Common Abnormalities: Teratology and Teratogenesis
Common Abnormalities: Teratology and Teratogenesis
1. Teratology
Teratology is the scientific study of abnormal physiological development, specifically focusing on the causes, mechanisms, and patterns of birth defects, also known as congenital malformations. The term comes from the Greek "teras," meaning monster or marvel.
Key Concepts in Teratology
Congenital Malformations (Birth Defects) are structural, functional, or metabolic abnormalities present at birth. These can range from minor cosmetic issues to severe, life-threatening conditions. Not all congenital conditions are visible at birth (e.g., some heart defects or metabolic disorders). They are classified into several distinct categories based on their origin.
Malformation
A primary structural defect resulting from an intrinsically abnormal developmental process. The blueprint itself was flawed from the beginning.
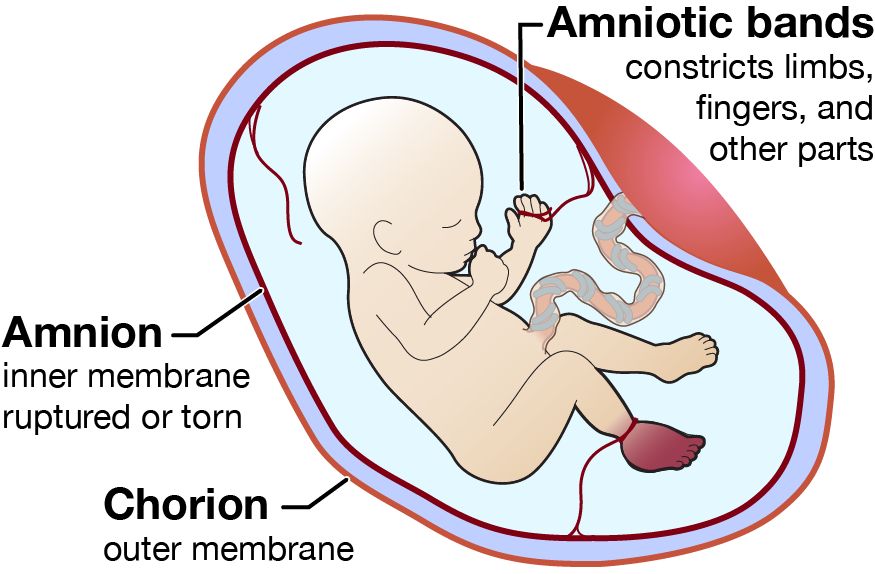
A defect resulting from the extrinsic breakdown of, or interference with, an originally normal developmental process. The blueprint was normal, but something damaged the structure as it was forming.
Example: Limb amputation due to amniotic bands wrapping around it.
Deformation
An abnormal form, shape, or position of a body part caused by extrinsic mechanical forces acting on a normally developed structure.
Example: Clubfoot due to intrauterine crowding, limiting space for the feet to grow properly.
Dysplasia
An abnormal organization of cells into tissues. The problem lies in how the cells themselves are structured and arranged.
Example: Skeletal dysplasias like achondroplasia (a form of dwarfism).
Syndrome
A group of anomalies that occur together and have a specific, common, known cause.
Example: Down syndrome (caused by Trisomy 21), Fetal Alcohol Syndrome.
Association
A non-random occurrence of two or more anomalies that appear together more often than by chance, but for which a common cause has not yet been identified.
Example: VACTERL association (Vertebral, Anal, Cardiac, Tracheo-Esophageal, Renal, Limb defects).
Factors Contributing to Birth Defects
While teratogens are a major focus, it's important to understand the broader categories of factors that can lead to congenital malformations.
Causes
40-50%: Unknown Causes
20-25%: Genetic Factors (chromosomal, single gene)
Teratogenesis is the process by which a teratogen (an agent that causes birth defects) acts on an embryo or fetus to produce a congenital malformation. The study of this process is governed by a set of foundational concepts known as Wilson's Principles.
Principle 1: Susceptibility (Genotype)
The genetic makeup of the embryo and mother determines their susceptibility to a teratogen. What harms one individual may have no effect on another due to genetic differences in metabolism and cellular repair.
Principle 2: Dosage & Duration
The amount of the teratogen and the length of exposure are critical. Generally, a higher dose or a longer duration of exposure increases the risk and severity of the resulting defect.
Principle 3: Timing of Exposure (Critical Periods)
This is arguably the most crucial principle. The susceptibility of an organ system to a teratogen varies dramatically with its stage of development.
Pre-implantation Period (Weeks 1-2)
The "all-or-nothing" period. Exposure to a teratogen usually results in either the death of the embryo or its complete recovery with no defects, as the cells are still totipotent and can be replaced.
Embryonic Period (Weeks 3-8)
The most sensitive period for major malformations. This is when organogenesis occurs, and each organ system has its own critical window of vulnerability (e.g., heart: weeks 3-5; CNS: weeks 3-16+).
Fetal Period (Weeks 9 to Birth)
Exposure during this period generally does not cause major structural defects but can lead to functional problems, growth retardation, and minor abnormalities, especially in the still-developing brain.
Principle 4: Mechanisms
Teratogens exert their effects through specific cellular and molecular mechanisms, such as interfering with cell proliferation or migration, inducing cell death (apoptosis), or disrupting biochemical pathways.
Principle 5: Manifestations
The final outcome of teratogenic exposure can be one of four manifestations: death, malformation, growth retardation, or functional deficit.
Classes of Teratogens
Teratogens are substances that can cause birth defects when a fetus is exposed during pregnancy. They can be broadly categorized into several classes, each with well-documented examples and associated defects. The risk and severity of abnormalities depend on the type of agent, timing, dosage, and duration of exposure.
Infectious Agents (TORCH Infections)
The acronym TORCH helps remember some of the most well-known infectious teratogens:
Toxoplasmosis: A parasitic infection that can cause hydrocephalus and intracranial calcifications.
Others (e.g., Syphilis, Varicella-Zoster, Zika, Parvovirus B19): Zika is known for causing microcephaly, while syphilis can lead to congenital deafness and other issues.
Rubella (German measles): Can result in a classic triad of cataracts, cardiac malformations, and deafness.
Cytomegalovirus (CMV): A common virus that can cause microcephaly, hearing loss, and intellectual disability.
Herpes Simplex Virus: Can lead to skin lesions, microcephaly, and eye problems.
Drugs and Chemicals
Thalidomide: A classic example that caused severe limb reduction defects (phocomelia).
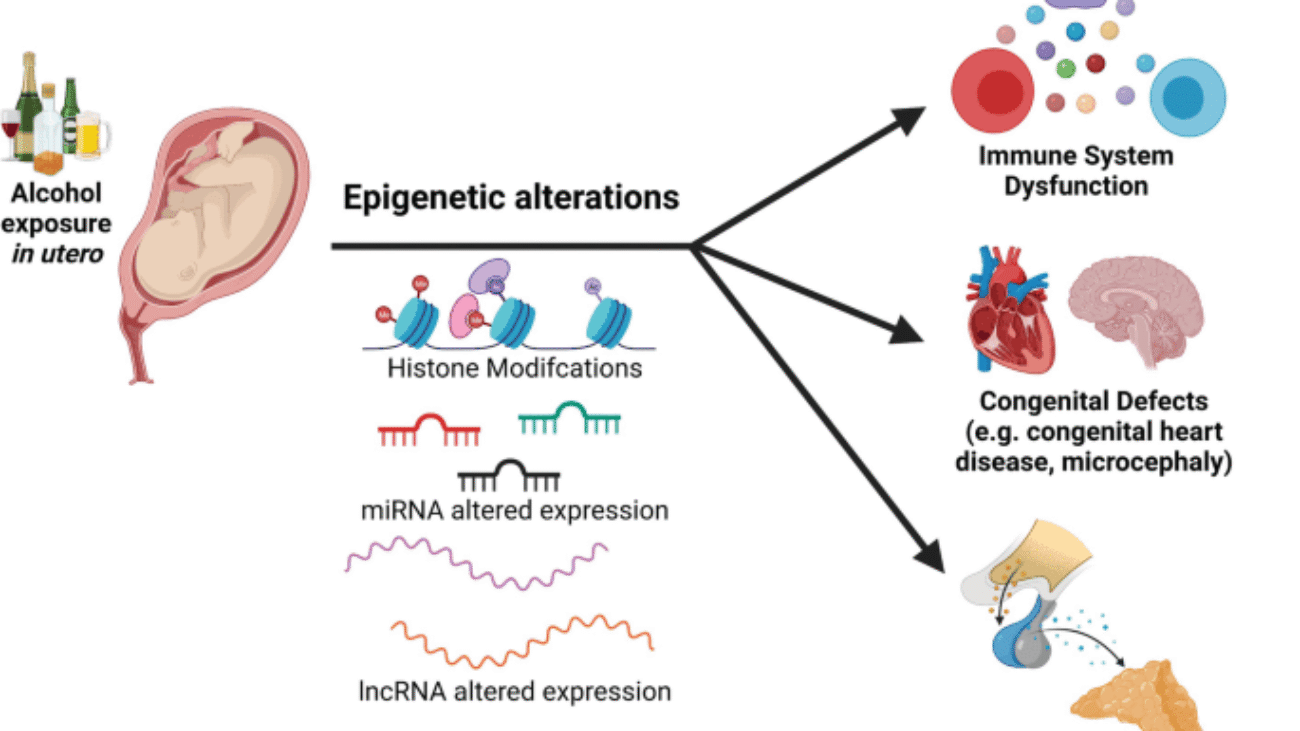
Alcohol (Ethanol): The leading preventable cause of non-genetic birth defects, leading to Fetal Alcohol Syndrome (FAS) with distinct facial anomalies, growth retardation, and CNS dysfunction.
Tobacco & Nicotine: Smoking is associated with low birth weight, premature delivery, and can affect the development of the fetal brain and lungs.
Retinoids (e.g., Isotretinoin/Accutane): Highly teratogenic, causing severe CNS, facial, cardiac, and ear malformations.
Anticonvulsants (e.g., Valproic Acid, Phenytoin): Associated with neural tube defects, cleft lip/palate, and cardiac defects.
ACE Inhibitors: Can cause renal failure and oligohydramnios (insufficient amniotic fluid).
Warfarin: An anticoagulant that can cause skeletal abnormalities, including chondrodysplasia punctata.
Certain Antibiotics (e.g., Tetracycline): Can cause yellow staining of teeth and affect long bone growth.
Recreational Drugs (e.g., Cocaine, Heroin): Can lead to low birth weight, withdrawal symptoms in the newborn, and learning or behavioral problems.
Environmental Toxins
Heavy Metals (e.g., Mercury, Lead): Can cause significant CNS damage and developmental delays. Mercury is often found in certain types of fish, and lead can be in old paint and pipes.
Polychlorinated Biphenyls (PCBs): Industrial chemicals that can lead to developmental and neurological problems.
Herbicides and Industrial Solvents: Exposure to certain chemicals used in agriculture and manufacturing can be harmful.
Physical Agents
Ionizing Radiation (e.g., X-rays, Radiation Therapy): High doses can cause microcephaly, intellectual disability, and growth restriction.
Hyperthermia: Prolonged high body temperature from fever or use of hot tubs and saunas in early pregnancy can increase the risk for neural tube defects.
Maternal Factors & Metabolic Conditions
Maternal Diabetes Mellitus (poorly controlled): High blood sugar levels can increase the risk of cardiac defects, neural tube defects, and caudal regression syndrome.
Maternal Phenylketonuria (PKU): Uncontrolled high phenylalanine levels are highly teratogenic to the fetal brain.
Maternal Obesity: Associated with a higher risk of neural tube defects and cardiac anomalies.
Nutritional Deficiencies: Folic acid deficiency is a major, preventable cause of neural tube defects like spina bifida.
Autoimmune Diseases (e.g., Lupus): The condition itself or the medications used for treatment can pose risks.
Prevention and Management
While not all birth defects are preventable, proactive measures can significantly reduce their incidence and impact.
Preconception Counseling: Discussing risks like chronic health conditions and medications with a healthcare provider before becoming pregnant is ideal.
Folic Acid Supplementation: Taking a daily prenatal vitamin with at least 400 micrograms of folic acid is a highly effective measure for preventing neural tube defects.
Avoidance of Known Teratogens: This includes abstaining from alcohol, smoking, and recreational drugs, as well as being cautious with medications and chemical exposures.
Vaccinations: Ensuring immunizations, such as for rubella, are up to date can prevent congenital infections.
Regular Prenatal Care: Utilizing prenatal tools like ultrasounds and maternal serum screening helps in the early identification of potential issues.
Managing Health Conditions: Actively managing chronic conditions like diabetes or thyroid issues is crucial during pregnancy.
Chromosomal Abnormalities
These abnormalities result from errors in chromosome number (aneuploidy) or structure. They are often severe and can affect multiple organ systems, leading to distinct syndromes.
A. Aneuploidies (Abnormal Number of Chromosomes)
Aneuploidies are typically caused by non-disjunction—the failure of chromosomes to separate properly during meiosis.
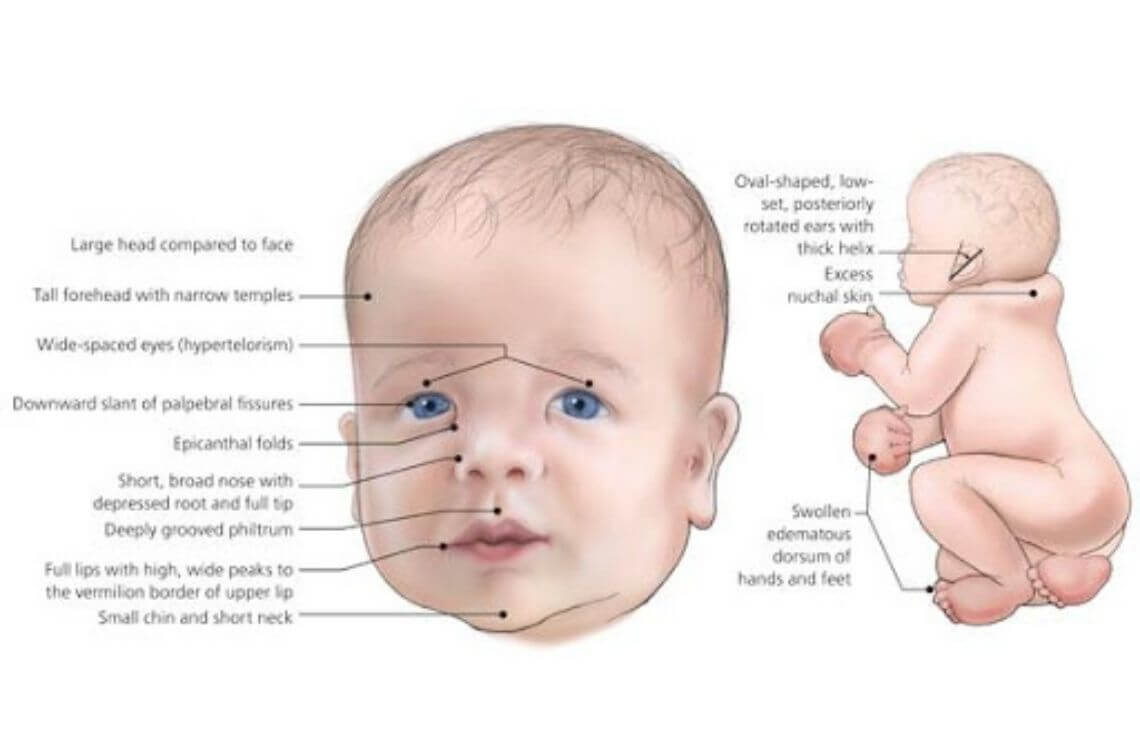
Down Syndrome (Trisomy 21)
Cause: An extra copy of chromosome 21 (47, XX/XY, +21). Incidence: ~1 in 700 live births; risk increases with maternal age.
Intellectual Disability: Mild to moderate severity.
Congenital Heart Defects: Very common (e.g., AV septal defect).
Other Signs: Hypotonia (poor muscle tone), single palmar crease, increased risk of leukemia and early-onset Alzheimer's.
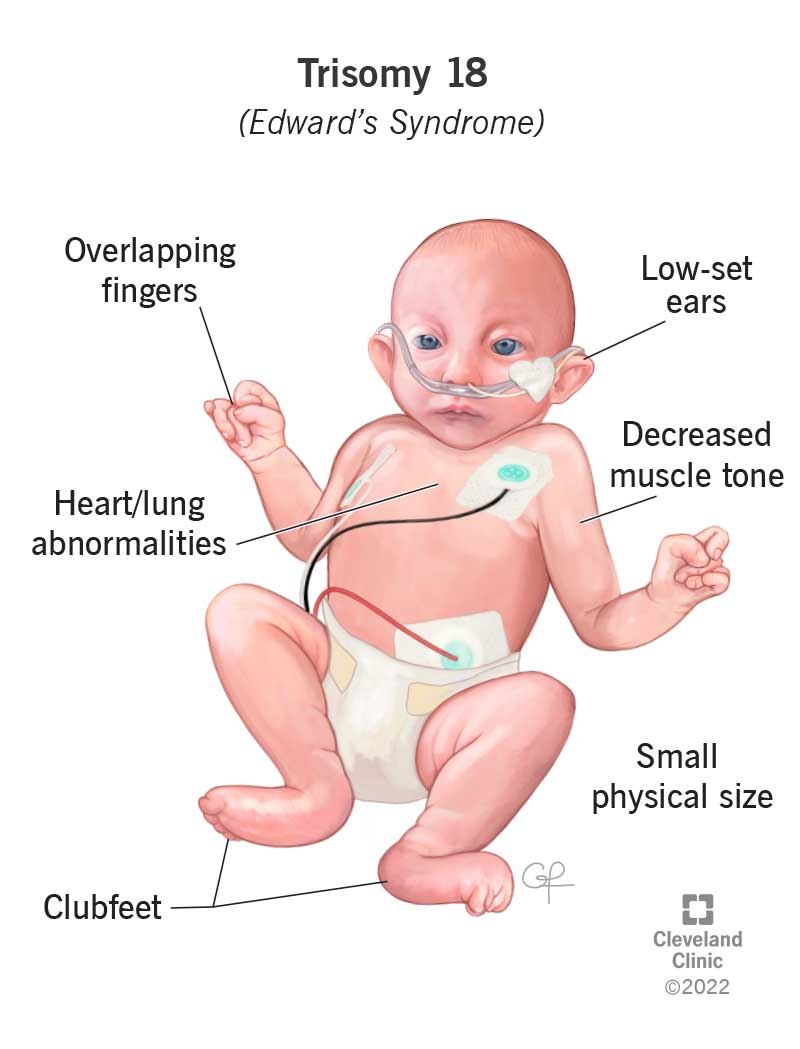
Edward Syndrome (Trisomy 18)
Cause: An extra copy of chromosome 18 (47, XX/XY, +18). Incidence: ~1 in 5,000 live births; severe prognosis.
Key Features:
Severe Intellectual Disability & Growth Retardation.
Characteristic Physical Features: Small head (microcephaly), small jaw (micrognathia), low-set ears, clenched hands with overlapping fingers, rocker-bottom feet.
Major Organ Defects: Severe heart and kidney malformations.
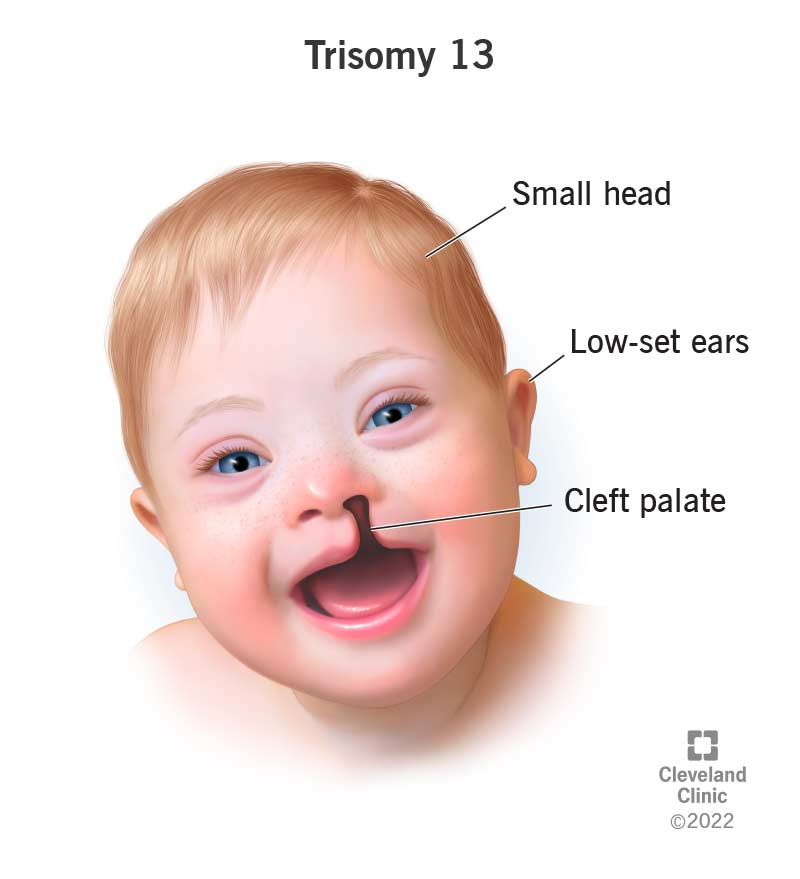
Patau Syndrome (Trisomy 13)
Cause: An extra copy of chromosome 13 (47, XX/XY, +13). Incidence: ~1 in 16,000 live births; severe prognosis.
Key Features:
Major CNS Malformations: Holoprosencephaly (failure of forebrain to divide).
Facial Anomalies: Cleft lip and/or palate, small or absent eyes.
Polydactyly (extra fingers or toes).
Severe heart and renal defects.
Turner Syndrome (Monosomy X)
Cause: Affects females; absence of one X chromosome (45, XO). Incidence: ~1 in 2,500 live female births.
Key Features:
Short Stature and Webbed Neck.
Ovarian Dysgenesis: Underdeveloped ovaries leading to infertility.
Broad Chest with widely spaced nipples.
Heart Defects: Coarctation of the aorta is common.
Normal intelligence, but may have specific spatial learning difficulties.
Klinefelter Syndrome
Cause: Affects males; an extra X chromosome (47, XXY). Incidence: ~1 in 500-1,000 live male births.
Key Features:
Tall Stature.
Hypogonadism: Small testes, leading to infertility and reduced testosterone.
Gynecomastia (breast development).
Increased risk of learning difficulties (often language-based).
Frequently undiagnosed until puberty or an infertility workup.
