T12 spinous processes | Clavicle, acromion, spine of scapula | Spinal Accessory (CN XI), C3-C4 | Elevates, retracts, depresses, rotates scapula |
| LATISSIMUS DORSI | T7-L5 spinous processes, iliac crest | Intertubercular groove of humerus | Thoracodorsal Nerve (C6-C8) | Extends, adducts, medially rotates arm |
| ERECTOR SPINAE GROUP | Iliac crest, sacrum, vertebrae | Ribs, vertebrae, mastoid process | Dorsal rami of spinal nerves | Extend & laterally flex vertebral column |
| EXTERNAL INTERCOSTALS | Rib above | Rib below | Intercostal nerves (T1-T11) | Elevate ribs (inspiration) |
| INTERNAL INTERCOSTALS | Rib above | Rib below | Intercostal nerves (T1-T11) | Depress ribs (forced expiration) |
| DIAPHRAGM | Xiphoid, costal cartilages, lumbar vertebrae | Central tendon | Phrenic Nerves (C3-C5) | Primary muscle of inspiration |
| RECTUS ABDOMINIS | Pubic crest and symphysis | Xiphoid process, costal cartilages 5-7 | Intercostal nerves (T7-T12) | Flexes vertebral column, compresses abdomen |
| EXTERNAL OBLIQUE | Ribs 5-12 | Linea alba, pubic tubercle, iliac crest | Intercostal nerves (T7-T12) | Flexes & rotates trunk (opposite side) |
| INTERNAL OBLIQUE | Thoracolumbar fascia, iliac crest | Linea alba, pubic crest, ribs 10-12 | Intercostal (T7-T12), Iliohypo/inguinal (L1) | Flexes & rotates trunk (same side) |
| TRANSVERSUS ABDOMINIS | Thoracolumbar fascia, iliac crest, ribs 7-12 | Linea alba, pubic crest | Intercostal (T7-T12), Iliohypo/inguinal (L1) | Compresses abdominal contents |
| QUADRATUS LUMBORUM | Iliac crest | Last rib, transverse processes of L1-L4 | Lumbar Plexus (T12-L4) | Laterally flexes vertebral column |
| LEVATOR ANI GROUP | Pubis, ischial spine | Coccyx, walls of pelvic organs | Pudendal Nerve (S2-S4), S3-S4 | Supports pelvic organs, maintains continence |
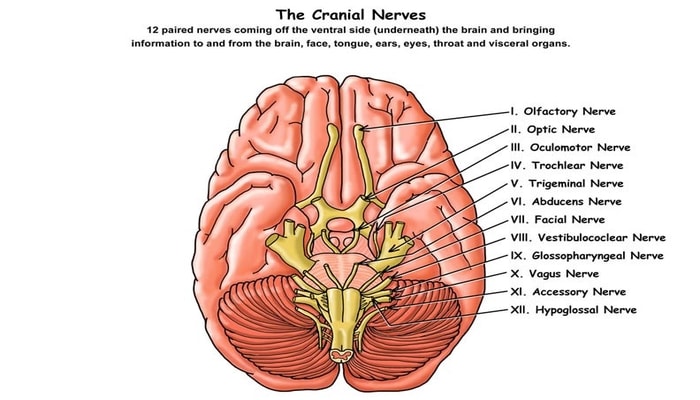
Reference: The 12 Cranial Nerves
The cranial nerves are a set of 12 paired nerves that arise directly from the brain and brainstem, as opposed to spinal nerves which emerge from the spinal cord. They are responsible for conveying sensory and motor information to and from the head and neck region, as well as controlling visceral functions.
Mnemonics for Memorization
For Nerve Names:
"Oh Oh Oh To Touch And Feel A Girls Vagina Ah Heaven"
For Functional Type (S=Sensory, M=Motor, B=Both):
"Some Say Marry Money, But My Brother Says Big Brains Matter More"
I. Olfactory Nerve
Function: Special sense of smell.
Clinical Test: Ask patient to identify common scents (e.g., coffee, vanilla) with each nostril closed.
II. Optic Nerve
Function: Special sense of vision.
Clinical Test: Test visual acuity (Snellen chart) and visual fields.
III. Oculomotor Nerve
Function: Controls most eye movements (up, down, medially), raises eyelid, and constricts pupil.
Clinical Test: Test eye movements (H-pattern); check for pupillary light reflex and eyelid drooping (ptosis).
IV. Trochlear Nerve
Function: Controls the superior oblique muscle, which moves the eye downward and inward.
Clinical Test: Ask patient to look down and in; damage can cause vertical double vision.
V. Trigeminal Nerve
Function: Sensory for the face (touch, pain, temperature) and Motor for muscles of mastication (chewing).
Clinical Test: Test facial sensation with a cotton wisp; ask patient to clench jaw and palpate masseter and temporalis muscles.
VI. Abducens Nerve
Function: Controls the lateral rectus muscle, which moves the eye laterally (abducts the eye).
Clinical Test: Ask patient to look to the side; damage can cause inability to look laterally and horizontal double vision.
VII. Facial Nerve
Function: Motor for muscles of facial expression, and Sensory for taste from the anterior two-thirds of the tongue.
Clinical Test: Ask patient to smile, frown, puff cheeks, and raise eyebrows. Damage causes facial paralysis (Bell's Palsy).
VIII. Vestibulocochlear Nerve
Function: Special senses of hearing (cochlear part) and balance/equilibrium (vestibular part).
Clinical Test: Test hearing (whisper test, Rinne/Weber tests); check for balance issues and vertigo.
IX. Glossopharyngeal Nerve
Function: Motor for swallowing, and Sensory for taste from the posterior one-third of the tongue and sensation from the pharynx.
Clinical Test: Check gag reflex; ask patient to say "ahhh" and watch for symmetrical uvula elevation.
X. Vagus Nerve
Function: The "wanderer"; provides parasympathetic motor innervation to most thoracic and abdominal viscera. Also motor to pharynx/larynx and sensory from the viscera.
Clinical Test: Check gag reflex and ability to swallow; assess for hoarseness.
XI. Accessory Nerve
Function: Controls the trapezius and sternocleidomastoid muscles.
Clinical Test: Ask patient to shrug shoulders (trapezius) and turn head against resistance (SCM).
XII. Hypoglossal Nerve
Function: Controls the intrinsic and extrinsic muscles of the tongue.
Clinical Test: Ask patient to stick out their tongue; it will deviate towards the side of the lesion.