B. Structural Chromosomal Abnormalities
These involve changes in the structure of a chromosome, such as deletions, duplications, or translocations. An important example is:
Cri-du-chat Syndrome
Caused by a deletion on the short arm of chromosome 5. It is characterized by severe intellectual disability, microcephaly, and a distinctive high-pitched, cat-like cry in infancy.
2. Single-Gene (Monogenic) Disorders
These disorders result from a mutation in a single gene and typically follow predictable Mendelian patterns of inheritance.
A. Autosomal Dominant Conditions
Only one copy of the mutated gene (from either parent) is needed to express the disease.
Achondroplasia
Cause: Mutation in the FGFR3 gene. Key Features: The most common cause of dwarfism (short-limbed), characterized by a large head (macrocephaly) and prominent forehead. Intelligence is typically normal.
Marfan Syndrome
Cause: Mutation in the FBN1 gene (codes for fibrillin-1, a key connective tissue protein). Key Features: Affects connective tissue. Leads to tall stature, long limbs, hypermobile joints, and severe cardiovascular complications (aortic aneurysm).
Huntington's Disease
Cause: Expansion of a CAG trinucleotide repeat in the HTT gene. Key Features: A progressive neurodegenerative disorder with motor, cognitive, and psychiatric symptoms, typically with an onset in mid-adulthood.
B. Autosomal Recessive Conditions
Two copies of the mutated gene (one from each carrier parent) are needed to express the disease.
Cystic Fibrosis (CF)
Cause: Mutation in the CFTR gene, affecting chloride channels. Key Features: Production of thick, sticky mucus that primarily damages the lungs and pancreas, leading to chronic respiratory infections and malabsorption.
Phenylketonuria (PKU)
Cause: Mutation in the PAH gene, leading to an enzyme deficiency. Key Features: Inability to metabolize the amino acid phenylalanine. If untreated, it leads to severe intellectual disability. Managed by a strict diet and detectable by newborn screening.
Sickle Cell Anemia
Cause: Point mutation in the beta-globin gene (HbS). Key Features: Red blood cells become sickle-shaped, causing painful vaso-occlusive crises, anemia, and organ damage. Common in populations from malaria-endemic regions.
C. X-Linked Recessive Conditions
Caused by a mutation on the X chromosome. Primarily affects males, as they have only one X chromosome. Females with one mutated copy are typically carriers.
Duchenne Muscular Dystrophy (DMD)
Cause: Mutation in the DMD gene, leading to an absence of the dystrophin protein. Key Features: Progressive muscle wasting and weakness, leading to loss of ambulation in early teens and eventual respiratory and cardiac failure.
Hemophilia A and B
Cause: Deficiency of clotting Factor VIII (Hemophilia A) or Factor IX (Hemophilia B). Key Features: Impaired blood clotting, leading to spontaneous or prolonged bleeding, especially into joints and muscles.
3. Multi-factorial & Environmental Abnormalities
This complex category includes some of the most common birth defects. They are caused by an intricate interplay of multiple genes and environmental factors, or are the direct result of a specific environmental exposure (teratogen).
A. Neural Tube Defects (NTDs)
Malformations of the brain or spinal cord from incomplete neural tube closure during weeks 3-4.
Common Types:
Spina Bifida: Incomplete closure of the vertebral column, potentially exposing the spinal cord and causing paralysis or bladder/bowel dysfunction.
Anencephaly: Failure of the cranial end to close, resulting in the absence of a major portion of the brain and skull. This condition is always lethal.
Prevention: Periconceptional folic acid supplementation significantly reduces the risk.
B. Cleft Lip and/or Palate
A congenital split in the upper lip and/or the roof of the mouth (palate).
Causes & Impact:
Caused by a mix of genes and environmental factors (e.g., smoking, certain medications). It can lead to difficulties with feeding, speech, and dental development, and requires surgical repair.
C. Congenital Heart Defects (CHDs)
The most common type of birth defect, involving abnormalities in the heart's structure.
Common Types:
Ventricular Septal Defect (VSD): A hole between the lower chambers.
Atrial Septal Defect (ASD): A hole between the upper chambers.
Patent Ductus Arteriosus (PDA): Failure of a fetal blood vessel to close after birth.
Tetralogy of Fallot: A complex defect involving four distinct abnormalities.
D. Fetal Alcohol Syndrome (FAS)
Caused by maternal alcohol consumption during pregnancy.
Key Features:
Facial Anomalies: Short palpebral fissures, a thin upper lip, and a smooth philtrum.
Growth Retardation.
Central Nervous System Abnormalities: Intellectual disability and behavioral problems.
Prevention: Complete abstinence from alcohol during pregnancy.
E. Congenital Rubella Syndrome (CRS)
Caused by maternal infection with the rubella virus during early pregnancy.
Key Features (Classic Triad):
Ocular Defects: Cataracts.
Cardiac Defects: Patent ductus arteriosus (PDA).
Sensorineural Deafness.
Prevention: MMR vaccination of women prior to pregnancy.
Test Your Knowledge
Check your understanding of the concepts covered in this post.
1. Which of the following terms describes a birth defect resulting from an extrinsically caused breakdown of an originally normal developmental process, such as limb amputation due to amniotic bands?
Malformation
Deformation
Dysplasia
Disruption
Rationale: Disruption specifically refers to a morphological defect resulting from the extrinsically caused breakdown of an originally normal developmental process, fitting the amniotic band example.
2. During which period of embryonic/fetal development is the conceptus most sensitive to major structural malformations due to teratogen exposure?
Pre-implantation Period (Weeks 1-2)
Embryonic Period (Weeks 3-8)
Fetal Period (Weeks 9 to birth)
Post-natal Period
Rationale: The Embryonic Period (Weeks 3-8) is the most sensitive period for major malformations because organogenesis (the formation of organs) occurs during this time.
3. According to Wilson's Principles of Teratogenesis, what is the most crucial factor determining the susceptibility of an organ system to a teratogen?
The mother's age
The duration of exposure
The timing of exposure (Critical Periods)
The father's genetic makeup
Rationale: The timing of exposure is perhaps the most crucial principle, as the susceptibility of an organ to damage varies significantly depending on its stage of development.
4. A significant proportion (40-50%) of birth defects fall into which causative category?
Genetic Factors
Environmental Factors
Multi-factorial Inheritance
Unknown Causes
Rationale: A significant proportion of birth defects have no clearly identifiable cause, falling into the "Unknown" category.
5. Which teratogen is the leading preventable cause of birth defects, characterized by facial anomalies, growth retardation, and CNS dysfunction?
Thalidomide
Isotretinoin
Alcohol (Ethanol)
Valproic Acid
Rationale: Alcohol is the leading preventable cause of birth defects and is associated with Fetal Alcohol Syndrome (FAS).
6. A group of anomalies occurring together that have a common cause is best described as a:
Association
Syndrome
Malformation
Deformation
Rationale: A syndrome is defined as a group of anomalies occurring together that have a common, known cause.
7. Exposure to a teratogen during the "all or nothing" period (Weeks 1-2 post-fertilization) most commonly results in which outcome?
Major structural malformations
Functional deficits and growth retardation
Either embryonic death or complete recovery without defects
Minor cosmetic issues
Rationale: During the pre-implantation "all or nothing" period, exposure to a teratogen usually results in either the death of the embryo or its complete recovery with no defects.
8. Which of the following maternal factors/metabolic conditions is strongly associated with an increased risk of neural tube defects if poorly controlled?
Maternal Phenylketonuria (PKU)
Maternal Diabetes Mellitus
Maternal Obesity
All of the above
Rationale: Poorly controlled maternal diabetes mellitus significantly increases the risk of various defects, including cardiac and neural tube defects.
9. Which infectious agent is known to cause microcephaly and is primarily associated with the Zika virus?
Toxoplasmosis
Rubella
Cytomegalovirus
Zika virus
Rationale: Infection with the Zika virus during pregnancy is a known cause of severe microcephaly in newborns.
10. The classic triad of cataracts, cardiac malformations, and deafness is associated with maternal exposure to which teratogenic infection?
Cytomegalovirus (CMV)
Rubella
Toxoplasmosis
Herpes Simplex Virus
Rationale: Rubella (German measles) infection during pregnancy can cause the classic triad of cataracts, cardiac malformations, and deafness in the fetus.
11. The scientific study of abnormal physiological development, focusing on the causes and patterns of birth defects, is known as ______________.
Rationale:teratology; This is the direct definition for the study of the causes and patterns of birth defects.
12. The process by which an agent acts on an embryo or fetus to produce a congenital malformation is called ______________.
Rationale: teratogenesis; This is the specific term for the process of an agent causing a congenital malformation.
13. ______________ is a birth defect caused by extrinsic mechanical forces, such as clubfoot due to intrauterine crowding.
Rationale: Deformation is defined as an abnormal form caused by extrinsic mechanical forces like intrauterine crowding.
14. The period during which organogenesis occurs (Weeks 3-8 post-fertilization) is also known as the ______________ period.
Rationale:embryonic; Weeks 3-8 post-fertilization, the time of organ formation, is defined as the Embryonic Period.
15. ______________ supplementation is crucial for preventing neural tube defects.
Rationale: Folic acid (a B vitamin) supplementation before and during early pregnancy is a well-established preventive measure for neural tube defects.
Fetal Membranes, Placenta, Cord and Circulation: Safety and Feeding
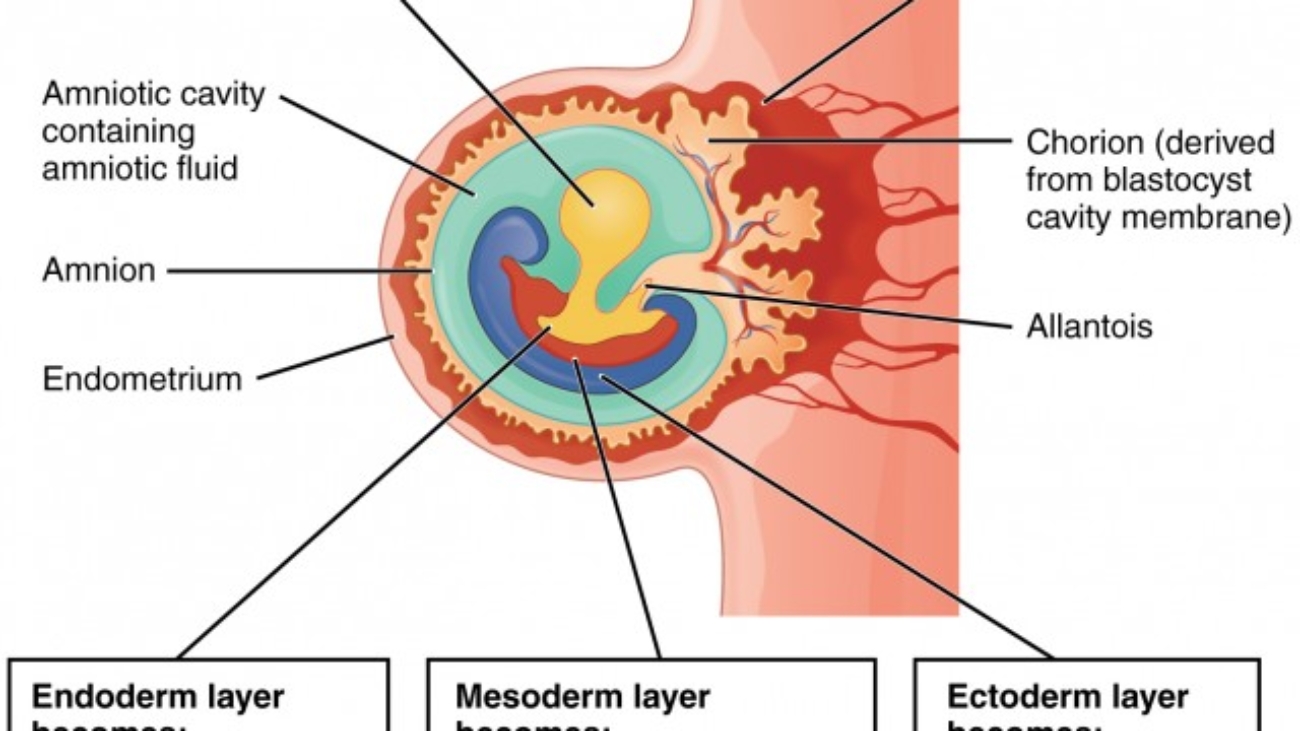
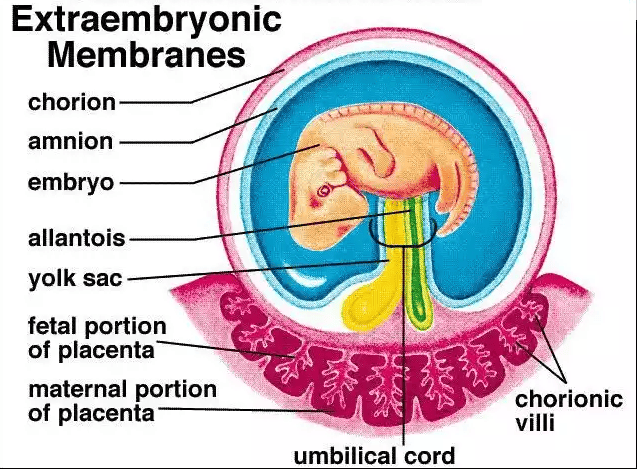
The Fetal Membranes and Placenta
The fetal membranes and the placenta are temporary, yet essential, organs that develop alongside the embryo and fetus. They provide a complete life-support system, handling protection, nourishment, gas exchange, waste removal, and hormonal regulation critical for successful intrauterine development. They are expelled from the body after birth.
Formation of Embryonic Cavities and Membranes
The period of early embryonic development (roughly Day 8 to Day 12-14 post-fertilization) is characterized by the rapid formation of several extraembryonic structures, which are vital for the embryo's survival and subsequent development. These include the amniotic cavity, primary and secondary yolk sacs, and the chorionic cavity, along with their associated membranes.
A. Formation of the Amniotic Cavity and Amnion
Timeline: Begins around Day 8 post-fertilization.
Process:
Cavity Formation: As the blastocyst implants, a small space appears within the epiblast, which is the dorsal layer of the bilaminar germ disc (formed from the Inner Cell Mass).
Enlargement: This space rapidly expands to become the amniotic cavity.
Amnioblast Differentiation: Cells from the epiblast adjacent to the cytotrophoblast differentiate into thin, flattened cells called amnioblasts.
Amniotic Membrane Formation: These amnioblasts, along with a layer of extraembryonic mesoderm, form the amnion, which eventually encloses the entire amniotic cavity.
Roof and Floor: The roof is formed by the amnion/cytotrophoblast, while the floor is formed by the epiblast of the bilaminar germ disc.
Key Features & Function of the Amnion/Amniotic Fluid:
Amniotic Sac
The amnion forms the inner lining of the amniotic sac, which will eventually surround the entire embryo and then fetus.
Amniotic Fluid
The cavity fills with amniotic fluid, serving crucial functions:
Protection: Acts as a shock absorber.
Temp Regulation: Maintains constant temperature.
Symmetry & Movement: Allows movement for musculoskeletal development.
Prevents Adhesion: Stops embryo from sticking to amnion.
Lung/GI Development: Fetal swallowing aids GI tract; "breathing" movements aid lungs.
B. Formation of the Yolk Sac
Timeline: Primary yolk sac begins around Day 9; Secondary yolk sac around Day 12-13.
1. Primary Yolk Sac (Exocoelomic Cavity) - Day 9
Cells from the hypoblast (ventral layer) migrate and line the inner surface of the cytotrophoblast.
These cells form a thin membrane called the exocoelomic membrane (Heuser's membrane).
This membrane + hypoblast encloses the primary yolk sac.
Position: Bilaminar disc lies between Amniotic Cavity (dorsal) and Primary Yolk Sac (ventral).
2. Extraembryonic Mesoderm - Day 10-11
A new layer of loose connective tissue appears and fills the space between the exocoelomic membrane/amnion externally and the cytotrophoblast internally.
3. Secondary Yolk Sac (Definitive) - Day 12-13
Primary sac constricts due to chorionic cavity expansion.
A smaller, definitive secondary yolk sac forms from a portion of the primary. The larger pinched-off part degenerates.
Key Features & Function of the Yolk Sac:
Early Nutrient Transfer
Plays a role before uteroplacental circulation is functional.
Hematopoiesis
Primary site of early blood cell formation (Weeks 3-6) before the liver takes over.
Primordial Germ Cells
Precursors to sperm/eggs originate here and migrate to gonads.
Vestigial Structure
In humans, it is small, regresses, and incorporates into the umbilical cord.
C. Formation of the Chorionic Cavity and Chorion
Timeline: Begins around Day 11-12.
Process:
Vacuole Formation: Numerous large spaces and vacuoles appear within the extraembryonic mesoderm.
Coalescence: These fuse to form a large, isolated cavity called the chorionic cavity (extraembryonic coelom).
Suspension of Embryo: The embryo (with amnion/yolk sac) is suspended in this cavity by the connecting stalk (future umbilical cord).
The Chorion (Outer Wall)
Formed by three layers:
Syncytiotrophoblast (outermost)
Cytotrophoblast
Somatic layer of extraembryonic mesoderm (innermost)
Functions:
Chorionic Villi: Gives rise to villi (functional units of placenta).
Protection: Additional protective layer.
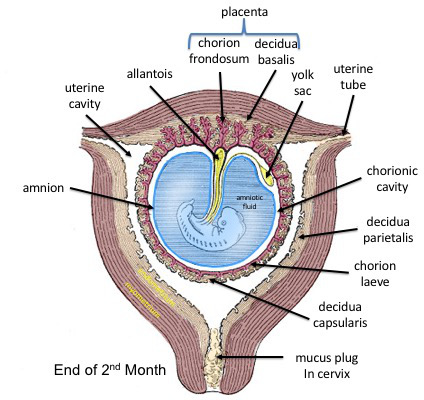
Part of Placenta: The chorion frondosum forms the fetal component.
Summary of Relationships (Day 12-14):
Bilaminar germ disc centrally located.
Dorsal: Amniotic cavity.
Ventral: Secondary yolk sac.
Surrounding all: Chorionic cavity (enclosed by Chorion).
Bridge: Connecting stalk linking disc to chorion.
The Allantois: Development and Significance
Origin: Appears around Day 16-18 as a small, sausage-shaped diverticulum (outpouching) from the caudal wall of the yolk sac (hindgut) extending into the connecting stalk.
Vascular Development
The most significant role in humans. Blood vessels develop in its wall to become the umbilical arteries and umbilical vein.
These extend through the connecting stalk to link embryonic and placental circulation.
Urinary Bladder Formation
The proximal part incorporates into the developing urinary bladder.
The connection (urachus) obliterates postnatally to form the median umbilical ligament. Anomalies can lead to cysts/fistulas.
Regression & Relationship to Umbilical Cord
In humans, the allantois is largely vestigial. As the amniotic cavity expands and forms the definitive umbilical cord, the allantois regresses into a fibrous cord within it, while its vessels remain as the vital umbilical vessels.
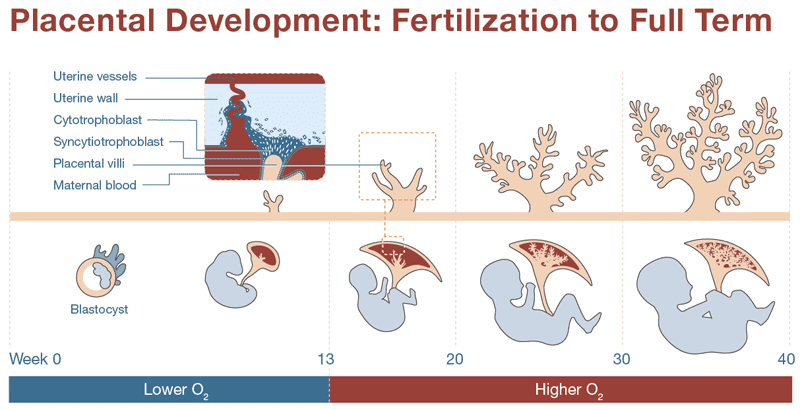
The Placenta
The placenta is a composite, temporary organ formed by both fetal tissues (the chorionic villi) and maternal tissues (the decidua basalis of the endometrium). It serves as the complete life-support system for the fetus and is also a critical endocrine organ during pregnancy.
A. Development of the Placenta
The placenta begins to form as soon as the blastocyst implants, with the trophoblast rapidly differentiating and invading the uterine wall.
Chorionic Villi Formation
The fetal portion of the placenta develops through three stages of villi:
Primary Villi: Columns of cytotrophoblast penetrate the syncytiotrophoblast.
Secondary Villi: Mesenchyme (connective tissue) invades the core of the primary villi.
Tertiary Villi: Fetal blood vessels develop within the mesenchymal core, establishing the feto-placental circulation.
B. Functions of the Placenta
The placenta is a multi-functional powerhouse, acting as the fetus's lungs, kidneys, GI tract, and endocrine gland.
Metabolic Functions
Synthesizes glycogen, fatty acids, and cholesterol, and actively transports essential nutrients like glucose, amino acids, and vitamins from mother to fetus.
Gas Exchange
Transfers oxygen from maternal blood to fetal blood and transfers carbon dioxide from fetal blood to maternal blood, acting as the fetal lungs.
Waste Removal
Excretes fetal metabolic waste products (urea, uric acid, creatinine) into the maternal bloodstream for disposal by the mother's kidneys.
Hormone Production
hCG: Maintains the corpus luteum in early pregnancy.
Progesterone: Maintains the pregnancy and keeps the uterus relaxed.
Estrogens: Promote uterine and mammary gland growth.
hPL: Modifies maternal metabolism to support fetal energy needs.
Immunological Barrier
Allows passive immunity by transferring maternal antibodies (IgG) to the fetus. It also acts as a partial barrier, though many harmful substances (drugs, viruses, alcohol) can cross it.
C. The Placental Barrier
This is not a true barrier but rather a highly selective membrane across which all exchange occurs. It consists of four layers initially, which thin out as pregnancy progresses to increase efficiency:
Syncytiotrophoblast
Cytotrophoblast (thins out later)
Connective tissue of the villus core
Endothelium of the fetal capillaries
Functions of the Placenta
The placenta is a transient but indispensable organ that acts as the lifeline between the mother and the developing fetus. It performs multiple critical functions, broadly categorized into metabolic, transfer (gas, nutrient, waste), barrier, and endocrine (hormonal) roles.
I. Metabolic Functions
The placenta is a metabolically active organ, performing synthesis, storage, and transfer of various substances essential for both fetal development and maternal adaptation to pregnancy.
Synthesis and Storage
Glycogen Synthesis & Storage: The placenta actively synthesizes and stores glycogen (a polymer of glucose), especially in early pregnancy. This serves as a readily available energy reserve for the growing embryo/fetus when maternal glucose supply might be fluctuating or insufficient, particularly before the fetal liver is fully mature.
Cholesterol Synthesis: The placenta synthesizes cholesterol, which is a precursor for steroid hormone production (estrogens, progesterone). While it can utilize maternal cholesterol, its own synthetic capacity is important.
Fatty Acid Synthesis: The placenta can synthesize some fatty acids, which are crucial for fetal membrane development and energy.
Protein Synthesis: The placenta synthesizes various proteins, including structural proteins for its own growth and enzymes required for its metabolic activities. It also synthesizes some growth factors and cytokines.
Nutrient Transfer (Feeding the Fetus)
The placenta acts as the primary organ for transferring nutrients from the maternal circulation to the fetal circulation.
1. Glucose
Mechanism: Primarily facilitated diffusion via glucose transporters (GLUTs), especially GLUT1, located on both maternal and fetal sides of the syncytiotrophoblast.
How it Works: Maternal glucose levels directly influence fetal glucose supply. The fetus relies almost entirely on maternal glucose for its energy needs. The placenta extracts glucose from maternal blood and passes it efficiently to the fetal side.
2. Amino Acids
Mechanism: Primarily active transport, requiring energy. There are multiple amino acid transporter systems (e.g., A, L, ASC systems) on the syncytiotrophoblast.
How it Works: Fetal amino acid concentrations are generally higher than maternal concentrations, demonstrating the active "pumping" action of the placenta. These are crucial for fetal protein synthesis, growth, and development.
3. Fatty Acids & Lipids
Mechanism: Simple diffusion for smaller fatty acids; facilitated diffusion and receptor-mediated endocytosis for larger fatty acids and cholesterol. Lipoprotein lipase in the placenta hydrolyzes maternal triglycerides.
How it Works: Essential fatty acids (e.g., omega-3 and omega-6) are vital for fetal brain and retinal development. Lipids are also a major source of energy and structural components for fetal cell membranes.
4. Vitamins
Mechanism: Simple/facilitated diffusion and active transport.
How it Works: All fat-soluble (A, D, E, K) and water-soluble vitamins cross. Active transport ensures higher concentrations of some water-soluble vitamins in the fetus.
5. Minerals
Mechanism: Primarily active transport (Iron, Calcium, Phosphorus).
How it Works: Iron is actively transported for erythropoiesis. Calcium/Phosphorus are crucial for skeletal mineralization.
II & III. Gas Exchange and Waste Excretion
Gas Exchange (O₂ & CO₂)
Mechanism: Simple diffusion, driven by partial pressure gradients.
Oxygen: Diffuses from maternal blood → fetal blood. Fetal hemoglobin (HbF) has a higher affinity for O₂ than adult HbA, facilitating uptake even at lower pressures.
Carbon Dioxide: Fetal blood (high CO₂) releases it into maternal blood (lower CO₂). Maternal lungs exhale it.
Waste Excretion
Substances: Urea, Creatinine, Uric Acid.
Mechanism: Primarily simple diffusion, driven by concentration gradients.
These metabolic waste products generated by the fetus are transferred to maternal blood. The maternal kidneys then excrete them.
IV. Barrier Function (Protective Role)
The placenta acts as a selective barrier, protecting the fetus from potentially harmful substances while allowing essential nutrients to pass. However, it is not an impenetrable barrier.
1. Antibodies (Immunological Protection)
Mechanism: Active transport via Fc receptors (FcRn) on the syncytiotrophoblast.
How it Works: Only maternal IgG antibodies are actively transported (predominantly 3rd trimester). This provides passive immunity against many diseases (measles, rubella, tetanus). IgM, IgA, IgD, IgE do not cross significantly.
2. TORCHES Infections (Barrier Failure)
The placenta is generally effective against bacteria, but the "TORCHES" group can cross and cause severe congenital defects:
Toxoplasmosis
Other (Syphilis, Varicella, Parvovirus B19, Zika, Listeria)
Rubella
Cytomegalovirus (CMV)
Herpes Simplex Virus (HSV)
Enteroviruses
Syphilis / Strep (Group B)
3. Drugs and Toxins
Most drugs, alcohol, nicotine, and environmental toxins (lead, mercury) can cross via diffusion. While the placenta metabolizes some, many are teratogens leading to malformations.
4. Maternal Thyroid Hormones
Maternal T3/T4 cross via active transport (early pregnancy). Crucial for early fetal brain development before the fetal thyroid is functional.
V. Hormonal (Endocrine) Functions
The placenta is a crucial endocrine organ, producing a wide array of hormones that regulate maternal physiology, maintain pregnancy, and promote fetal growth.
A. Protein Hormones
hCG (Human Chorionic Gonadotropin)
Source: Syncytiotrophoblast.
Maintains Corpus Luteum: Acts like LH to sustain progesterone/estrogen production (preventing menstruation) in early pregnancy (up to ~7-10 weeks).
Pregnancy Test: Basis of maternal blood/urine tests.
Fetal Testes: Stimulates testosterone production for male differentiation.
hPL (Human Placental Lactogen)
Source: Syncytiotrophoblast.
Metabolic Adaptation: Anti-insulin effect; decreases maternal glucose use, diverting it to the fetus.
Lipolysis: Mobilizes maternal fatty acids for energy.
Mammary Glands: Stimulates growth for lactation.
Fetal Growth: Indirectly promotes growth.
CRH (Corticotropin-Releasing Hormone)
"Placental Clock": Rising levels in late pregnancy may trigger labor.
Pelvic Relaxation: Softens ligaments/pubic symphysis for childbirth.
Cervical Ripening: Aids dilation/effacement.
Uterine Quiescence: Relaxes uterine muscle.
B. Steroid Hormones
The placenta is a major site of steroid hormone synthesis, often utilizing precursors from both maternal and fetal sources (the "feto-placental unit").
1. Progesterone
Source: Syncytiotrophoblast (primary source from 7-10 weeks).
Contractility: Increases myometrial sensitivity to oxytocin (towards term).
The Umbilical Cord: The Fetal Lifeline
The umbilical cord develops from the connecting stalk and serves as the vital connection between the fetus and the placenta, facilitating all exchange.
Two Umbilical Arteries
Carry deoxygenated blood and waste from the fetus to the placenta.
One Umbilical Vein
Carries oxygenated blood and nutrients from the placenta to the fetus.
Wharton's Jelly
A gelatinous connective tissue that surrounds and protects the vessels from compression.
Fetal Circulation
In utero, the fetus relies entirely on the placenta for respiration, nutrition, and excretion, as its lungs and GI tract are non-functional. Fetal circulation is ingeniously designed with a series of shunts to accommodate this reality, ensuring the most highly oxygenated blood reaches the most critical organs.
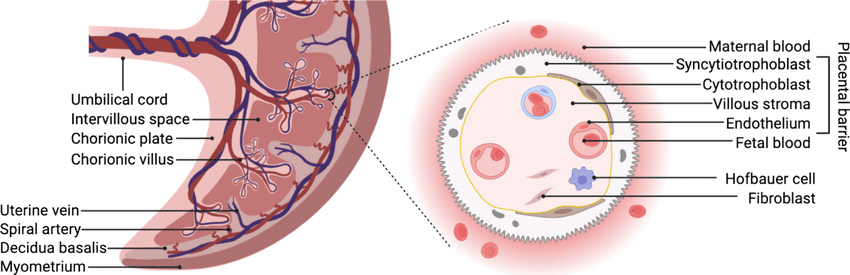
The Pathway of Fetal Blood Flow
1. Oxygenated Blood from Placenta: Rich blood flows to the fetus via the single umbilical vein.
2. Bypassing the Liver: About 50% of this blood bypasses the liver through the ductus venosus to enter the Inferior Vena Cava (IVC).
3. Bypassing the Lungs (First Shunt): In the right atrium, most of this oxygenated blood is shunted directly to the left atrium through the foramen ovale.
4. Supplying Vital Organs: From the left heart, this highly oxygenated blood is pumped into the aorta to supply the heart and brain first.
5. Bypassing the Lungs (Second Shunt): Deoxygenated blood from the upper body enters the right heart and is pumped into the pulmonary artery. Most of it is shunted away from the high-resistance lungs, through the ductus arteriosus, into the descending aorta.
6. Return to Placenta: Deoxygenated blood from the descending aorta flows into the two umbilical arteries and travels back to the placenta for re-oxygenation.
Summary & Mnemonic
A simple way to remember the key structures in order:
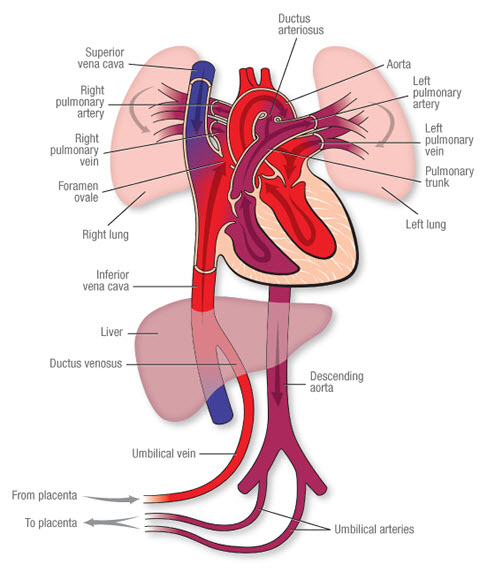
Changes After Birth: Adaptation to Extrauterine Life
At birth, with the first breath and the clamping of the umbilical cord, a series of rapid and profound physiological changes occur to transition the circulatory system from fetal to adult patterns.
Closure of Fetal Shunts
The onset of respiration increases pressure in the left atrium, closing the flap-like foramen ovale. Increased oxygen levels and changes in prostaglandins cause the muscular walls of the ductus arteriosus and ductus venosus to constrict and close.
Formation of Ligaments (Remnants)
Umbilical Vein → Ligamentum Teres (in the falciform ligament of the liver).
Ductus Venosus → Ligamentum Venosum.
Foramen Ovale → Fossa Ovalis.
Ductus Arteriosus → Ligamentum Arteriosum.
Umbilical Arteries → Medial Umbilical Ligaments.
Test Your Knowledge
Check your understanding of the concepts covered in this post.
1. Which fetal membrane directly surrounds the embryo/fetus and is filled with amniotic fluid?
Chorion
Yolk sac
Amnion
Allantois
Rationale: The amnion is the innermost fetal membrane that forms a fluid-filled sac (the amniotic sac) directly surrounding and protecting the developing embryo and fetus.
2. The primary function of amniotic fluid includes all of the following EXCEPT:
Cushioning the fetus from trauma
Providing nutrients for fetal growth
Allowing for fetal movement
Maintaining fetal body temperature
Rationale: The placenta is responsible for nutrient exchange. Amniotic fluid primarily cushions, allows movement, and helps maintain temperature.
3. The placenta is formed from tissues derived from both the mother and the fetus. Which fetal component primarily contributes to the formation of the placenta?
Amnion
Yolk sac
Trophoblast
Inner cell mass
Rationale: The trophoblast cells of the blastocyst are the primary fetal contributors, forming the chorionic villi which are the functional units of the placenta.
4. Which part of the placenta is the site of nutrient, gas, and waste exchange between mother and fetus?
Decidua basalis
Chorionic villi
Amniotic sac
Umbilical vein
Rationale: The chorionic villi are the tree-like structures where gas, nutrient, and waste products are exchanged across the placental barrier.
5. The umbilical cord typically contains how many blood vessels?
One artery, one vein
Two arteries, one vein
One artery, two veins
Two arteries, two veins
Rationale: The typical cord contains two arteries (carrying deoxygenated blood from fetus) and one vein (carrying oxygenated blood to fetus).
6. Which of the following fetal shunts bypasses the liver, directing oxygenated blood from the umbilical vein directly to the inferior vena cava?
Foramen ovale
Ductus arteriosus
Ductus venosus
Patent foramen ovale
Rationale: The ductus venosus allows oxygenated blood from the placenta to bypass the fetal liver and quickly reach the heart.
7. In fetal circulation, the highest oxygen saturation is found in the blood within the:
Umbilical arteries
Pulmonary artery
Umbilical vein
Aorta
Rationale: The umbilical vein carries highly oxygenated blood (around 80% saturation) from the placenta to the fetus.
8. The foramen ovale is a shunt that allows blood to bypass which fetal organ?
Liver
Lungs
Kidneys
Brain
Rationale: The foramen ovale is an opening between the atria that allows blood to bypass the non-functional fetal lungs.
9. What is the primary reason why fetal lungs receive only a small amount of blood flow in utero?
They are not yet fully developed.
The fetus breathes amniotic fluid.
High pulmonary vascular resistance.
The lungs are filled with meconium.
Rationale: The fluid-filled, unexpanded fetal lungs have high vascular resistance, causing blood to be shunted away from them.
10. After birth, the ductus arteriosus typically closes to become the:
Ligamentum teres
Ligamentum venosum
Ligamentum arteriosum
Medial umbilical ligaments
Rationale: After birth, the ductus arteriosus constricts and functionally closes, becoming the ligamentum arteriosum over time.
11. The fetal component of the placenta, characterized by its finger-like projections, is called the _____________.
Rationale: These structures, formed by the trophoblast, contain fetal capillaries and are the primary site of exchange between maternal and fetal blood.
12. The gelatinous substance that surrounds the blood vessels within the umbilical cord, protecting them from compression, is known as _____________.
Rationale: Wharton's jelly is a mucous connective tissue that provides structural support and protection to the delicate umbilical arteries and vein.
13. The fetal shunt that connects the pulmonary artery to the aorta, bypassing the fetal lungs, is the _____________.
Rationale: ductus arteriosus: This shunt allows most of the blood ejected from the right ventricle to bypass the pulmonary circulation and enter the systemic circulation.
14. The part of the maternal endometrium that forms the maternal portion of the placenta is the _____________.
Rationale: The decidua basalis is the portion of the maternal endometrium directly beneath the implanted embryo that forms the maternal side of the placenta.
15. The small, usually non-functional, sac that extends from the embryonic gut into the connecting stalk, contributing to early blood formation and primordial germ cell migration, is the _____________.
Rationale: allantois: In humans, the allantois is rudimentary but plays a role in early blood formation and the development of the urinary bladder. Its vessels become the umbilical arteries and veins.
Germ Disc, Gastrulation & Neurulation: Fortion of Organs
Brief Recap
We concluded our last discussion with the blastocyst successfully implanted (around Day 12 post-fertilization) into the uterine endometrium. At this point:
The blastocyst is fully embedded in the decidua (the transformed endometrial tissue).
The inner cell mass (embryoblast) is now clearly visible and undergoing significant changes, leading to the formation of the embryonic disc and associated cavities.
Formation of the Bilaminar Embryonic/Germ Disc and Associated Cavities (Week 2 Development)
This period, roughly from Day 8 to Day 14 post-fertilization, is often referred to as "the week of twos" because several structures differentiate into two layers or cavities. It's a phase of rapid differentiation of the inner cell mass.
After fertilization and cleavage, the embryo, now a blastocyst, undergoes profound organizational changes. It remodels itself from a sphere into a flattened, two-layered structure known as the Bilaminar Germ Disc. This process is crucial as it sets the stage for gastrulation, where the three primary germ layers will form.
1. From Blastocyst to Bilaminar Germ Disc
This transformation begins around Day 8 post-fertilization, as the Inner Cell Mass (ICM) differentiates.
A. Differentiation of the Inner Cell Mass:
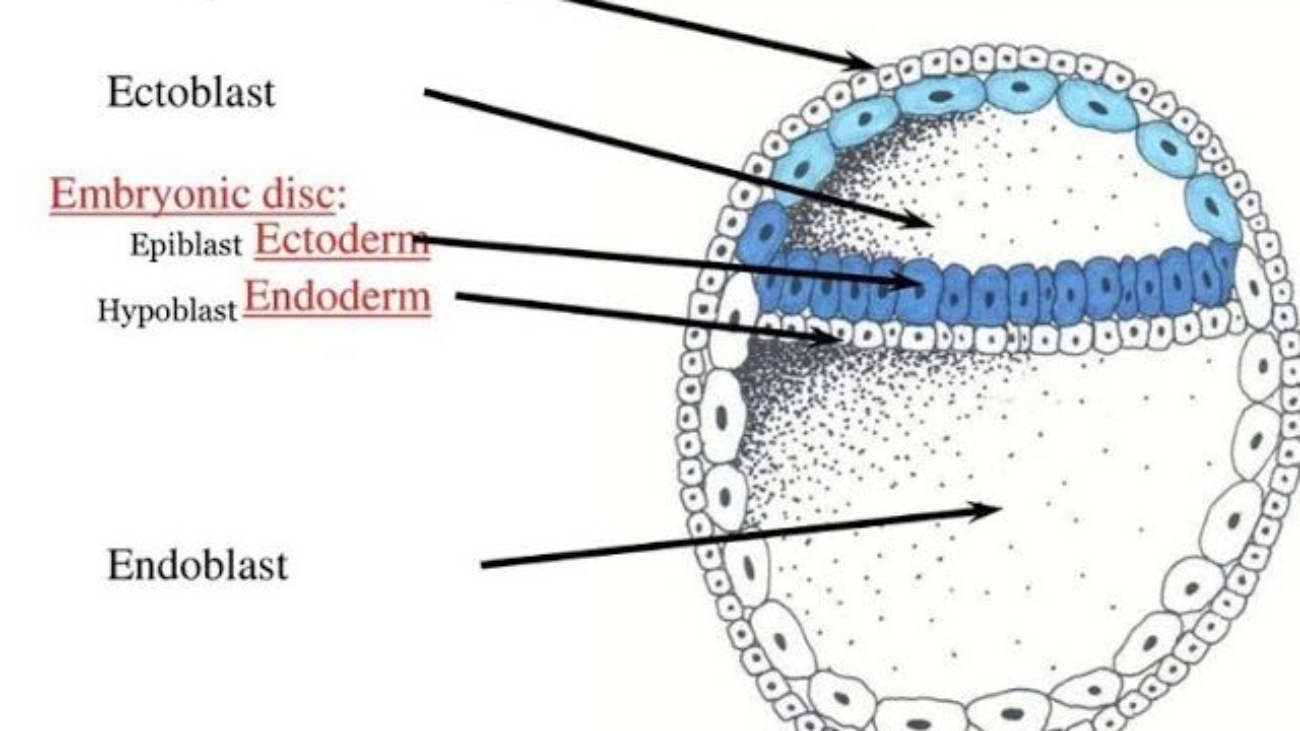
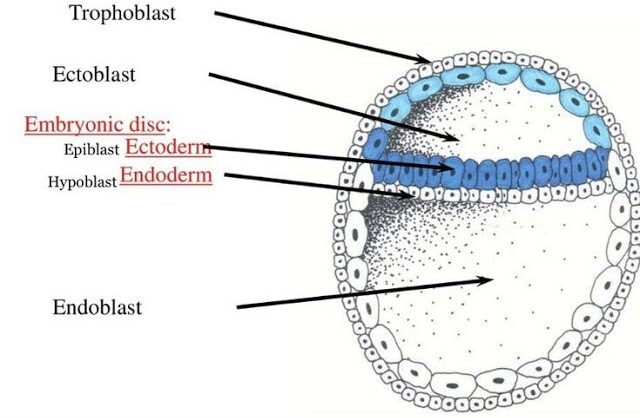
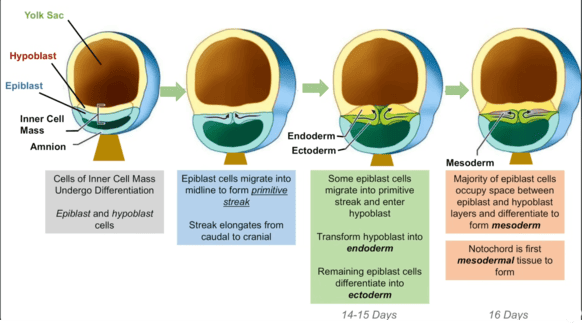
The inner cell mass (embryoblast) differentiates into two distinct layers that collectively form a flat, circular structure called the bilaminar embryonic disc:
Epiblast (Dorsal/Upper Layer)
A layer of columnar cells facing the developing amniotic cavity. Crucially, all three primary germ layers of the embryo will eventually originate from the epiblast.
Location: The dorsal (upper) layer of the disc.
Cell Type: Consists of tall, columnar cells.
Relation to Cavity: It is directly adjacent to what will become the amniotic cavity.
Significance: The epiblast is the source of all three primary germ layers during gastrulation. It is essentially the "true" embryonic component at this stage.
Hypoblast (Ventral/Lower Layer)
A layer of cuboidal cells facing the blastocoel. It primarily contributes to extraembryonic membranes, particularly the yolk sac.
Location: The ventral (lower) layer of the disc, beneath the epiblast.
Cell Type: Consists of small, cuboidal cells.
Relation to Cavity: It is directly adjacent to what will become the primary yolk sac.
Significance: While the hypoblast does not contribute directly to the embryo proper's germ layers, it plays crucial roles in signaling, guiding epiblast cell movements, and forming the extraembryonic endoderm lining of the yolk sac.
B. Formation of Associated Cavities:
As the epiblast and hypoblast differentiate, two fluid-filled cavities form in close association with them:
Amniotic Cavity
Formation: A small cavity appears within the epiblast and expands.
Lining: The roof of this cavity is formed by amnioblasts (cells that differentiate from the epiblast and line the amniotic cavity). The floor is the epiblast itself.
Contents: It will eventually be filled with amniotic fluid, which protects the developing embryo/fetus.
Primary Yolk Sac (Exocoelomic Cavity)
Formation: Cells from the hypoblast migrate and spread along the inner surface of the cytotrophoblast, forming a thin membrane called the exocoelomic membrane (Heuser's membrane). This membrane, together with the hypoblast, encloses a new cavity, the primary yolk sac.
Contents: Contains fluid and plays a role in early nutrient transfer and blood cell formation.
C. Development of Extraembryonic Structures:
During this same period (Week 2), other crucial extraembryonic structures are forming:
1. Extraembryonic Mesoderm:
Origin: A loose connective tissue layer that develops between the cytotrophoblast and the exocoelomic membrane/amnion.
Cavitation: This mesoderm soon develops large cavities, forming the extraembryonic coelom (chorionic cavity). This cavity completely surrounds the amnion and the primary yolk sac, except where the embryonic disc is connected to the trophoblast by the connecting stalk (which will become the umbilical cord).
Amniotic Cavity
A new fluid-filled space that appears within the epiblast, enclosed by a thin membrane called the amnion. It will eventually surround the entire embryo.
2. Secondary Yolk Sac:
As the extraembryonic coelom forms, the primary yolk sac shrinks, and a new, smaller secondary yolk sac forms from a second wave of hypoblast cells. This is the definitive yolk sac of the embryo.
Primary Umbilical Vesicle (Yolk Sac)
Forms when hypoblast cells line the blastocoel. In humans, it plays roles in early blood cell formation and nutrient transfer.
3. Chorion:
The extraembryonic mesoderm, together with the two layers of the trophoblast (cytotrophoblast and syncytiotrophoblast), forms the chorion.
The chorion is the outermost fetal membrane and will eventually contribute to the fetal part of the placenta. The chorionic cavity is the space within the chorion.
Extraembryonic Mesoderm & Coelom
A new layer of mesoderm forms between the yolk sac/amnion and the trophoblast. A large cavity, the chorionic cavity (or coelom), then forms within this mesoderm, suspending the embryo by a connecting stalk.
D. Establishment of Body Axes (Preliminary):
By the end of Week 2, some crucial axes begin to be established, even before gastrulation formally begins:
Dorsoventral Axis: Already defined by the epiblast (dorsal) and hypoblast (ventral).
Cranial-Caudal Axis: The future head end (cranial) is distinguished from the future tail end (caudal) by the appearance of a localized thickening of the hypoblast, the prechordal plate, at the future cranial region. This is an important signaling center.
Left-Right Asymmetry: While not yet morphologically apparent, molecular signals are starting to be laid down that will determine left-right patterning.
Summary of Bilaminar Disc Development (Week 2):
Inner cell mass differentiates into Epiblast and Hypoblast.
These form the Bilaminar Embryonic Disc.
Amniotic Cavity forms above the epiblast.
Primary Yolk Sac forms below the hypoblast, later replaced by the Secondary Yolk Sac.
Extraembryonic Mesoderm and Extraembryonic Coelom develop, surrounding the amnion and yolk sac.
The Chorion (trophoblast + extraembryonic mesoderm) encases everything.
A Connecting Stalk links the embryonic disc to the trophoblast.
Clinical Significance
This highly sensitive period is critical for assessing early embryonic viability. Disruptions during germ disc formation can lead to severe birth defects, and this is when issues like ectopic pregnancies become apparent.
4. Transition to Gastrulation
The formation of the bilaminar germ disc is the final preparatory step before gastrulation begins in week 3. During gastrulation, cells from the epiblast will migrate inward through the primitive streak to form the three definitive germ layers (ectoderm, mesoderm, and endoderm) that will give rise to the entire body.
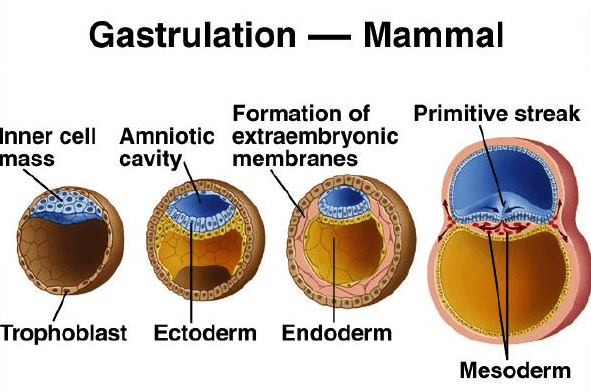
Gastrulation: Formation of Germ Layers and Body Axis
Gastrulation is a highly complex and critical developmental process that involves the dramatic reorganization and movement of embryonic cells. This process transforms the simple, two-layered bilaminar disc into a three-layered structure.
These three layers, known as the primary germ layers, are the foundational tissues from which all organs and tissues of the body will ultimately develop. In humans, gastrulation occurs around week 3 of embryonic development, after the blastocyst has successfully implanted.
Key Events of Gastrulation
Gastrulation is initiated by two fundamental events that establish the blueprint for the developing embryo.
1. Formation of the Primitive Streak
A thickened line of cells forms on the dorsal surface of the epiblast. The primitive streak is profoundly important as it establishes all major body axes: anterior-posterior (head-tail), dorsal-ventral (back-belly), and medial-lateral.
2. Cell Migration & Invagination
Epiblast cells migrate towards the primitive streak and then "dive" inward in a process called invagination. It is this inward migration and subsequent differentiation that forms the new germ layers.
Formation of the Primitive Streak
Gastrulation begins with the formation of a distinct linear structure on the surface of the epiblast, known as the primitive streak. This is the first morphological sign that the embryo is transitioning from a simple disc to a more complex, three-dimensional structure with defined axes.
A. Timing and Location:
Timing: The primitive streak appears around Day 15-16 post-fertilization.
Location: It forms on the dorsal surface of the epiblast, specifically at the caudal end of the embryonic disc.
Elongation: Once formed, it rapidly elongates in a cranial (headward) direction, reaching about half the length of the embryonic disc by Day 17-18.
B. Structure of the Primitive Streak:
As the primitive streak elongates, it develops specific anatomical features:
1. Primitive Groove
Description: A narrow, shallow depression that runs along the midline of the primitive streak.
Function: This groove is the actual passageway or "mouth" through which epiblast cells will migrate inwards, a process called ingression (or sometimes referred to as invagination, though ingression is more precise for individual cell migration).
2. Primitive Node (Hensen's Node)
Description: A distinct, slightly elevated, knob-like or pit-like structure located at the most cranial (anterior) end of the primitive streak.
Function: The primitive node is a crucial organizing center for gastrulation and subsequent development. Cells passing through the primitive node have a distinct fate, forming the notochord and prechordal plate. It's also involved in establishing left-right asymmetry.
3. Primitive Pit
Description: A small depression or pit located in the center of the primitive node. It is essentially the cranial-most opening of the primitive groove.
Function: This is the entry point for cells destined to form the notochord.
C. Significance of the Primitive Streak:
The primitive streak is far more than just a visible landmark; it is the central organizing structure of gastrulation and critical for establishing the fundamental body plan:
Defines Embryonic Axes:
Cranial-Caudal Axis: Its appearance defines the cranial (head) and caudal (tail) ends of the embryo. The primitive streak itself forms at the caudal end and extends cranially.
Medial-Lateral Axis: The streak runs along the midline, establishing the embryo's central axis.
Dorso-Ventral Axis: Already established by the epiblast/hypoblast arrangement.
Left-Right Axis: While not morphologically obvious at this stage, molecular signals originating around the primitive node begin to establish this crucial asymmetry.
Gateway for Cell Migration: It is the exclusive site for epiblast cells to ingress into the interior of the embryo to form the new germ layers. Without the primitive streak, gastrulation cannot occur.
Source of Inductive Signals: The primitive node, in particular, acts as a signaling center, producing factors that influence the differentiation of surrounding cells and contribute to processes like neural induction (later).
D. Molecular Regulation of Primitive Streak Formation:
The precise formation and maintenance of the primitive streak are orchestrated by a complex interplay of signaling molecules:
Nodal (TGF-β superfamily)
Nodal plays a central role in initiating and maintaining the primitive streak, promoting cell ingression, and influencing cell fate. It's often found in a gradient, with higher concentrations at the caudal end.
BMP4 (Bone Morphogenetic Protein 4)
Produced throughout the epiblast and primitive streak. High levels generally promote ventral mesoderm fates (e.g., blood and kidney precursors), while antagonists of BMP (like Chordin and Noggin, produced by the primitive node) allow for neural development.
FGF8 (Fibroblast Growth Factor 8)
Secreted by primitive streak cells, FGF8 is crucial for controlling cell migration through the streak and maintaining its integrity. It also works with Nodal to specify mesodermal lineages.
Wnt Signaling
Involved in establishing and maintaining the posterior (caudal) identity of the primitive streak.
Brachyury (T gene)
A transcription factor expressed in the primitive streak and notochord. It is essential for mesoderm formation and differentiation, and for the elongation of the primitive streak and notochord.
So, we now have our active, elongating primitive streak, complete with its groove, node, and pit. This structure is precisely positioned and signaling actively, preparing for the most dramatic cellular rearrangement: the actual movement of epiblast cells to form the three germ layers.
The Three Primary Germ Layers
As cells invaginate and migrate, they arrange themselves into three distinct layers, each with a specific developmental fate.
Cell Migration and Ingression: The Formation of the Three Primary Germ Layers
This is the heart of gastrulation. It involves the dynamic movement and differentiation of epiblast cells as they pass through the primitive streak.
A. The Process of Ingression:
Key Mechanisms
Epiblast as the Source: All three germ layers (ectoderm, mesoderm, and endoderm) originate exclusively from the epiblast. The hypoblast is displaced and does not contribute to the embryo proper.
Convergent Extension: Epiblast cells around the primitive streak undergo active changes. They begin to proliferate, lose their epithelial characteristics (cell-to-cell junctions), become bottle-shaped, and detach from the epiblast layer.
Movement into the Groove: These cells then migrate towards and move into the primitive groove.
Ingression vs. Invagination: This process of individual epiblast cells detaching from the surface layer and moving into the space between the epiblast and hypoblast is called ingression. It is distinct from invagination, where an entire sheet of cells folds inwards.
Cellular Transformation (EMT): As they ingress, these cells undergo an Epithelial-to-Mesenchymal Transition (EMT). They lose their apical-basal polarity, shed adhesion molecules, and gain migratory properties, becoming mesenchymal cells.
B. Formation of the Definitive Endoderm:
The first wave of epiblast cells to ingress through the primitive groove has a very specific destination and function:
Ingression: These pioneering cells migrate through the primitive groove and move ventrally (downwards).
Displacement of Hypoblast: They position themselves beneath the epiblast and effectively displace the existing hypoblast cells. The hypoblast cells are pushed out towards the periphery, where they contribute to the extraembryonic membranes of the yolk sac.
Formation of Definitive Endoderm: The newly migrated epiblast cells replace the hypoblast to form the definitive endoderm. This layer will ultimately form the lining of the gastrointestinal and respiratory tracts, and associated glands (e.g., liver, pancreas).
C. Formation of the Intraembryonic Mesoderm:
Once the definitive endoderm is established, subsequent waves of epiblast cells ingress through the primitive groove, forming the middle germ layer:
Continued Ingression: More epiblast cells migrate through the primitive groove.
Formation of Mesenchymal Layer: Instead of displacing cells, these new cells move into the space between the newly formed definitive endoderm and the remaining epiblast. They spread out laterally and cranially.
Formation of Intraembryonic Mesoderm: This intervening layer of loosely organized mesenchymal cells constitutes the intraembryonic mesoderm. This mesoderm will give rise to a vast array of tissues and organs, including muscle, bone, connective tissue, circulatory system, and urogenital system.
D. Formation of the Definitive Ectoderm:
After the endoderm and mesoderm have been formed by ingressing cells, the remaining epiblast cells that did not ingress through the primitive streak undergo a fate change:
Remaining Epiblast: The cells that stay on the dorsal surface of the embryonic disc, remaining in the epiblast layer, are now designated as the definitive ectoderm.
Future Development: This ectoderm will give rise to the epidermis (skin and its appendages), the nervous system (brain and spinal cord), and sensory organs.
Summary of Germ Layer Formation through Ingression
Epiblast Cells (the original upper layer of the bilaminar disc) are the sole source.
First Wave (through primitive groove) → displaces Hypoblast → forms Definitive Endoderm.
Second Wave (through primitive groove) → occupies space between Epiblast & Endoderm → forms Intraembryonic Mesoderm.
Remaining Epiblast → forms Definitive Ectoderm.
E. Special Mesodermal Derivatives from the Primitive Node
While the bulk of the mesoderm forms through the primitive groove, cells ingressing specifically through the primitive node and primitive pit have special fates:
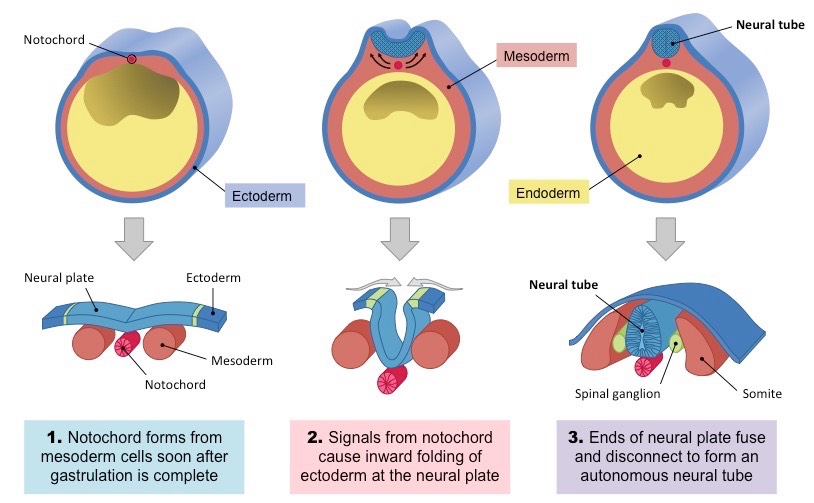
The Notochord
Origin: Cells ingressing through the primitive pit (at the very cranial end of the primitive node) migrate cranially along the midline.
Formation: They form a rod-like structure called the notochordal process. This process then elongates and hollows, forming the notochordal canal, before fusing with the endoderm and eventually detaching to form the solid notochord.
Significance: The notochord is a transient, flexible rod that:
Defines the primitive axis of the embryo.
Provides some rigidity.
Serves as the basis for the axial skeleton (vertebral column will form around it).
Is crucial for neural induction: it induces the overlying ectoderm to form the neural plate (the precursor to the brain and spinal cord).
Plays a role in determining the dorsal-ventral axis of the neural tube and somites.
Fate: In adults, the notochord remnants persist as the nucleus pulposus of the intervertebral discs.
Prechordal Plate
Origin: Some cells that ingress through the primitive node and migrate cranially, but do not become part of the notochord.
Location: They form a small, localized region of mesoderm just cranial (anterior) to the notochord.
Significance: The prechordal plate is an important signaling center for the development of the forebrain and cranial structures. It also contributes to the cranial mesoderm.
At this point, the embryo has been transformed into a trilaminar embryonic disc, with distinct ectoderm, mesoderm, and endoderm layers. The notochord is forming, defining the central axis and setting the stage for nervous system development.
Derivatives of the Three Primary Germ Layers (An Overview)
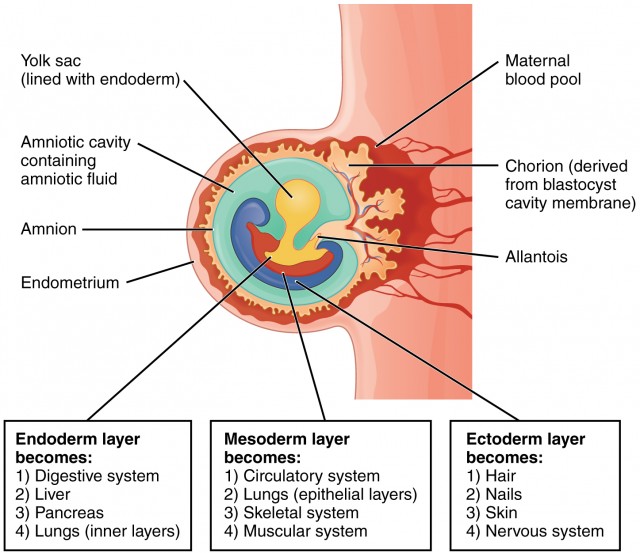
It is crucial to understand that each of these newly formed germ layers (ectoderm, mesoderm, and endoderm) is programmed to give rise to specific tissues, organs, and systems in the developing embryo. This is a high-level overview; we will delve deeper into organogenesis later.
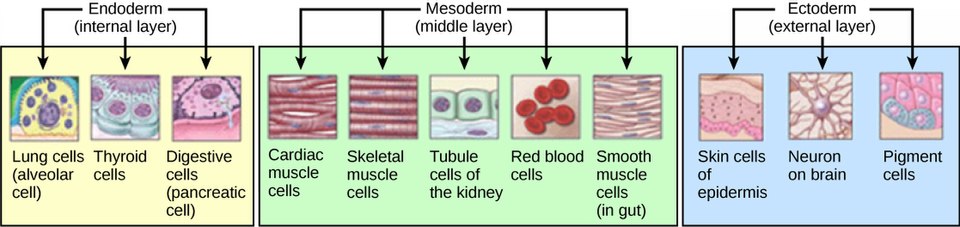
A. Ectoderm (The "Outer" Layer)
The ectoderm differentiates into two main components: surface ectoderm and neuroectoderm.
1. Surface Ectoderm
Epidermis: The outer layer of skin, including hair, nails, and sebaceous glands.
Cutaneous Glands: Sweat glands, mammary glands.
Oral Epithelium: Lining of the mouth, enamel of teeth.
Sensory Epithelium of Sense Organs: Lens of the eye, inner ear, olfactory (smell) epithelium.
Peripheral Nervous System: All neurons and glial cells outside the brain and spinal cord, including cranial nerves, spinal nerves, and autonomic ganglia.
Retina of the Eye: And optic nerve.
Posterior Pituitary Gland: (Neurohypophysis).
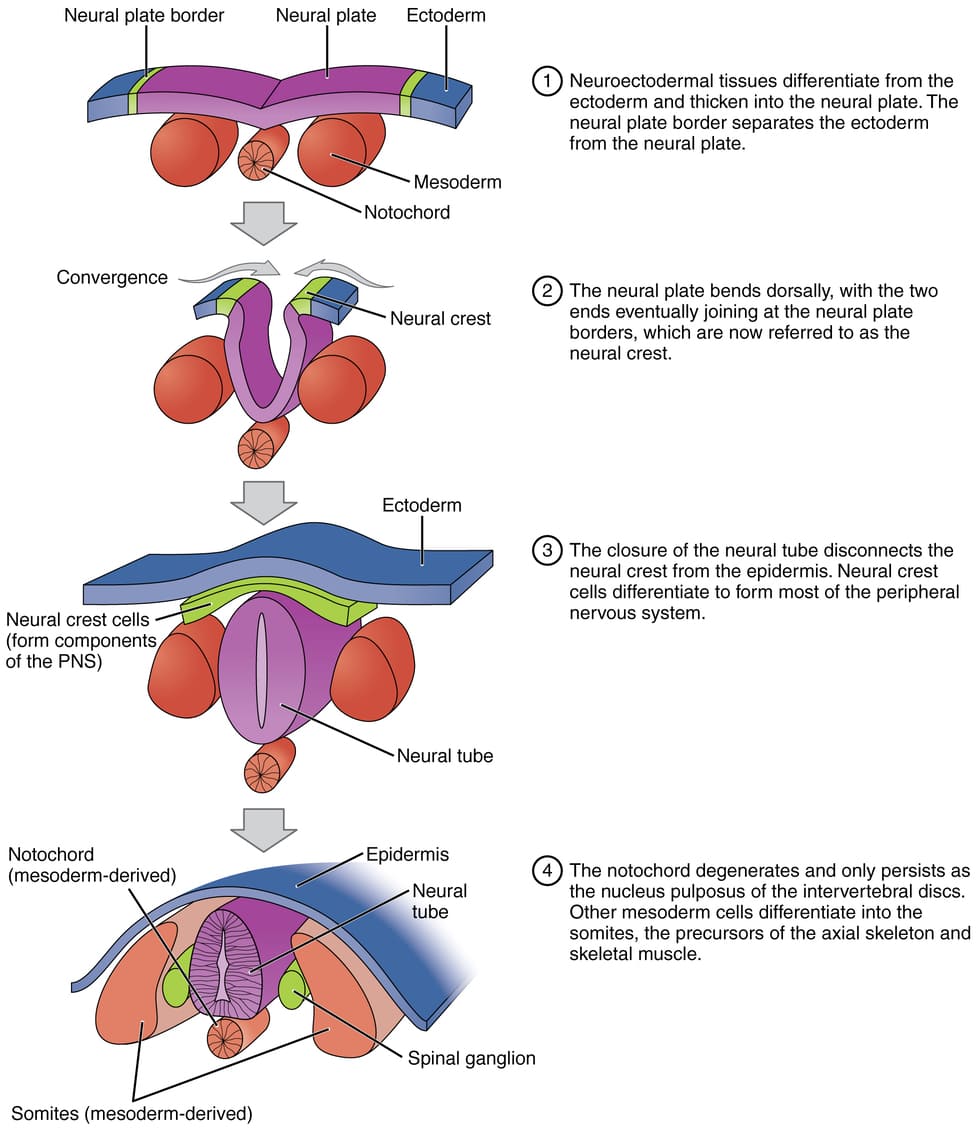
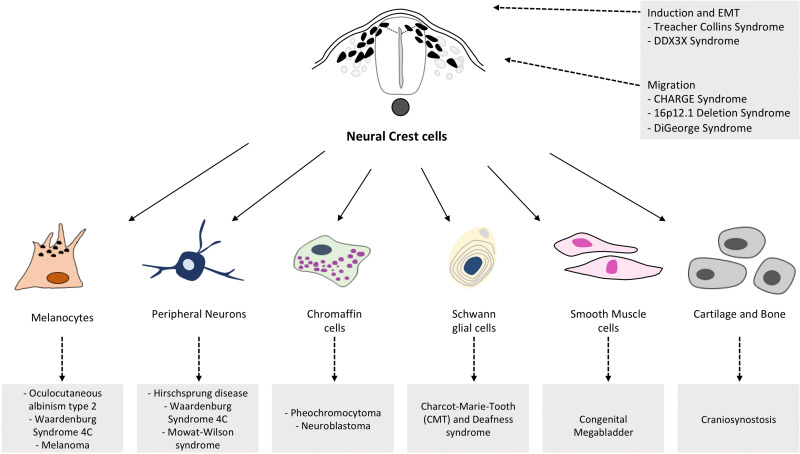
3. Neural Crest Cells
A special population of cells that delaminate from the edges of the neural plate/tube. They are often considered the "fourth germ layer" due to their widespread migratory capabilities and diverse derivatives:
Craniofacial Structures: Bones, cartilage, connective tissue of the face and skull.
Endocrine Glands: Adrenal medulla, C-cells of the thyroid.
Pigment Cells: Melanocytes (skin pigmentation).
Cardiac Development: Septa of the outflow tract of the heart.
B. Mesoderm (The "Middle" Layer)
The mesoderm is arguably the most diverse germ layer, giving rise to connective tissues, muscles, and circulatory system components. It differentiates into distinct regions:
1. Paraxial Mesoderm
Forms somites (blocks of tissue that appear sequentially along the neural tube).
Sclerotome: Vertebrae and ribs.
Myotome: Skeletal muscle of the trunk and limbs.
Dermatome: Dermis of the skin (connective tissue under epidermis).
2. Intermediate Mesoderm
Urinary System: Kidneys, ureters, bladder.
Gonads: Ovaries and testes.
Reproductive Ducts: Portions of the male and female reproductive tracts.
3. Lateral Plate Mesoderm
Divides into two layers separated by the intraembryonic coelom (future body cavities).
Somatic (Parietal) Mesoderm:
Forms the parietal layer of serous membranes (lining body walls), connective tissue of limbs, and parts of the sternum.
Splanchnic (Visceral) Mesoderm:
Forms the visceral layer of serous membranes (covering organs), smooth muscle and connective tissue of internal organs (e.g., gut wall, respiratory tract), and heart and circulatory system (blood vessels, blood cells, lymphatic vessels).
4. Head Mesoderm
Undifferentiated mesoderm in the cranial region, contributes to connective tissues and muscles of the head.
C. Endoderm (The "Inner" Layer)
The endoderm primarily forms the epithelial lining of internal organs and associated glands.
Gastrointestinal Tract: Epithelial lining from the pharynx to the rectum (excluding portions of the oral cavity and anal canal, which are ectodermal).
Respiratory Tract: Epithelial lining of the larynx, trachea, bronchi, and alveoli of the lungs.
Epithelial Lining of Urinary Bladder: And most of the urethra.
Epithelial Lining of Auditory Tube and Tympanic Cavity.
To Summarize;
Ectoderm (Outer Layer)
Formed from the remaining cells of the epiblast that do not invaginate.
Future Structures:
Nervous System (brain, spinal cord, nerves)
Epidermis of Skin (including hair and nails)
Sensory Organs (eyes, ears)
Mesoderm (Middle Layer)
Formed from the cells that invaginate and migrate to lie between the epiblast and the newly formed endoderm.
Future Structures:
Muscles, Bones, and Cartilage
Circulatory System (heart, blood, vessels)
Kidneys and Reproductive Organs
Endoderm (Inner Layer)
Formed from the first cells that invaginate and displace the original hypoblast layer.
Future Structures:
Lining of the Digestive Tract (and associated glands like the liver and pancreas)
Lining of the Respiratory System (lungs)
Lining of the Bladder
6. Other Key Structures Formed or Established During Gastrulation
Beyond the germ layers, gastrulation is crucial for defining several other foundational structures:
A. Notochord
Recap: Forms from cells ingressing through the primitive node, migrating cranially, forming the notochordal process, and eventually solidifying into the definitive notochord.
Critical Role: The notochord defines the embryonic midline, acts as a primary inducer for the overlying ectoderm to form the neural plate (the first step in central nervous system development), and patterns the surrounding mesoderm. It is crucial for proper vertebral column formation.
B. Prechordal Plate
Recap: A localized thickening of mesoderm (derived from the primitive node) just cranial to the notochord.
Critical Role: It is a vital signaling center for the development of the forebrain and craniofacial structures. It also helps organize the head mesenchyme.
C. Oropharyngeal Membrane (Buccopharyngeal Membrane)
Description: A small, circular area at the cranial end of the embryonic disc where the ectoderm and endoderm remain in direct contact, with no intervening mesoderm.
Significance: It forms the future opening of the mouth. It will eventually rupture (around Week 4) to connect the developing oral cavity with the pharynx.
D. Cloacal Membrane
Description: A similar small, circular area at the caudal end of the embryonic disc where the ectoderm and endoderm remain in direct contact, with no intervening mesoderm.
Significance: It forms the future opening of the anus and urogenital orifices. It will eventually rupture (around Week 7) to create these openings.
E. Body Axes Finalized
Gastrulation definitively establishes the cranial-caudal (head-to-tail) and medial-lateral axes.
The left-right axis also becomes established during gastrulation. This is due to molecular events around the primitive node (e.g., a "nodal flow" generated by cilia in the primitive node, influencing the asymmetrical expression of genes like Nodal and Lefty-1, which dictate left-sided development).
Clinical Note: Failure of this patterning can lead to conditions like situs inversus.
Primitive Streak Regression and Disappearance
The primitive streak, having served its essential purpose as the gateway for cell ingression and germ layer formation, is a transient structure. It does not persist throughout embryonic development.
1. Regression:
Beginning around Day 18-20, the primitive streak starts to shorten and move caudally (towards the tail end) relative to the embryonic disc.
2. Disappearance:
By the end of the fourth week (around Day 28), the primitive streak normally undergoes complete regression and disappears.
3. Significance of Regression:
Its timely regression is critical for proper embryonic development. The processes of gastrulation (formation of germ layers) and neurulation (formation of the neural tube) occur concurrently and in a cranio-caudal sequence, meaning the cranial regions differentiate while the caudal regions are still undergoing gastrulation. The primitive streak regresses as these caudal regions complete gastrulation and begin to form more mature structures.
8. Clinical Correlates: When Gastrulation Goes Awry
Given the complexity and critical timing of gastrulation, errors during this period can have severe consequences, often leading to major congenital malformations or early embryonic demise. These are some of the most significant clinical conditions associated with faulty gastrulation:
A. Sacrococcygeal Teratoma
Cause: This is the most common tumor in newborns. It results from the persistence of remnants of the primitive streak (pluripotent cells that failed to ingress or fully differentiate) in the sacrococcygeal region.
Nature: These primitive streak cells retain their pluripotency and can give rise to tissues from all three germ layers (ectoderm, mesoderm, and endoderm), resulting in a tumor that can contain hair, teeth, bone, cartilage, nervous tissue, glandular tissue, etc.
Location: Usually found at the base of the spine (sacrum and coccyx).
B. Caudal Dysgenesis (Sirenomelia)
Cause: This severe malformation is believed to result from an insufficient or premature regression of the primitive streak, or an insult that interferes with the caudal migration of mesoderm. This leads to a deficiency of caudal mesoderm.
Manifestations:
Partial or complete fusion of the lower limbs (giving a "mermaid-like" appearance, hence sirenomelia in severe cases).
Vertebral anomalies (sacrum and coccyx are often absent or poorly formed).
Association: Strongly associated with maternal diabetes.
C. Situs Inversus
Cause: While not a failure of germ layer formation, situs inversus is a condition where the normal left-right asymmetry of the organs is reversed (e.g., heart on the right, liver on the left). It can also be situs ambiguus or heterotaxy, where organs are randomly placed.
Mechanism: This condition results from defects in the molecular signaling pathways that establish left-right asymmetry during gastrulation, particularly around the primitive node (e.g., issues with nodal flow generated by cilia, or downstream gene expression like Nodal and Lefty-1).
D. Holoprosencephaly
Cause: While defects can occur later, some forms of holoprosencephaly (failure of the forebrain to divide into two hemispheres) are linked to problems in the prechordal plate and the signaling centers during early gastrulation that organize the head region.
Manifestations: Severe facial anomalies (cyclopia, proboscis), intellectual disability.
E. Anencephaly and Spina Bifida (Neural Tube Defects)
Cause: While technically occurring during neurulation (which immediately follows gastrulation), the proper formation and signaling from the notochord (derived during gastrulation) are crucial for inducing the overlying ectoderm to form the neural tube. Problems in notochord formation or signaling can predispose to these defects.
Anencephaly: Failure of the neural tube to close at the cranial end, resulting in the absence of a major portion of the brain and skull.
Spina Bifida: Failure of the neural tube to close at the caudal end, leading to various degrees of spinal cord and vertebral column defects.
9. Overall Significance of Gastrulation
To bring it all together:
Body Plan Establishment:
Gastrulation fundamentally establishes the three primary germ layers and the basic body plan of the organism, including all major body axes.
Cellular Differentiation:
It initiates the first major wave of cellular differentiation, transforming pluripotent epiblast cells into specific lineages.
Precursor to Organogenesis:
It lays the essential foundation upon which all subsequent organogenesis will occur. Without successful gastrulation, no further embryonic development is possible.
Vulnerability:
Due to its complex, coordinated cellular movements and signaling events, gastrulation is a highly sensitive period in development. Teratogens (agents causing birth defects) are particularly damaging during this window.
Organogenesis: From Germ Layers to Organs
Organogenesis is the dynamic developmental process where the three primary germ layers transform into specialized tissues and functional organs. This highly coordinated period begins around the end of week 3 and continues intensely through week 8, by which time all major organ systems have begun to form.
Timing:
Organogenesis spans from the third week (overlapping with gastrulation and neurulation, as initial organ precursors form) through to the eighth week of development.
Key Event:
During this period, the major organ systems begin to develop and take shape. By the end of the eighth week, all major organ systems are established, and the embryo looks distinctly human.
Significance:
This is an extremely critical period of development. Because so many fundamental structures are being laid down, the embryo is highly susceptible to teratogenic agents (factors causing birth defects) during this time.
General Principles of Organogenesis
Organogenesis isn't a random process; it's governed by several fundamental principles:
A. Inductive Interactions
One tissue signals to another to influence its development (e.g., notochord inducing neural plate).
Reciprocal Induction: Often, the induced tissue then signals back to the inducer, leading to a cascade of developmental events (e.g., eye development, limb development).
B. Cell Proliferation & Growth
Cells multiply rapidly through mitosis, increasing the size and complexity of tissues and organs.
C. Cell Migration
Cells move from their place of origin to their definitive location (e.g., neural crest cells, primordial germ cells, heart cells).
D. Cell Differentiation
Cells become specialized in structure and function (e.g., muscle cells, neurons, epithelial cells).
E. Apoptosis (Programmed Death)
Crucial for sculpting organs, forming lumens (hollow spaces), and removing unwanted structures (e.g., separating fingers and toes, forming the vaginal canal).
F. Patterning & Morphogenesis
Cells and tissues organize into specific shapes. Involves complex signaling (e.g., Hox genes for body axis patterning, FGFs for limb bud outgrowth).
Overview of Organ System Development (Week 3 - Week 8)
Here's a brief snapshot of what's happening with each major system during this crucial period.
The ectoderm gives rise to structures that maintain contact with the outside world.
Neurulation (Formation of the Nervous System)
The notochord (from the mesoderm) induces the overlying ectoderm to form the neural plate, which folds into the neural tube. This tube becomes the brain and spinal cord (CNS).
Neural Crest Cells break off during this process to form the peripheral nervous system, pigment cells, and parts of the face, skull, and heart.
Epidermal Ectoderm
The remaining ectoderm forms the epidermis and its derivatives, including: hair, nails, sweat glands, mammary glands, tooth enamel, and the lens of the eye.
II. Development from the Mesoderm (Middle Layer)
The mesoderm gives rise to structures that support and move the body, and circulate fluids.
Paraxial Mesoderm (forms Somites)
Sclerotome: Vertebrae and ribs (skeleton).
Myotome: Skeletal muscles.
Dermatome: Dermis of the skin.
Intermediate Mesoderm
Forms the urogenital system: kidneys, gonads (ovaries/testes), and their associated ducts.
Lateral Plate Mesoderm
Forms the body cavities, connective tissues of the body wall and limbs, smooth muscle of organs, and the entire circulatory system (heart, blood vessels, blood cells).
III. Development from the Endoderm (Inner Layer)
The endoderm primarily forms the epithelial lining of internal structures.
Gut Tube & Respiratory System
The endoderm folds to form a tube, giving rise to the epithelial lining of the entire digestive tract (pharynx to large intestine) and the respiratory system (trachea, bronchi, lungs).
Associated Glands & Organs
Forms the functional tissues of the liver, pancreas, gallbladder, thyroid, parathyroid, and thymus, as well as the lining of the urinary bladder.
The Embryonic Period Concludes (End of Week 8)
By the end of the eighth week (approx. 56 days post-fertilization), the embryonic period ends, and the fetal period begins.
All major organ systems are now established, though many are not yet fully functional.
The embryo is about 3 cm long (crown-rump length) and weighs around 4-5 grams.
It now has a distinctly human appearance, with discernible limbs, digits, and facial features.
Clinical Correlates: Teratogens During Organogenesis
Because organogenesis is the period of rapid development and differentiation of all major systems, it is also the period of greatest sensitivity to teratogens. Exposure to harmful agents during these weeks can lead to severe congenital malformations.
Examples:
Thalidomide: Caused severe limb reduction defects (amelia, phocomelia) when taken during Weeks 4-6.
Radiation: Can cause microcephaly, intellectual disability.
Understanding the timeline of organogenesis is crucial for identifying when exposure to a teratogen would have its most devastating effect on a particular organ system.
So means we start from Nervous System. Neurulation Next
What is Neurulation?
Neurulation is the process by which the neural plate folds to form the neural tube, which subsequently develops into the brain and spinal cord. It is the first step in the formation of the Central Nervous System (CNS). This process is critically important as the CNS acts as the control center for virtually all body functions.
When does it occur?
Timing: Primarily takes place during the third and fourth weeks of embryonic development.
Key Event: It directly follows and is critically dependent upon the formation of the notochord during gastrulation.
Why is it so significant?
Foundation of the CNS: It creates the precursor structure for the entire brain and spinal cord.
Inductive Event: It's a classic example of embryonic induction, where one tissue (the notochord) signals to another (the overlying ectoderm) to change its fate and develop into a new structure.
Vulnerability: Due to the complex movements and cell shape changes involved, neurulation is highly susceptible to disruptions, leading to a class of birth defects known as Neural Tube Defects (NTDs).
Neurulation is the pivotal process by which the neural plate folds and fuses to form the neural tube, the embryonic precursor to the central nervous system (CNS)—the brain and the spinal cord. This is one of the first major events of organogenesis.
This process begins during the third week of development (around day 18) and is completed by the end of the fourth week (around day 28). It occurs in the dorsal ectoderm, directly above the notochord.
Key Players and Precursors
Notochord (from Mesoderm)
The master conductor. This rod-like structure secretes signaling molecules that act as neural inducers.
Ectoderm
The outermost germ layer that responds to the notochord's signals, differentiating into the nervous system and skin.
The Role of the Notochord: The Master Inducer
Before neurulation can even begin, the newly formed notochord (from gastrulation) must be in place. The notochord is the primary inducer of neurulation.
Location: The notochord lies in the midline, directly beneath the ectoderm and above the endoderm.
Signaling: The notochord secretes various signaling molecules, most notably Sonic Hedgehog (Shh) and Noggin/Chordin (BMP antagonists).
Induction: These signals induce the overlying ectoderm to differentiate into neuroectoderm, forming the neural plate. Without the notochord, the ectoderm would continue to develop into epidermis.
Stages of Neurulation
Neurulation is divided into two main phases, with primary neurulation forming the majority of the CNS.
1. Primary Neurulation
a. Formation of the Neural Plate (Day 18)
The notochord induces the overlying ectoderm to thicken and flatten, forming an elongated structure called the neural plate. The cells of this plate are now called neuroectoderm.
Origin: The ectoderm that lies directly dorsal to the notochord.
Transformation: Under the inductive influence of the notochord, this region of the ectoderm thickens and flattens to form a slipper-shaped, elongated structure called the neural plate.
Location: Extends cranially from the primitive node towards the oropharyngeal membrane.
Cell Type: Cells are now called neuroectoderm. They are taller and more columnar than the surrounding surface ectoderm.
b. Formation of Neural Groove & Folds (Day 19-20)
The lateral edges of the neural plate elevate to form neural folds, while the central region sinks to create the neural groove. Hinge points form, causing the plate to bend inward.
Elevation: The lateral edges of the neural plate elevate, forming neural folds.
Neural Groove: As the neural folds elevate, a central depression forms between them, known as the neural groove.
U-shape: This process gives the neural plate a U-shaped appearance.
c. Fusion of Neural Folds (Day 20-22)
The neural folds move towards the midline and begin to fuse, starting in the future cervical (neck) region. This fusion proceeds in both directions, like a zipper.
Approximation & Fusion: Neural folds meet in the midline and fuse, starting in the cervical region (future neck) and proceeding cranially and caudally.
Neural Tube Formation: Seals off the neural groove, creating a hollow, tube-like structure.
Separation: The neural tube detaches from the overlying surface ectoderm, which fuses to form the continuous epidermis.
Closure Points:
Anterior (Cranial) Neuropore: Closes around Day 25.
Posterior (Caudal) Neuropore: Closes around Day 27-28.
d. Formation of the Neural Tube & Neural Crest
As the folds fuse, the neural tube is pinched off from the surface ectoderm, which then fuses above it to become the epidermis. At the crests of the fusing folds, a unique population of neural crest cells delaminates and begins to migrate.
e. Closure of Neuropores
The open ends of the neural tube, the neuropores, are the last to close. The anterior (cranial) neuropore closes around day 25, and the posterior (caudal) neuropore closes around day 28.
Differentiation of the Neural Tube: Brain and Spinal Cord Development
Once formed, the neural tube doesn't remain a simple, uniform structure. It rapidly undergoes regionalization and differentiation into the distinct parts of the central nervous system. This process begins even as the neural tube is closing.
A. Regionalization along the Cranio-Caudal Axis:
The neural tube quickly develops distinct regions along its length, largely due to signaling molecules (like FGFs, Wnt, and retinoic acid gradients) that establish anterior-posterior patterning.
1. Brain Vesicles (Cranial End)
The cranial (anterior) two-thirds of the neural tube expands dramatically and forms three primary brain vesicles by the end of Week 4:
Prosencephalon (Forebrain): Will further divide into the telencephalon (cerebral hemispheres) and diencephalon (thalamus, hypothalamus).
Mesencephalon (Midbrain): Remains a single vesicle.
Rhombencephalon (Hindbrain): Will further divide into the metencephalon (pons, cerebellum) and myelencephalon (medulla oblongata).
These vesicles will then undergo further folding and differentiation to form the complex structures of the adult brain.
2. Spinal Cord (Caudal End)
The caudal (posterior) one-third of the neural tube remains relatively narrow and develops into the spinal cord.
B. Regionalization along the Dorso-Ventral Axis:
Within the neural tube, particularly in the spinal cord and brainstem regions, specific cell types differentiate depending on their dorsal or ventral position. This is another example of inductive signaling:
Dorsal/Sensory Side (Alar Plate)
Induced by signals from the surface ectoderm (like BMPs and Wnt). Cells here will give rise to sensory neurons and interneurons.
Ventral/Motor Side (Basal Plate)
Induced by signals from the notochord and floor plate (like Sonic Hedgehog - Shh). Cells here will give rise to motor neurons and interneurons.
Sulcus Limitans: A longitudinal groove on the inner surface of the neural tube that separates the alar and basal plates.
C. Histological Differentiation:
The wall of the early neural tube consists of neuroepithelial cells. These rapidly divide and differentiate to form:
Neuroblasts: Precursors to neurons.
Glioblasts: Precursors to glial cells (astrocytes, oligodendrocytes).
Ependymal Cells: Line the central canal of the spinal cord and the ventricles of the brain.
2. Secondary Neurulation
While primary neurulation forms most of the CNS, the very caudal (tail end) part of the spinal cord is formed by a different process. This involves the condensation of mesenchyme cells in the tail bud, which then cavitate and fuse with the primary neural tube.
Folding of the Embryo
1. Introduction: From Flat Disc to 3D Body
Timing: Embryonic folding occurs primarily during the fourth week of development.
Purpose: To convert the flat, trilaminar embryonic disc into a more cylindrical, three-dimensional body form. This brings structures into their correct anatomical positions, establishes the major body cavities, and incorporates parts of the yolk sac into the embryo proper.
Key Movements: Folding occurs simultaneously in two main directions:
Cephalocaudal Folding: (Head-Tail) along the longitudinal axis.
Lateral Folding: (Transverse) along the horizontal axis.
2. Cephalocaudal (Longitudinal) Folding: The Head and Tail Folds
Driven primarily by the rapid growth of the neural tube, particularly the developing brain vesicles at the cranial end.
A. Cranial (Head) Fold
Mechanism: Brain vesicles grow rapidly and extend dorsally, then fold ventrally over the cardiac area.
Consequences:
Neural Tube: Forebrain moves cranially, then ventrally.
Oropharyngeal Membrane: Moves ventrally and caudally to future mouth region.
Cardiac Area: Pulled ventrally and caudally into definitive chest position.
Septum Transversum: Moves ventrally and caudally, ending up caudal to the heart (diaphragm precursor).
Foregut Formation: Part of yolk sac incorporated as the foregut.
B. Caudal (Tail) Fold
Mechanism: Caudal end of neural tube and somites grow; primitive streak regresses.
Consequences:
Neural Tube: Caudal end moves dorsally, then ventrally.
Cloacal Membrane: Carried ventrally and cranially to anal/urogenital region.
Connecting Stalk: Moves from caudal to ventral position (future umbilical cord).
Hindgut Formation: Part of yolk sac incorporated as the hindgut.
3. Lateral (Transverse) Folding: Formation of the Body Walls
Driven by the rapid growth of somites and the neural tube.
Mechanism: The left and right lateral edges of the trilaminar disc fold downwards and inwards towards the midline.
Consequences:
Body Wall Formation: Lateral plate mesoderm and ectoderm form ventrolateral body walls.
Midgut Formation: Central portion of yolk sac incorporated as midgut. Connects to yolk sac via vitelline duct.
Gut Tube Formation: Foregut, midgut, and hindgut form primitive gut tube suspended in coelom.
Formation of Body Cavities: Intraembryonic coelom transforms into pericardial, pleural, and peritoneal cavities.
Fusion of Ventral Body Wall: Lateral folds meet and fuse in midline (except at umbilical cord).
The neural tube, the primary structure formed during neurulation, differentiates into the entire Central Nervous System (CNS).
Brain
The anterior (cranial) part of the tube undergoes significant expansions to form the primary brain vesicles, which further differentiate into all adult brain structures (cerebrum, cerebellum, brainstem, etc.).
Spinal Cord
The posterior (caudal) part of the neural tube forms the spinal cord.
Neural Canal
The hollow lumen inside the tube becomes the ventricular system of the brain and the central canal of the spinal cord, responsible for circulating cerebrospinal fluid (CSF).
Formation of the Neural Crest Cells: The "Fourth Germ Layer"
During the process of neural fold elevation and fusion, a very special population of cells emerges.
Origin: As the neural folds elevate and fuse, cells at the crest (apex) of the neural folds undergo an epithelial-to-mesenchymal transition (EMT) and delaminate.
Migration: These cells, now called neural crest cells, migrate extensively throughout the embryo.
Craniofacial Structures: Bones, cartilage, connective tissue of the face and skull.
Endocrine Glands: Adrenal medulla, C-cells of the thyroid.
Pigment Cells: Melanocytes (skin pigmentation).
Cardiac Structures: Septa of the outflow tract of the heart.
Other: Dermis of facial region, smooth muscle of large arteries, odontoblasts (dentin of teeth).
By the end of primary neurulation, we have a fully formed neural tube, destined to become the brain and spinal cord, and a migrating population of neural crest cells that will contribute to many other body systems.
Derivatives of the Neural Crest Cells
Neural crest cells are often called the "fourth germ layer" due to their remarkable migratory abilities and the vast array of diverse tissues they form. After delaminating from the neural folds, they travel extensively throughout the embryo.
Peripheral Nervous System (PNS)
Sensory & Autonomic Neurons
Schwann Cells
Endocrine & Pigment
Adrenal Medulla
Melanocytes (pigment cells)
Craniofacial Structures
Bones & cartilage of face/skull
Dentin of teeth
Cardiac Development
Outflow tract of the heart
Clinical Correlates: Neural Tube Defects (NTDs)
Neural Tube Defects (NTDs) are among the most common and serious birth defects. They result from the failure of the neural tube to close properly at specific points along its length.
A. Factors Contributing to NTDs:
Folic Acid Deficiency: This is by far the most well-established and preventable cause. Adequate maternal folic acid intake (especially preconception and during the first trimester) is crucial.
Genetics: Some genetic predispositions exist.
Maternal Diabetes: Poorly controlled maternal diabetes increases the risk.
Certain Medications: Some anticonvulsants (e.g., valproic acid) increase risk.
Maternal Obesity.
Hyperthermia: Exposure to high temperatures during early pregnancy.
B. Types of NTDs:
1. Anencephaly
Cause: Failure of the anterior (cranial) neuropore to close (around Day 25).
Manifestations: Absence of a major portion of the brain, skull, and scalp. The brain tissue that is present is often malformed and exposed.
Prognosis: Incompatible with life; affected fetuses are stillborn or die shortly after birth.
2. Spina Bifida
Cause: Failure of the posterior (caudal) neuropore to close (around Day 27-28), or more generally, defective closure of the vertebral arches of the spinal column.
a) Spina Bifida Occulta (Hidden)
Mildest form. Incomplete fusion of vertebral arches, usually asymptomatic. Identified by hair patch/dimple.
b) Meningocele
Meninges protrude through the defect forming a fluid-filled sac. Spinal cord remains in canal. Fewer neurological deficits.
c) Myelomeningocele (Severe)
Meninges AND spinal cord protrude. Significant deficits: paralysis, loss of sensation, hydrocephalus (Chiari II), bowel/bladder dysfunction.
3. Encephalocele (Cranium Bifidum)
Cause: Defect in closure of neural tube AND skull, resulting in protrusion of brain tissue/meninges.
Manifestations: Varying degrees of neurological impairment.
C. Prevention of NTDs:
Folic Acid Supplementation: The most effective preventative measure. Women of childbearing age are recommended to take 400 micrograms (0.4 mg) daily, starting at least one month before conception. Higher doses (e.g., 4 mg) for high-risk cases.
Fertilization & Implantation: The Beginning of a New Individual
Fertilization
Fertilization, also known as conception, is the fundamental biological process where a male gamete (sperm) and a female gamete (secondary oocyte) fuse to form a new, single-celled entity called a zygote.
Fertilization is the process by which a male gamete (sperm) and a female gamete (ovum) fuse to form a new diploid cell called a zygote. This event typically occurs in the ampulla of the fallopian tube, usually within 12-24 hours after ovulation.
This remarkable union restores the diploid (2n) number of chromosomes and marks the very beginning of the development of a new, genetically unique individual.
Site of Fertilization
In humans, fertilization typically occurs in the ampulla of the fallopian tube (oviduct). This is the wider, outer portion of the tube, close to the ovary, where the egg is captured after ovulation.
The Key Players in Fertilization
Successful fertilization depends on the precise interaction of four critical components.
Sperm (Male Gamete)
A small, motile cell designed to travel through the female reproductive tract and deliver its haploid genetic material to the egg.
Egg (Secondary Oocyte)
A large, non-motile cell containing the female's haploid genetic material, cytoplasm, and all the necessary nutrients to support early embryonic development. It is arrested in Metaphase II of meiosis.
Zona Pellucida
A thick, glycoprotein-rich outer layer surrounding the egg. It acts as a species-specific binding site for sperm and is essential for preventing polyspermy (fertilization by more than one sperm).
Corona Radiata
The outermost layer of follicular (granulosa) cells that surrounds the zona pellucida, providing nourishment and protection to the ovulated egg.
The Journey of the Sperm
The passage of sperm through the female reproductive tract is a highly regulated and selective process, designed to ensure only sperm with normal morphology and vigorous motility reach the egg.
Post-Ejaculation: Semen coagulates into a gel, protecting sperm from the vagina's acidic environment and holding them near the cervix. This gel liquefies within an hour.
The Cervix: Cervical mucus acts as a barrier, filtering out sub-motile sperm.
The Uterus: Uterine myometrial contractions, aided by prostaglandins in the seminal fluid, propel the sperm towards the fallopian tubes.
The first sperm enter the fallopian tubes minutes after ejaculation, but they can survive in the female reproductive tract for up to five days, awaiting ovulation.
The Events of Fertilization
Once an ovulated egg is present, fertilization proceeds through a highly coordinated series of events.
Event 1: Capacitation
A final maturation step that "arms" the sperm within the female reproductive tract.
The Process: The female tract's environment strips away cholesterol and proteins from the sperm's head.
The Result: The sperm's tail becomes hyper-motile, and its acrosome membrane is destabilized, ready to release enzymes.
Key takeaway: A sperm cannot fertilize an egg until it has been capacitated.
A. Sperm Transport and Capacitation
1. The Journey
Ejaculation & Vaginal Transit: Millions of sperm deposited in posterior fornix. Many lost to acidity/leukocytes.
Cervical & Uterine Passage: Sperm navigate the cervix (mucus becomes permeable) and uterine cavity.
Fallopian Tube: Only a few thousand reach the tubes, guided by chemotaxis and uterine contractions.
2. Capacitation (Maturation)
Crucial process (2-10 hours) in female tract involving:
Membrane Changes: Removal of cholesterol/glycoproteins from sperm head (acrosomal region). Increases fluidity/reactivity.
Hyperactivation: Increased flagellar beating (vigorous/erratic) essential for penetrating egg layers.
Result: Sperm is now capable of the acrosomal reaction.
Event 2: The Acrosomal Reaction
Penetrating the Corona Radiata: Hyper-motile sperm push through the outer layer of follicular cells.
Binding to the Zona Pellucida: The sperm binds to species-specific ZP3 receptors on the zona pellucida, like a key in a lock.
Releasing Enzymes: This binding triggers the acrosome to release digestive enzymes (like acrosin).
Digesting a Path: These enzymes create a tunnel through the zona pellucida, allowing the sperm to reach the egg's cell membrane.
B. Penetration of the Egg's Protective Layers
Upon reaching the secondary oocyte, capacitated sperm must penetrate two barriers:
1. Corona Radiata Penetration
Sperm use hyperactivated motility to push through. Enzymes like hyaluronidase (on sperm surface) break down hyaluronic acid in the extracellular matrix.
2. Zona Pellucida Penetration
Binding: Sperm proteins bind to specific receptors (primarily ZP3 glycoprotein) on the Zona Pellucida. (Species-specific).
Acrosomal Reaction: Binding to ZP3 triggers fusion of acrosomal membrane with sperm plasma membrane. Releases hydrolytic enzymes (acrosin, neuraminidase).
Sperm head lies flat against oocyte plasma membrane.
Membranes fuse.
Sperm head, tail, mitochondria, and centriole enter oocyte cytoplasm.
Events 3 & 4: The Blocks to Polyspermy
To prevent a lethal condition where more than one sperm fertilizes the egg, the oocyte deploys a two-stage defense system.
Fast Block (Immediate but Temporary)
The instant fusion of the first sperm triggers a rapid influx of sodium ions (Na⁺) into the oocyte, instantly changing the membrane's electrical charge to repel all other sperm.
Slow Block (Cortical Reaction - Permanent)
Sperm fusion also triggers a massive release of calcium ions (Ca²⁺) inside the oocyte. This causes cortical granules to release enzymes that destroy all ZP3 receptors and harden the zona pellucida, making it impenetrable.
D. Prevention of Polyspermy (Block to Polyspermy)
Mechanisms to ensure only ONE sperm fertilizes the egg (preventing lethal abnormal chromosome numbers).
1. Fast Block (Electrical)
Rapid, transient depolarization of oocyte membrane prevents other sperm fusion. (Less prominent in humans).
Oocyte Completes Meiosis: The calcium wave also signals the secondary oocyte to complete Meiosis II, forming the mature ovum and a second polar body.
Fusion of Pronuclei (Syngamy): The male pronucleus (from the sperm) and the female pronucleus (from the ovum) swell and then fuse their genetic material.
The Result: A zygote is formed—a new, single cell with the restored diploid number of 46 chromosomes, containing genetic material from both parents.
Summary
The formation of the zygote is the remarkable start of a new individual. This single cell holds all the genetic instructions for development. From this point, the journey of rapid cell division and differentiation begins, as the zygote makes its way towards the uterus.
Cleavage, Morula, and Blastocyst Formation
Immediately following fertilization, the zygote undergoes a series of rapid mitotic divisions known as cleavage, without significant growth of the embryo as a whole. This process transforms the single-celled zygote into a multicellular structure while it simultaneously travels down the fallopian tube towards the uterus.
Cleavage is the initial series of rapid mitotic cell divisions that a newly formed zygote undergoes immediately after fertilization. This process transforms the single-celled zygote into a multicellular structure ready for implantation.
Key Characteristics of Cleavage
Rapid Mitotic Divisions: The number of cells (blastomeres) increases exponentially (1, 2, 4, 8, etc.).
No Overall Growth: The embryo's total size does not increase; cells become progressively smaller with each division.
Cytoplasm Partitioning: The large volume of the zygote's cytoplasm is divided among the numerous smaller blastomeres.
A. Cleavage (Day 1-4 Post-Fertilization)
Definition & Characteristics
Rapid Mitosis: A series of divisions where cells (called blastomeres) become progressively smaller.
No Growth: These divisions occur without an increase in the overall size of the embryonic mass.
Timing/Location: Begins approx. 24 hours post-fertilization in the fallopian tube.
Purpose: To increase cell number exponentially for differentiation and prepare for blastocyst formation.
Stages of Cleavage
Day 12-Cell Stage:
Approx. 24 hours post-fertilization. First mitotic division completes.
Day 24-Cell Stage:
Divisions continue.
Day 38-Cell Stage & Compaction:
Blastomeres maximize contact forming a compact ball.
Compaction: Mediated by cell adhesion molecules. Essential for segregating inner vs. outer cell populations.
A Timeline
Zygote (Single Cell): The starting point, immediately after fertilization.
2-Cell Stage (~24 hours): First mitotic division is complete.
4-Cell Stage (~48 hours): Second division.
Morula (~3-4 days): A solid ball of 16-32 blastomeres, still enclosed within the zona pellucida.
B. Morula Formation (Day 4 Post-Fertilization)
As the morula continues to divide, a fluid-filled cavity (the blastocoel) forms inside, transforming the solid ball into a more complex structure called the blastocyst. The cells reorganize into two distinct, crucial groups: Inner cell mass(Embryoblast) and Trophoblast
16+
The Morula ("Mulberry")
Structure: A solid ball of 16-32 tightly packed, indistinguishable blastomeres.
Location: Within fallopian tube or entering uterine cavity.
Potency: Cells are Totipotent (each cell has potential to develop into a complete organism).
C. Blastocyst Formation (Day 5-6 Post-Fertilization)
As uterine fluid penetrates the zona pellucida, it accumulates within the morula, forming a central cavity called the blastocoel. This transforms the morula into a blastocyst.
Differentiation within the Blastocyst
The cells are no longer totipotent but have differentiated into two populations:
Inner Cell Mass (ICM) / Embryoblast
Cluster of cells located eccentrically at one pole.
Pluripotent: Can give rise to the embryo proper (fetus) and some extraembryonic membranes (yolk sac, amnion).
Source of embryonic stem cells.
Trophoblast
Thin, outer layer of flattened cells forming the wall.
Crucial for implantation and formation of the placenta (chorion).
Does NOT contribute to the embryo proper.
Around day 5-6, the blastocyst "hatches" from the zona pellucida, ready for implantation.
Hatching (Day 5-6)
Before implantation, the blastocyst must "hatch" from the zona pellucida. Enzymes released by the trophoblast, along with blastocyst contractions, break the zona pellucida. This is essential because the zona pellucida would otherwise prevent the trophoblast from contacting the uterine endometrium.
Formation of the Bilaminar Disc
Just as implantation begins, the Inner Cell Mass (ICM) differentiates into two critical layers, forming the bilaminar (two-layered) embryonic disc.
Epiblast (Upper Layer)
Faces the trophoblast. Crucially, all three primary germ layers (ectoderm, mesoderm, endoderm) arise from the epiblast. The entire fetus develops from this layer.
Hypoblast (Lower Layer)
Faces the blastocoel. Contributes to extraembryonic structures, primarily the yolk sac, and provides important signaling to the epiblast.
Purpose of Cleavage
Increase Cell Number: To generate enough cells for future development.
Prepare for Implantation: To form the trophoblast, which is essential for implanting in the uterus.
Establish Basic Organization: To create the initial distinction between cells that will form the embryo (ICM) and cells that will form the placenta (trophoblast).
Summary
This journey from a single zygote to a free-floating blastocyst within the uterine cavity is a remarkable feat of rapid cell division and initial differentiation. The stage is now set for the next critical event: the physical attachment of the blastocyst to the uterine wall.
Implantation
Implantation is the process by which the hatched blastocyst adheres to and subsequently invades the uterine endometrium, embedding itself within the maternal tissue. This event is absolutely essential for the successful establishment of pregnancy and typically occurs around Day 6-12 post-fertilization.
The uterine endometrium, under the influence of progesterone, must be in a receptive state ("window of implantation"), usually lasting from day 20 to 24 of a typical cycle.
Implantation is the crucial process by which the early embryo, now at the blastocyst stage, attaches itself to and invades the inner lining of the uterus, the endometrium. This typically occurs around 6 to 12 days after fertilization.
Prerequisites for Successful Implantation
For implantation to occur, two main conditions must be perfectly met, creating a synchronized "dialogue" between the embryo and the uterus.
1. A Competent Blastocyst
The blastocyst must be well-developed and, most importantly, must have "hatched" from its protective zona pellucida. This hatching allows the trophoblast cells to make direct contact with the uterine lining.
2. A Receptive Endometrium
The uterine lining must be in its secretory phase, made thick and nutrient-rich by the hormone progesterone. This period of optimal readiness is known as the "implantation window."
The Three Stages of Implantation
1. Apposition (Initial Contact / Orientation)
What it is: This is the very first, often loose, physical contact between the hatched blastocyst and the endometrial surface. It is essentially about the blastocyst "finding its spot."
Location: Most commonly, the blastocyst positions itself with its embryonic pole (the end containing the Inner Cell Mass, or ICM) facing the endometrial epithelium. This orientation is crucial for directed invasion and proper development.
Cellular Mechanisms of Apposition
Endometrial Receptivity:
The uterine endometrium must be in a specific "receptive window" (usually days 20-24 of a 28-day menstrual cycle) for implantation to succeed. This receptivity is hormonally controlled, primarily by progesterone.
Pinopodes:
During this receptive phase, the endometrial epithelial cells develop transient, finger-like protrusions called pinopodes. These structures are thought to facilitate fluid absorption, bringing the blastocyst closer to the epithelial surface, and may also be involved in cellular recognition and adhesion.
Glycocalyx Interactions:
Initial, weak interactions occur between the specialized carbohydrate-rich coat (glycocalyx) of the trophoblast cells and the glycocalyx of the endometrial epithelial cells.
Electrostatic Forces:
Subtle electrostatic forces may also play a role in this initial loose contact.
2. Adhesion (Firm Attachment)
What it is: Following apposition, the blastocyst establishes a more stable and firm attachment to the endometrial epithelial cells. This is no longer just a loose contact; it is a commitment to bind.
Cellular Mechanisms: This stage is characterized by a sophisticated molecular dialogue between the trophoblast and the endometrium, involving various adhesion molecules.
Integrins
These are transmembrane receptors found on both trophoblast and endometrial cells. They act as bridges, binding to extracellular matrix components (like fibronectin, laminin, collagen) and linking them to the cell's cytoskeleton.
Specific Pairs:αvβ3 and α4β1 are upregulated on the endometrial surface during the receptive window.
Selectins
Carbohydrate-binding proteins involved in initial transient adhesion. L-selectin on the trophoblast is thought to bind to carbohydrate ligands on the endometrial surface, facilitating initial rolling and weak attachment.
Cadherins
Calcium-dependent cell adhesion molecules important for cell-to-cell binding. E-cadherin, for instance, is expressed in the endometrium and may play a role in trophoblast-endometrial interactions.
Growth Factors & Cytokines
Local factors secreted by the endometrium modulate adhesion molecule expression.
Key Player:LIF (Leukocyte Inhibitory Factor) is particularly highlighted as crucial for enhancing endometrial receptivity and trophoblast adhesiveness.
3. Invasion (Penetration into the Endometrium)
What it is: This is the most active and transformative stage, where the blastocyst breaks down the endometrial lining and burrows deep into the uterine stroma. This process is highly regulated to prevent excessive invasion.
A. Trophoblast Differentiation
Upon contact with the endometrium, the trophoblast cells at the embryonic pole undergo rapid proliferation and differentiation into two distinct layers:
Cytotrophoblast (CTB)
The Inner Layer
This is the inner layer of mononucleated, mitotically active cells. These are the progenitor cells that continuously divide and fuse to form the outer layer. They form a distinct cellular layer.
Syncytiotrophoblast (STB)
The Outer, Invasive Layer
This is the outer layer, a highly invasive, multinucleated mass of cytoplasm formed by the fusion of underlying cytotrophoblast cells. Crucially, the STB has no distinct cell boundaries.
B. Mechanisms of Invasion
1. Proteolytic Enzyme Secretion
The syncytiotrophoblast is the primary invasive component. It secretes a battery of proteolytic enzymes:
Matrix Metalloproteinases (MMPs): These enzymes (e.g., MMP-2, MMP-9) degrade the components of the extracellular matrix (ECM) of the endometrium, such as collagen, laminin, and fibronectin. This breakdown allows the blastocyst to literally digest its way into the uterine wall.
Serine Proteinases: Other proteinases also contribute to the degradation of the ECM.
2. Phagocytosis
The syncytiotrophoblast actively engulfs and phagocytoses apoptotic endometrial cells and cellular debris, clearing a path for the invading embryo.
3. Angiogenic Factors & hCG
Angiogenesis: The invading trophoblast secretes factors that promote the growth of new blood vessels within the endometrium, essential for establishing the uteroplacental circulation.
hCG Secretion: The STB produces human chorionic gonadotropin (hCG) almost immediately. This maintains the corpus luteum → progesterone → prevents menstruation.
Closing Plug Formation: As the blastocyst burrows deeper, the endometrial epithelial defect (the entry point) is eventually closed by a coagulation plug of fibrin and cellular debris, sealing off the implantation site.
Summary of Invasion Progress
Day 8-9
The blastocyst is usually superficially embedded. The syncytiotrophoblast expands rapidly, eroding endometrial stromal cells and uterine glands. These eroded maternal tissues provide initial nutritional support (histiotrophic nutrition).
Day 9-10
Lacunae (small spaces) begin to appear within the expanding syncytiotrophoblast. These coalesce and fill with maternal blood from eroded capillaries and glandular secretions, marking the very beginning of the uteroplacental circulation.
D. Hormonal Support of Implantation
Progesterone
Critical for preparing endometrium (secretory phase) and maintaining pregnancy. Initially secreted by Corpus Luteum.
Human Chorionic Gonadotropin (hCG)
Produced by Syncytiotrophoblast as soon as implantation begins.
Structurally similar to LH.
Function: "Rescues" the Corpus Luteum, maintaining Progesterone production (preventing menstruation).
Clinical: Detected by home pregnancy tests.
Summary
With successful implantation, the embryo is securely anchored within the maternal uterus, establishing a direct connection for nutrient exchange and hormonal support. This marks the end of the pre-embryonic period and the beginning of embryonic development.
Initial Placenta Formation
As we discussed with invasion, the blastocyst's engagement with the endometrium immediately kickstarts the development of the earliest placental structures. The placenta is a vital organ that facilitates nutrient, gas, and waste exchange between the mother and the developing embryo/fetus, and it also produces crucial hormones.
The foundation of the placenta is laid during the implantation process, primarily through the differentiation and expansion of the trophoblast.
Recall from Implantation (Day 6/7 onwards):
The trophoblast layer of the blastocyst, upon contact with the endometrium, differentiates into two key layers:
Cytotrophoblast (CTB): The inner, cellular layer.
Syncytiotrophoblast (STB): The outer, invasive, multinucleated layer.
A. Development and Roles of the Cytotrophoblast and Syncytiotrophoblast in Placental Formation
1. Syncytiotrophoblast (STB): The Invasive Frontier & Exchange Mediator
Formation: Formed by the continuous fusion of underlying cytotrophoblast cells. This process is ongoing throughout placental development, especially in the early stages.
Key Characteristics:
Multinucleated: Contains numerous nuclei within a single, continuous cytoplasm. This means there are no individual cell membranes separating nuclei.
Non-mitotic: Once a cytotrophoblast cell fuses to become part of the syncytiotrophoblast, it loses its ability to divide. The STB grows by accreting new CTB cells.
Highly Invasive: As detailed previously, the STB is the primary agent of invasion during implantation. It secretes proteolytic enzymes (MMPs) to break down the endometrial extracellular matrix, allowing the blastocyst to embed.
Roles in Placenta Formation & Function:
Initial Uteroplacental Circulation (Day 9-10)
As the STB invades, it erodes the walls of maternal spiral arteries and venous sinusoids within the endometrium.
Lacunae Formation: Small, fluid-filled spaces (lacunae) develop within the expanding STB mass.
Lacunar Network: These lacunae rapidly coalesce to form an interconnected network.
Maternal Blood Inflow: As maternal capillaries are eroded, blood flows into these lacunar spaces, directly bathing the syncytiotrophoblast. This marks the establishment of the rudimentary uteroplacental circulation. This is the first critical step in enabling maternal-fetal exchange.
Nutrient Uptake & Waste Removal
The STB is the direct interface with maternal blood. It is responsible for:
Active Transport: Facilitating the uptake of nutrients (glucose, amino acids, vitamins) from maternal blood and transporting them to the embryo.
Passive Diffusion: Allowing for the diffusion of gases (oxygen to embryo, carbon dioxide from embryo) and other small molecules.
Waste Product Transfer: Facilitating the transfer of embryonic waste products (e.g., urea) into maternal circulation for excretion.
Hormone Production
The STB is a major endocrine organ of pregnancy. It synthesizes and secretes critical hormones:
1. Human Chorionic Gonadotropin (hCG):
Crucial for maintaining the corpus luteum and progesterone production in early pregnancy. This prevents menstruation.
2. Progesterone:
Takes over from the corpus luteum around 7-10 weeks of gestation as the primary source of progesterone, which is essential for maintaining uterine quiescence and pregnancy.
3. Estrogens:
Produced by the placenta in increasing amounts throughout pregnancy, contributing to uterine growth and mammary gland development.
4. Human Placental Lactogen (hPL):
Involved in maternal metabolism and fetal growth.
Immunomodulation: The STB plays a role in protecting the semi-allogeneic embryo from maternal immune rejection.
2. Cytotrophoblast (CTB): The Progenitor Layer & Structural Contributor
Formation: Derived from the trophoblast cells of the blastocyst.
Key Characteristics:
Mononucleated: Composed of individual cells, each with a single nucleus.
Mitotically Active: These cells continuously divide, providing a fresh supply of cells.
Inner Layer: Forms a distinct cellular layer internal to the syncytiotrophoblast.
Roles in Placenta Formation & Function:
1. Source of Syncytiotrophoblast
The primary role of the CTB is to serve as the progenitor cell population for the syncytiotrophoblast. CTB cells proliferate and then differentiate by fusing with the existing STB layer. This continuous renewal is vital for the growth and function of the STB.
2. Formation of Primary Chorionic Villi (Day 11-12)
As the lacunar network within the STB expands and fills with maternal blood, the cytotrophoblast cells begin to proliferate and form finger-like projections.
These solid cords of cytotrophoblast cells grow into the blood-filled lacunae, forming the primary chorionic villi. These villi are essentially columns of cytotrophoblast cells surrounded by syncytiotrophoblast.
The formation of these villi significantly increases the surface area for exchange between maternal blood and embryonic tissues, laying the groundwork for a more efficient placenta.
3. Anchoring to Decidua
In later development, some cytotrophoblast cells differentiate and invade the maternal decidua (the modified endometrium) to form extravillous cytotrophoblast (EVCT). These cells remodel maternal spiral arteries, ensuring adequate blood supply to the intervillous space and anchoring the placenta to the uterine wall. (While this happens a bit later, the CTB is the origin of these crucial cells).
Summary of Initial Placental Events (Day 9-12)
Day 9-10
Lacunae within the syncytiotrophoblast begin to form and coalesce, establishing the rudimentary uteroplacental circulation as maternal blood enters these spaces. The syncytiotrophoblast is actively absorbing nutrients and secreting hCG.
Day 11-12
Cytotrophoblast cells begin to proliferate and extend into the blood-filled syncytial lacunae, forming the primary chorionic villi. These villi represent the earliest structural units of the placental exchange interface.
The interplay between the cytotrophoblast (proliferating and forming the structural backbone) and the syncytiotrophoblast (invading, facilitating exchange, and secreting hormones) is fundamental to the successful establishment of the placenta. This early phase is characterized by rapid growth and integration into the maternal uterine wall, setting the stage for the more complex villous tree development.
The menstrual cycle is a monthly series of natural changes in hormone production and the structures of the uterus and ovaries. It is a complex, coordinated process that prepares the female body for the possibility of pregnancy.
Averaging around 28 days, the cycle is designed to produce and release an egg (ovulation) and prepare the uterus for potential implantation. If pregnancy does not occur, the uterine lining is shed, resulting in menstruation.
Key Organs & Hormones Involved
The entire cycle is a masterful conversation between the brain and the reproductive organs, regulated by a precise cascade of hormones.
Hypothalamus
Releases GnRH to start the cascade.
Pituitary Gland
Releases FSH & LH to stimulate the ovaries.
Ovaries
Mature eggs; produce Estrogen & Progesterone.
Uterus
Its lining (endometrium) thickens and sheds.
Hypothalamus releases GnRH
Pituitary Gland releases FSH & LH
Ovaries produce Estrogen & Progesterone
Uterus responds, and hormones feedback to the brain
The Purpose of the Cycle
The menstrual cycle is elegantly designed to ensure that if fertilization occurs, the uterus is perfectly prepared to nurture the developing embryo. If fertilization doesn't happen, the system resets itself, and the cycle begins anew, ready for the next opportunity.
Phases of the Menstrual Cycle
The entire process is best understood by looking at two main, overlapping cycles that happen simultaneously:
The Ovarian Cycle: Focuses on what happens in the ovaries (egg maturation and release).
The Uterine Cycle: Focuses on what happens in the uterus (preparation and shedding of the lining).
Let's explore these coordinated events in the next section.
The Ovarian Cycle
This cycle describes the series of changes that occur within the follicles of the ovary, driven by fluctuating hormones. It is divided into three distinct phases.
A. The Follicular Phase (Day 1 to ~14)
What happens in the Ovary:
Follicle Development: Under the influence of FSH, several primordial follicles begin to grow.
Dominant Follicle Selection: Usually, only one follicle becomes the dominant (Graafian) follicle and continues to mature.
Estrogen Production: The growing dominant follicle produces increasing amounts of estrogen.
Estrogen: Initially provides negative feedback on FSH, then switches to positive feedback, leading to the LH surge.
B. Ovulation (Around Day 14)
The Trigger:
The high surge of estrogen from the dominant follicle causes a sudden, dramatic release of Luteinizing Hormone (LH) from the pituitary gland (the "LH surge").
What happens in the Ovary:
The LH surge triggers the mature dominant follicle to rupture, expelling the secondary oocyte (arrested in Metaphase II) into the fallopian tube. The egg remains viable for fertilization for around 24 hours.
C. The Luteal Phase (~Day 14 to 28)
What happens in the Ovary:
Corpus Luteum Formation: After ovulation, the ruptured follicle transforms into the corpus luteum ("yellow body").
Hormone Production: The corpus luteum produces large amounts of progesterone and some estrogen.
Fate of Corpus Luteum: It degenerates after 10-14 days if no pregnancy occurs. If pregnancy occurs, it is "rescued" by hCG to continue producing progesterone.
Hormonal Control:
Progesterone: Becomes the dominant hormone, preparing the uterus for implantation.
Negative Feedback: High progesterone and estrogen levels inhibit FSH and LH release, preventing new follicle development.
The Uterine Cycle
This cycle describes the corresponding changes occurring in the lining of the uterus (the endometrium). These changes are driven directly by the ovarian hormones, estrogen and progesterone, and are perfectly timed to coincide with the events of the ovarian cycle.
A. The Menstrual Phase (Day 1 to ~5-7)
What causes it:
This phase marks the start of the cycle (Day 1). The sharp drop in progesterone and estrogen from the degeneration of the previous cycle's corpus luteum causes the uterine lining to break down and shed, resulting in menstrual bleeding.
Purpose:
To clear out the old uterine lining, making way for a new cycle to begin.
B. The Proliferative Phase (~Day 5-7 to 14)
Driven by Estrogen:
Overlapping with the ovarian follicular phase, the rising estrogen from the dominant follicle stimulates the repair and regrowth of the endometrium.
What happens in the Uterus:
The endometrium thickens, and new blood vessels and glands develop, making the lining lush and ready to receive a fertilized egg.
C. The Secretory Phase (~Day 14 to 28)
Driven by Progesterone:
Overlapping with the ovarian luteal phase, this phase is primarily driven by the progesterone from the corpus luteum.
What happens in the Uterus:
The endometrium continues to thicken and its glands become highly secretory, producing nutrient-rich fluids (glycogen, mucus) to nourish a potential embryo and make the uterus receptive for implantation.
What Happens at the End of the Cycle?
There are two possible outcomes, which determine whether the cycle repeats or pauses.
If Pregnancy Does NOT Occur:
The corpus luteum degenerates.
Progesterone levels plummet.
The uterine lining breaks down, and a new period begins at Day 1.
If Pregnancy Occurs:
The implanted embryo produces hCG.
hCG "rescues" the corpus luteum, keeping progesterone levels high.
The uterine lining is maintained, the menstrual cycle pauses, and pregnancy is supported.
Test Your Knowledge
Check your understanding of the concepts covered in this post.
1. The ovarian cycle describes changes occurring in the __________, while the uterine cycle describes changes occurring in the ___________.
Uterus; Ovary
Ovary; Vagina
Ovary; Uterus
Uterus; Cervix
Rationale: This question defines the fundamental distinction between the two interdependent cycles. The ovarian cycle details changes in the ovaries, while the uterine cycle describes corresponding changes in the uterine lining.
2. Which hormone is primarily responsible for initiating the development of ovarian follicles at the beginning of a new cycle?
Estrogen
Progesterone
Luteinizing Hormone (LH)
Follicle-Stimulating Hormone (FSH)
Rationale: At the start of a cycle, FSH is secreted to directly target and stimulate the growth and development of ovarian follicles.
3. Ovulation typically occurs around day 14 of a 28-day cycle and is directly triggered by a surge in which hormone?
Estrogen
Progesterone
Luteinizing Hormone (LH)
Follicle-Stimulating Hormone (FSH)
Rationale: The mid-cycle surge in LH is the critical event that triggers the rupture of the mature follicle and the release of the oocyte.
4. During the proliferative phase of the uterine cycle, which event is happening?
The functional layer of the endometrium is shed.
The endometrium rebuilds itself under the influence of estrogen.
Progesterone causes the endometrium to become highly vascularized and glandular.
The corpus luteum is actively secreting progesterone.
Rationale: During the proliferative phase, rising levels of estrogen from developing follicles stimulate the rapid regeneration and thickening of the endometrium.
5. Which ovarian structure primarily secretes progesterone after ovulation to prepare the uterus for potential implantation?
Graafian follicle
Primary follicle
Corpus luteum
Corpus albicans
Rationale: After ovulation, the ruptured follicle transforms into the corpus luteum, which secretes large amounts of progesterone to maintain the uterine lining.
6. If fertilization and implantation do not occur, the corpus luteum degenerates, leading to a drop in estrogen and progesterone levels. What is the immediate consequence of this hormonal drop on the uterus?
Further thickening of the endometrium
Onset of menstruation
Ovulation
Secretion of Human Chorionic Gonadotropin (hCG)
Rationale: Without hormonal support from the corpus luteum, the functional layer of the endometrium becomes unstable and sheds, marking the beginning of menstruation.
7. The follicular phase of the ovarian cycle corresponds to which phase(s) of the uterine cycle?
Menstrual phase only
Secretory phase only
Menstrual and Proliferative phases
Proliferative and Secretory phases
Rationale: The follicular phase (days ~1-14) overlaps with the menstrual phase (days ~1-5) and the proliferative phase (days ~5-14) of the uterine cycle.
8. High levels of estrogen during the late follicular phase exert what kind of feedback on the hypothalamus and anterior pituitary, leading to the LH surge?
Negative feedback
Positive feedback
No feedback
Inhibitory feedback
Rationale: Very high levels of estrogen switch from negative to positive feedback, stimulating a massive surge of LH that triggers ovulation.
9. What is the primary role of progesterone during the secretory phase of the uterine cycle?
To cause the shedding of the endometrium.
To stimulate the growth of new ovarian follicles.
To maintain and enhance the vascularization and glandular activity of the endometrium, making it receptive to implantation.
To trigger ovulation.
Rationale: During the secretory phase, progesterone makes the endometrium highly vascularized and glandular, creating an optimal environment for a fertilized egg.
10. What is the main event that marks the beginning of the menstrual phase of the uterine cycle?
Ovulation
Implantation of a fertilized egg
Degeneration of the corpus luteum
Shedding of the functional layer of the endometrium
Rationale: The menstrual phase is defined by the shedding of the uterine lining, which marks day 1 of a new cycle.
11. The entire cycle of changes in the uterus, encompassing the menstrual, proliferative, and secretory phases, is collectively known as the _____________.
Rationale: Uterine cycle term explicitly refers to the monthly changes within the uterus itself, driven by the hormonal fluctuations from the ovarian cycle.
12. The primary ovarian event during the secretory phase of the uterine cycle is the active presence and hormonal secretion of the _____________.
Rationale: The secretory phase of the uterus is directly dependent on the high levels of progesterone produced by the corpus luteum after ovulation.
13. The release of the oocyte from the ovary is specifically called _____________.
Rationale: Ovulation is the pivotal event in the ovarian cycle where the mature oocyte is expelled from the ruptured Graafian follicle.
14. If pregnancy occurs, the developing embryo produces the hormone _____________, which signals the corpus luteum to continue producing progesterone, thus maintaining the uterine lining.
Rationale: hCG acts like LH, "rescuing" the corpus luteum and ensuring continuous progesterone support for the developing pregnancy. This is the hormone detected by pregnancy tests.
15. During the early follicular phase, the rising levels of estrogen exert a ___________ feedback on the release of FSH and LH, preventing the development of too many follicles.
Rationale: Moderate and rising levels of estrogen during the early follicular phase provide negative feedback to the pituitary, which helps to select a single dominant follicle and suppress the growth of others.
Gametogenesis is the fundamental biological process where a diploid cell (2n), specifically a primordial germ cell, undergoes meiosis to form a haploid gamete (n). In simpler terms, it's the creation of sex cells.
In males, this process is called spermatogenesis and results in the production of spermatozoa (sperm). In females, it is called oogenesis, which leads to the formation of an ovum (egg).
Purpose of Gametogenesis
To produce genetically diverse haploid gametes (sperm and egg) that are ready for fertilization. The fusion of these cells forms a diploid zygote, initiating the development of a new, genetically unique individual.
Where It Happens (The Gonads)
In Males: The testes
In Females: The ovaries
Common Terms to Know First
Understanding the following vocabulary is essential for grasping the concepts of gametogenesis.
Diploid (2n) vs. Haploid (n)
Diploid cells contain two complete sets of chromosomes (46 in humans), one from each parent. Most body cells are diploid. Haploid cells contain only a single set of chromosomes (23 in humans). Gametes are haploid.
Primordial Germ Cells (PGCs)
The earliest recognizable precursor cells for gametes. They originate outside the gonads during embryonic development and migrate into them.
Mitosis
Standard cell division that produces two identical diploid daughter cells. Used to multiply the number of precursor germ cells before meiosis begins.
Meiosis
A specialized two-stage cell division that reduces the chromosome number by half, producing four genetically unique haploid cells from one diploid cell.
Meiosis I: The "reductional division" where homologous chromosome pairs are separated, making the cells haploid. Meiosis II: Similar to mitosis, where sister chromatids are separated.
1. The Fundamental Purpose of Reproduction
At its core, reproduction is the biological process by which new individual organisms are produced from their parents. It is a defining characteristic of all known life, and it ensures the continuation of a species from one generation to the next. Without reproduction, a species would become extinct.
A. Asexual vs. Sexual Reproduction
There are two primary modes of reproduction, each with distinct characteristics and evolutionary implications:
Asexual Reproduction
Definition: Involves a single parent producing offspring that are genetically identical to itself. There is no fusion of gametes.
Mechanisms:
Binary Fission: (e.g., bacteria, amoeba) A single cell divides into two identical daughter cells.
Budding: (e.g., yeast, hydra) A new organism grows out from the body of the parent.
Fragmentation: (e.g., starfish, planaria) A parent organism breaks into fragments, and each fragment develops into a new individual.
Vegetative Propagation: (e.g., plants) New plants grow from parts of the parent plant (stems, leaves, roots).
Parthenogenesis: (e.g., some insects, reptiles) Development of an embryo from an unfertilized egg.
Advantages:
Rapid population growth: Can produce many offspring quickly.
No need for a mate: Beneficial in sparsely populated or harsh environments.
Energy efficient: Less energy investment compared to finding a mate and gamete production/fertilization.
Successful in stable environments: If the parent is well-adapted, offspring will also be well-adapted.
Disadvantages:
Lack of genetic diversity: Offspring are clones, making the entire population vulnerable to environmental changes, diseases, or new predators.
Limited adaptation: Slower evolution due to lack of variation.
Sexual Reproduction
Definition: Involves two parents contributing genetic material to produce offspring that are genetically unique. This typically involves the fusion of two specialized reproductive cells called gametes (sperm and egg).
Mechanisms:
Fertilization: The fusion of male and female gametes to form a zygote.
Meiosis: A specialized type of cell division that produces haploid gametes from diploid germline cells (which we will delve into next!).
Advantages:
Genetic diversity: Generates new combinations of alleles through meiosis (crossing over, independent assortment) and the random fusion of gametes. This variation is the raw material for natural selection.
Adaptation: Increased diversity allows populations to adapt to changing environments, resist diseases, and evolve.
Removal of deleterious mutations: Sexual reproduction can help purge harmful mutations from a population more effectively over time.
Disadvantages:
Slower reproduction rate: Typically fewer offspring produced.
Energy intensive: Requires finding a mate, courtship, and often parental care.
Risk of disease transmission: Can facilitate the spread of sexually transmitted diseases.
In humans and most complex animals, sexual reproduction is the primary mode, emphasizing the crucial role of genetic diversity in long-term species survival and adaptation.
2. The Role of Meiosis in Gametogenesis
Sexual reproduction relies on the fusion of two gametes, each contributing a set of chromosomes. To ensure that the offspring ends up with the correct number of chromosomes (and not double the amount with each generation), a specialized cell division called Meiosis is essential.
A. Overview of Chromosome Number:
Diploid (2n): Cells that contain two sets of homologous chromosomes (one set inherited from each parent). Somatic (body) cells are diploid. In humans, 2n = 46 chromosomes.
Haploid (n): Cells that contain only one set of chromosomes. Gametes (sperm and egg) are haploid. In humans, n = 23 chromosomes.
B. What is Meiosis?
Meiosis is a two-step cell division process that transforms one diploid cell into four genetically distinct haploid cells (gametes). It is unique to sexually reproducing organisms and has two main goals:
Reduce the chromosome number by half: From diploid (2n) to haploid (n).
Generate genetic diversity: Through processes we've touched upon before, and will elaborate here.
C. Stages of Meiosis:
Meiosis involves two consecutive cell divisions, Meiosis I and Meiosis II, each with prophase, metaphase, anaphase, and telophase stages.
Meiosis I (Reductional Division)
Homologous chromosomes separate.
Prophase I:
Chromosomes condense and become visible.
Synapsis: Homologous chromosomes pair up, forming bivalents (or tetrads, as they consist of four chromatids).
Crossing Over: Non-sister chromatids of homologous chromosomes exchange genetic material at points called chiasmata. This is a critical event for genetic recombination and creating new allele combinations on chromatids.
Homologous chromosome pairs (bivalents) align randomly at the metaphase plate.
Independent Assortment: The orientation of each homologous pair is random and independent of other pairs. This further shuffles genetic information.
Anaphase I: Homologous chromosomes separate and move to opposite poles of the cell. Sister chromatids remain attached.
Telophase I & Cytokinesis:
Chromosomes decondense (partially).
Nuclear envelopes may reform.
Cytokinesis divides the cytoplasm, resulting in two haploid cells (each chromosome still consists of two sister chromatids).
Meiosis II (Equational Division)
Sister chromatids separate. This division is very similar to mitosis.
Prophase II: Chromosomes condense again (if they decondensed). Nuclear envelope breaks down; spindle fibers form.
Metaphase II: Chromosomes (each still with two sister chromatids) align individually at the metaphase plate.
Anaphase II: Sister chromatids separate and move to opposite poles, now considered individual chromosomes.
Telophase II & Cytokinesis:
Chromosomes decondense.
Nuclear envelopes reform.
Cytokinesis divides the cytoplasm, resulting in a total of four haploid cells, each with single, unreplicated chromosomes.
D. How Meiosis Contributes to Genetic Variation:
Meiosis is a powerhouse of genetic diversity, achieving it through three main mechanisms:
Crossing Over (Prophase I):
Exchange of genetic material between non-sister chromatids of homologous chromosomes.
Breaks old combinations of alleles and creates new ones on the chromatids.
For example, if a chromosome initially carried alleles AB, after crossing over it might carry Ab or aB.
Independent Assortment of Homologous Chromosomes (Metaphase I):
The random orientation of homologous pairs at the metaphase plate means that the maternal and paternal chromosomes are segregated into daughter cells independently of other pairs.
For an organism with 'n' pairs of chromosomes, there are 2^n possible combinations of chromosomes in the resulting gametes. In humans (n=23), this is over 8 million (2^23) possibilities!
Random Fertilization:
The fusion of any one male gamete with any one female gamete further increases the number of possible genetic combinations in the zygote. The odds of two children from the same parents being genetically identical (except for identical twins) are astronomically small.
Spermatogenesis: The Formation of Sperm
Spermatogenesis is the continuous process of producing sperm (male gametes) in the testes. It's a marvel of biological engineering, designed to create a vast number of highly specialized cells capable of fertilization.
Timing
Begins at puberty (10-16 years) and continues throughout adult life.
Location
Within the seminiferous tubules of the testes.
Quantity
Enormous output of ~200 million sperm per day.
The Blood-Testis Barrier: Protecting the Sperm
Sertoli cells form a critical barrier that prevents substances from the blood from harming developing sperm. It also shields the genetically different sperm from the male's own immune system, which would otherwise recognize them as foreign and attack them.
Terms in Spermatogenesis
Before diving into the process, it's crucial to understand the key cell types involved.
Spermatogonium
The diploid (2n) stem cells in the testes that initiate the process.
Primary Spermatocyte
A diploid (2n) cell that has grown and is ready to undergo Meiosis I.
Secondary Spermatocyte
The two haploid (n) cells resulting from Meiosis I.
Spermatid
The four haploid (n), round, immature cells resulting from Meiosis II.
Spermiogenesis
The final maturation stage where spermatids are physically remodeled into spermatozoa. This is not cell division.
Spermatozoon (Sperm)
The mature, motile male gamete with a head (containing the nucleus and acrosome), midpiece, and tail.
The Stages of Spermatogenesis
The journey from a basic stem cell to four spermatids involves a carefully orchestrated sequence of mitosis and meiosis.
1. Proliferation (Mitosis)
Diploid spermatogonia divide by mitosis to create a pool of precursor cells. Some remain as stem cells for continuous production, while others (Type B) are committed to becoming sperm.
2. Growth
The Type B spermatogonium grows and replicates its DNA, becoming a primary spermatocyte (still 2n, but with duplicated chromosomes).
3. First Meiotic Division (Meiosis I)
The primary spermatocyte divides, separating homologous chromosomes. This results in two haploid secondary spermatocytes (n).
4. Second Meiotic Division (Meiosis II)
Each secondary spermatocyte divides again, separating sister chromatids. This produces a total of four haploid spermatids (n).
Final Maturation and Journey
The spermatids created through meiosis are not yet functional. They must undergo a final transformation and journey to become capable of fertilization.
Spermiogenesis: The Transformation
During this dramatic remodeling phase, the round spermatid:
Forms a head with a condensed nucleus and an enzyme-filled acrosome cap.
Develops a midpiece packed with mitochondria for energy.
Grows a long tail (flagellum) for movement.
Sheds most of its cytoplasm to become lightweight.
Once this is complete, the cells are called spermatozoa and are released into the tubule lumen in a process called spermiation.
The Journey to Maturity
Immature sperm travel from the seminiferous tubules through the rete testis and into the epididymis. The epididymis is the "finishing school" where sperm spend several weeks to gain full motility and the ability to fertilize an egg. It also serves as the primary storage site.
Capacitation: The Final Activation
Even after leaving the epididymis, sperm are not ready. Capacitation is a final series of biochemical changes that occurs within the female reproductive tract. It destabilizes the sperm's acrosome membrane, making it capable of releasing its enzymes to penetrate the egg. Without capacitation, fertilization cannot occur.
3. Detail the Process of Spermatogenesis (Male Gamete Formation)
Spermatogenesis is the process by which male primordial germ cells (spermatogonia) develop into mature spermatozoa (sperm). This continuous process occurs in the male gonads, the testes, specifically within the walls of the seminiferous tubules. It begins at puberty and continues throughout a male's life.
A. Site of Spermatogenesis:
Seminiferous Tubules: Coiled tubes located within the testes. These tubules contain two main cell types critical for sperm production:
Spermatogenic cells: These are the cells undergoing meiosis and differentiation to become sperm.
Sertoli cells (or sustentacular cells): These are "nurse cells" that support, protect, and nourish the developing spermatogenic cells. They also form the blood-testis barrier and produce hormones (like inhibin).
Leydig cells (or interstitial cells): Located in the connective tissue between the seminiferous tubules, these cells produce androgens, primarily testosterone, which is essential for spermatogenesis and the development of male secondary sexual characteristics.
B. Stages of Spermatogenesis:
Spermatogenesis is a highly organized process involving three main phases: mitosis, meiosis, and spermiogenesis. It takes approximately 64-72 days in humans.
1. Proliferation (Mitosis)
Spermatogonia (2n): These are diploid (2n=46) stem cells located in the outermost layer of the seminiferous tubule wall, near the basement membrane. Throughout life, spermatogonia continually divide by mitosis. Some daughter cells remain as spermatogonia to maintain the stem cell pool, while others differentiate into primary spermatocytes.
2. Meiosis
Primary Spermatocyte (2n): A diploid cell that enters Meiosis I. Undergoes Meiosis I to produce two secondary spermatocytes.
Secondary Spermatocyte (n): Each is haploid (n=23), but chromosomes still consist of two sister chromatids. Each undergoes Meiosis II to produce two spermatids.
Spermatid (n): Each is haploid (n=23) and now has single, unreplicated chromosomes. They are round cells and not yet motile.
Summary of Meiosis in Spermatogenesis:
One primary spermatocyte (2n) yields two secondary spermatocytes (n).
Two secondary spermatocytes (n) yield four spermatids (n).
Therefore, one primary spermatocyte ultimately produces four haploid spermatids.
3. Spermiogenesis (Differentiation)
This is the final stage where spermatids undergo a remarkable morphological transformation into mature, motile spermatozoa (sperm). No further cell division occurs here.
Key changes include:
Head Formation: The nucleus condenses and flattens. The acrosome, a cap-like organelle derived from the Golgi apparatus, forms over the anterior part of the nucleus. The acrosome contains enzymes vital for penetrating the egg.
Midpiece Formation: Mitochondria cluster around the base of the flagellum, forming the midpiece, which provides ATP for flagellar movement.
Tail (Flagellum) Formation: Microtubules organize to form a long flagellum, providing motility.
Cytoplasm Shedding: Most excess cytoplasm is shed, making the sperm streamlined for movement.
C. Mature Spermatozoon Structure:
A mature sperm cell is highly specialized for delivering male genetic material to the egg:
Head: Contains the condensed haploid nucleus (genetic material) and the acrosome.
Midpiece: Contains numerous mitochondria to power the flagellum.
Tail (Flagellum): Provides motility, allowing the sperm to swim towards the egg.
D. Timing of Spermatogenesis:
Begins at puberty due to the surge in testosterone.
Continuous process throughout a male's reproductive life, though production may decrease with age.
The entire cycle from spermatogonium to mature spermatozoon takes approximately 64-72 days.
Oogenesis: The Formation of the Ovum
Oogenesis is the biological process by which ova (egg cells) are produced in the ovaries. It begins with primordial germ cells that colonise the cortex of the primordial gonad, multiplying to a peak of approximately 7 million by mid-gestation before a process of cell death (atresia) begins.
Crucially, Meiosis I begins before birth, forming all the primary oocytes a female will ever have. This means there is a finite supply of ova.
Key Differences from Spermatogenesis
Timing: Starts before birth, pauses, and ends at menopause.
Quantity: Produces only one large, functional ovum and smaller polar bodies per division.
Nature: A cyclic process after puberty, releasing one egg per menstrual cycle.
Terms in Oogenesis
Understanding the unique vocabulary of female gamete formation is essential.
Oogonium
The diploid (2n) stem cells in the fetal ovary that divide by mitosis.
Primary Oocyte
A diploid (2n) cell that enters Meiosis I but is arrested in Prophase I before birth.
Secondary Oocyte
The large, haploid (n) cell produced after Meiosis I is completed. It is arrested in Metaphase II and is the cell released during ovulation.
Ovum
The mature haploid (n) egg cell, formed only after the secondary oocyte is fertilized by a sperm, triggering the completion of Meiosis II.
Polar Body
A small, non-functional haploid cell produced during unequal divisions, serving to discard excess chromosomes.
Ovarian Follicle (e.g., Graafian Follicle)
The functional unit of the ovary, a fluid-filled sac containing the developing oocyte and hormone-producing cells.
The Stages of Oogenesis
Oogenesis is a prolonged process that occurs in three distinct phases, punctuated by long periods of arrest.
Phase 1: Before Birth (Fetal Ovary)
Oogonia multiply via mitosis. Many differentiate into primary oocytes, which then begin Meiosis I but are immediately arrested in Prophase I. A female is born with her lifetime supply of these arrested primary oocytes.
Phase 2: From Puberty to Menopause (Monthly Cycles)
Each month, hormonal signals cause a primary oocyte to complete Meiosis I. This division is unequal, producing one large, haploid secondary oocyte and one small first polar body. The secondary oocyte then begins Meiosis II but is arrested again in Metaphase II. This is the stage at which ovulation occurs.
Phase 3: Only Upon Fertilization
Meiosis II is only completed if the secondary oocyte is fertilized by a sperm. The sperm's entry triggers the final division, producing one large, mature ovum and a tiny second polar body. If fertilization does not occur, the arrested secondary oocyte degenerates.
Follicular Development
The maturation of the oocyte happens within a structure called the ovarian follicle, which also undergoes its own development.
Pre-antral Stage: The primary oocyte is surrounded by follicular cells that grow and secrete glycoproteins, forming the zona pellucida.
Antral Stage: A fluid-filled space called the antrum forms, creating a secondary follicle.
Preovulatory Stage: Triggered by an LH surge, Meiosis I completes, and the mature follicle (Graafian follicle) prepares for ovulation.
4. Detail the Process of Oogenesis (Female Gamete Formation)
Oogenesis is the process by which female primordial germ cells (oogonia) develop into mature ova (eggs). Unlike spermatogenesis, oogenesis is a discontinuous process, beginning before birth and completing only after fertilization. It occurs in the female gonads, the ovaries, within structures called follicles.
A. Site of Oogenesis:
Ovaries: Female gonads where ova are produced and mature within follicles.
Ovarian Follicles: Structures within the ovary that consist of an oocyte surrounded by one or more layers of support cells (granulosa cells). These cells nurture the developing oocyte and produce hormones (estrogens, progesterone).
B. Stages of Oogenesis:
Oogenesis involves phases of mitosis, meiosis, and growth, but with crucial differences in timing and cytoplasmic division compared to spermatogenesis.
1. Proliferation (Mitosis) - Occurs before birth
Oogonia (2n): Diploid (2n=46) stem cells in the fetal ovary. These multiply rapidly by mitosis during fetal development. By the fifth month of gestation, all oogonia that will ever develop are formed (up to 7 million). Many degenerate, but those remaining grow into primary oocytes. No new oogonia are formed after birth.
2. Meiosis - Highly Asynchronous
Primary Oocyte (2n): A diploid cell that enters Meiosis I. Each primary oocyte becomes enclosed by a single layer of flattened follicular cells, forming a primordial follicle. Primary oocytes enter Prophase I of Meiosis during fetal development but then arrest at this stage. They remain arrested for years, even decades, until puberty.
At Puberty: Starting at puberty, usually one primary oocyte per month is stimulated by hormones to resume meiosis. It completes Meiosis I to produce two unequal cells: a large secondary oocyte and a small first polar body. This unequal division (cytokinesis) ensures that the secondary oocyte retains most of the cytoplasm and nutrients. The first polar body may or may not divide again.
Secondary Oocyte (n): This haploid (n=23, chromosomes with two chromatids) large cell enters Meiosis II. It then arrests at Metaphase II. The secondary oocyte is released from the ovary during ovulation.
If fertilization occurs: The secondary oocyte completes Meiosis II to produce a large ovum (n=23, single chromatids) and a small second polar body.
If fertilization does NOT occur: The secondary oocyte degenerates without completing Meiosis II.
Ovum (n): The mature female gamete, fully haploid with single chromatids, ready for fusion with sperm.
Summary of Meiosis in Oogenesis:
One primary oocyte (2n) yields one secondary oocyte (n) and one first polar body.
One secondary oocyte (n) yields one ovum (n) and one second polar body only if fertilized.
Therefore, one primary oocyte ultimately produces only one functional ovum and two or three non-functional polar bodies.
C. Timing of Oogenesis:
Initiation: Begins in the fetal ovary.
Arrested Development: Primary oocytes are arrested in Prophase I from fetal life until puberty. Secondary oocytes are arrested in Metaphase II until fertilization.
Completion: Meiosis II is only completed upon successful fertilization.
Discontinuous: Occurs in phases over many years.
5. Compare and Contrast Spermatogenesis and Oogenesis
Both spermatogenesis and oogenesis are processes of gametogenesis, involving meiosis to produce haploid gametes. However, they exhibit significant differences tailored to their distinct roles in reproduction.
A. Similarities:
Involve Meiosis: Both processes utilize meiosis (Meiosis I and Meiosis II) to reduce the chromosome number from diploid (2n) to haploid (n), ensuring that the zygote formed upon fertilization has the correct diploid number of chromosomes.
Produce Haploid Gametes: Both ultimately result in the formation of haploid cells (sperm and ovum) containing half the number of chromosomes of a somatic cell.
Involve Mitosis: Both processes begin with the mitotic proliferation of primordial germ cells (spermatogonia and oogonia) to increase their numbers.
Occur in Gonads: Both take place in the respective primary reproductive organs: testes for spermatogenesis and ovaries for oogenesis.
Subject to Hormonal Control: Both processes are regulated by complex hormonal pathways involving the hypothalamic-pituitary-gonadal (HPG) axis.
Genetic Recombination: Both benefit from genetic recombination events (crossing over and independent assortment) during meiosis, contributing to genetic diversity.
B. Key Differences:
Feature
Spermatogenesis
Oogenesis
Location
Testes (seminiferous tubules)
Ovaries (within follicles)
Timing
Starts at puberty, continuous throughout life
Starts during fetal development, discontinuous, ends at menopause
Duration of Process
Approximately 64-72 days (continuous cycle)
Many years (from fetal life to potential fertilization)
Number of Gametes from 1 Primary Cell
Four functional spermatozoa from one primary spermatocyte
One functional ovum and 2-3 polar bodies from one primary oocyte
Size of Gametes
Small, motile (spermatozoa)
Large, non-motile (ovum), rich in cytoplasm and nutrients
Cytokinesis
Equal division of cytoplasm during meiosis
Unequal division of cytoplasm during meiosis, forming polar bodies
Continuity
Continuous and prolific
Intermittent (typically one oocyte per month) and limited
Completion of Meiosis II
Completed before maturation
Completed only upon fertilization
Hormonal Control
LH stimulates Leydig cells (testosterone); FSH acts on Sertoli cells
LH and FSH stimulate follicular development, estrogen, and progesterone production; surge of LH triggers ovulation
C. Evolutionary Significance of Differences:
The distinct strategies for gamete formation reflect evolutionary adaptations:
Sperm Production: The male strategy is to produce vast numbers of small, motile gametes (sperm) to maximize the chances of reaching and fertilizing an egg. The continuous nature and equal cytoplasmic division support this high-volume production.
Egg Production: The female strategy is to produce a limited number of large, nutrient-rich gametes (ova) that can support early embryonic development. The unequal cytoplasmic division ensures that the ovum receives all the necessary organelles and nutrients for the initial stages of a new organism. The long and arrested development stages allow for careful selection and maturation of a few high-quality ova.
This comparison highlights how both processes achieve the same fundamental goal (producing haploid gametes) but with profoundly different mechanisms, each optimized for its role in sexual reproduction.
Understand the Hormonal Regulation of Male Reproductive Function
Male reproductive function, including spermatogenesis and the development of male secondary sexual characteristics, is exquisitely controlled by a complex interplay of hormones, primarily orchestrated by the hypothalamic-pituitary-gonadal (HPG) axis.
A. The Hypothalamic-Pituitary-Gonadal (HPG) Axis (Male)
This axis involves three key endocrine glands that communicate with each other:
1Hypothalamus: Located in the brain, master regulator.
2Anterior Pituitary Gland: Base of brain, stimulated by hypothalamus.
3Testes (Gonads): Primary reproductive organs.
B. Key Hormones and Their Roles
Gonadotropin-Releasing Hormone (GnRH)
Source: Hypothalamus.
Action: Released in a pulsatile manner. Travels via portal system to anterior pituitary to stimulate release of gonadotropins.
Luteinizing Hormone (LH)
Source: Anterior Pituitary.
Action: Acts on Leydig cells (interstitial cells). Stimulates them to produce and secrete Testosterone.
Follicle-Stimulating Hormone (FSH)
Source: Anterior Pituitary.
Action: Acts on Sertoli cells (sustentacular cells). Stimulates spermatogenesis (maturation) and production of Androgen-Binding Protein (ABP) to keep testosterone high in tubules.
Testosterone (Androgen)
Source: Leydig cells (stimulated by LH).
Actions:
Initiation/Maintenance of spermatogenesis.
Male secondary sexual characteristics (muscle, voice, hair, libido).
Maintenance of reproductive organs (prostate, etc.).
Negative Feedback: Inhibits GnRH, LH, and FSH.
Inhibin
Source: Sertoli cells.
Action: Selectively inhibits FSH secretion from anterior pituitary. (Feedback for sperm production rate).
C. Negative Feedback Mechanisms
The HPG axis operates under a tight negative feedback loop:
Testosterone's Feedback
High levels inhibit GnRH (Hypothalamus) and LH/FSH (Pituitary). Prevents overproduction.
Nervous tissue is the master controller and communication system of the body. It forms the brain, spinal cord, and peripheral nerves, and its primary function is to regulate and integrate all body functions by rapidly transmitting electrical signals.
The Two Main Cell Types
The nervous system is comprised of two principal types of cells that work in concert.
Neurons (Nerve Cells)
These are the primary functional cells that are specialized to transmit electrical signals (nerve impulses). They send and receive messages using chemical signals called neurotransmitters across junctions known as synapses.
Neuroglia (Glial Cells)
These are the non-excitable, supporting cells of the nervous system. They provide physical and metabolic support, insulation (myelin), and immune defense for the neurons. Examples include Astrocytes, Oligodendrocytes, and Schwann Cells.
General Characteristics
Primary Function: To receive stimuli, transmit electrical impulses, and process information to control the body's responses.
Location: Makes up the Central Nervous System (CNS)—the brain and spinal cord—and the Peripheral Nervous System (PNS)—the peripheral nerves.
Key Properties of Neurons
Excitability
The ability to respond to a stimulus by generating an electrical change across its membrane (membrane potential).
Conductivity
The ability to propagate these electrical signals (nerve impulses or action potentials) rapidly along the cell membrane.
The Neuron (Nerve Cell): The Signaling Unit
Neurons are the excitable cells responsible for transmitting electrical signals. They are typically long-lived, amitotic (do not divide in their mature form), and have a very high metabolic rate, requiring a continuous supply of oxygen and glucose to function.
1. Structural Components of a Typical Neuron
Cell Body (Soma)
The neuron's main nutritional and metabolic center. It contains the nucleus, most organelles, and prominent Nissl bodies (rough ER), reflecting its high rate of protein synthesis.
Dendrites
Numerous, short, highly branched processes that act as the main receptive regions. They receive incoming signals from other neurons and convey them towards the cell body.
Axon
A single, long process that acts as the conducting region, generating and transmitting nerve impulses (action potentials) away from the cell body. It terminates in branches called axon terminals.
The Myelin Sheath
Many axons are covered by a fatty, insulating layer called the myelin sheath, which is formed by glial cells (Schwann cells in the PNS and oligodendrocytes in the CNS). This sheath dramatically speeds up nerve impulse transmission. The gaps between the myelin segments are called Nodes of Ranvier, where the action potential "jumps" from node to node (saltatory conduction).
2. Functional Classification of Neurons
Sensory (Afferent)
Transmit impulses from sensory receptors towards the CNS.
Motor (Efferent)
Transmit impulses from the CNS to effector organs (muscles/glands).
Interneurons
Lie between sensory and motor neurons within the CNS to integrate information. Most neurons are interneurons.
3. Structural Classification of Neurons
Multipolar
Three or more processes (one axon, many dendrites). The most common type in the CNS.
Bipolar
Two processes (one axon, one dendrite). Rare; found in special sense organs like the retina.
Unipolar
A single, short process that divides T-like. Found in most sensory neurons in the PNS.
Neuroglia (Glial Cells): The Supporting Cast
Neuroglia are non-excitable cells that surround, support, insulate, and protect neurons. They are far more numerous than neurons and can divide throughout life. There are six types of neuroglia: four in the CNS and two in the PNS.
A. Neuroglia of the Central Nervous System (CNS)
Astrocytes (Star Cells)
Most abundant and versatile. Anchor neurons to blood vessels (form the blood-brain barrier) and regulate the chemical environment.
Microglial Cells
The resident macrophages of the CNS. They monitor neuron health and phagocytize microorganisms and debris.
Ependymal Cells
Line the central cavities of the brain and spinal cord. Their cilia help circulate cerebrospinal fluid (CSF).
Oligodendrocytes
Form the myelin sheaths around axons in the CNS. One oligodendrocyte can myelinate several axons.
B. Neuroglia of the Peripheral Nervous System (PNS)
Satellite Cells
Surround neuron cell bodies in PNS ganglia, providing support and regulating the chemical environment.
Schwann Cells
Form the myelin sheaths around thicker axons in the PNS. One Schwann cell myelinates one segment of one axon. Crucial for regeneration.
Nerve Impulse (Action Potential) Generation and Transmission
The ability of neurons to communicate relies on their ability to generate and transmit electrical signals, a process that involves several key stages.
1. Resting Membrane Potential
A neuron at rest has a voltage difference across its membrane of about -70mV. This is maintained by the sodium-potassium pump and ion leak channels.
2. Graded Potentials
Short-lived, localized changes in membrane potential. If a graded potential is strong enough to reach the threshold potential (~ -55mV) at the axon hillock, it triggers an action potential.
3. Action Potential (Nerve Impulse)
A brief, rapid, all-or-none electrical impulse that travels down the axon. It involves a depolarization phase (Na⁺ rushes in) followed by a repolarization phase (K⁺ rushes out).
4. Synapses
The junction where information is transferred. An arriving action potential causes the release of chemical messengers called neurotransmitters across a tiny gap (the synaptic cleft), which then bind to the next cell.
Test Your Knowledge
Check your understanding of the concepts covered in this post.
1. Which of the following is the primary function of nervous tissue?
Support and protect organs
Contract and generate force
Transmit electrical signals and process information
Form linings and glandular secretions
Rationale: This is the overarching function of nervous tissue, allowing for rapid communication and complex thought processes.
2. The two main types of cells found in nervous tissue are:
Epithelial cells and glial cells
Neurons and muscle cells
Neurons and neuroglia
Fibroblasts and oligodendrocytes
Rationale: Neurons are the excitable, signaling cells, while neuroglia (glial cells) are the supporting cells.
3. Which part of a neuron typically receives incoming signals from other neurons?
Axon
Axon terminal
Dendrite
Myelin sheath
Rationale: Dendrites are the highly branched receptive regions that receive neurotransmitter signals from other neurons.
4. The ability of a neuron to respond to a stimulus by changing its membrane potential is called:
Conductivity
Contractility
Excitability
Secretion
Rationale: Excitability is the fundamental property of neurons (and muscle cells) to respond to stimuli by generating an electrical impulse.
5. Which glial cell type forms the myelin sheath in the Central Nervous System (CNS)?
Schwann cells
Astrocytes
Microglial cells
Oligodendrocytes
Rationale: Oligodendrocytes are the glial cells responsible for myelinating axons in the CNS.
6. Which type of neuron transmits impulses from sensory receptors towards the CNS?
Motor (efferent) neuron
Sensory (afferent) neuron
Interneuron
Neuroglia
Rationale: Afferent neurons carry sensory information towards the CNS.
7. Gaps in the myelin sheath along an axon are called:
Synaptic clefts
Nodes of Ranvier
Axon hillocks
Dendritic spines
Rationale: These unmyelinated gaps allow for saltatory conduction, where the action potential "jumps," speeding up transmission.
8. Which glial cells are phagocytic and act as the "immune cells" of the CNS?
Ependymal cells
Satellite cells
Microglial cells
Astrocytes
Rationale: Microglial cells are the resident immune cells of the CNS, functioning as phagocytes to remove debris and pathogens.
9. The region where an action potential is typically generated in a neuron is the:
Dendrite
Cell body
Axon hillock
Axon terminal
Rationale: The axon hillock is the "trigger zone" where graded potentials summate, and if threshold is reached, an action potential is initiated.
10. Which statement best describes the primary role of the axon?
To integrate incoming signals.
To produce neurotransmitters.
To transmit nerve impulses away from the cell body.
To form the blood-brain barrier.
Rationale: The axon's primary role is to conduct the action potential from the cell body to the axon terminals, propagating the signal.
11. The long, single process of a neuron that transmits signals away from the cell body is called the _____________.
Rationale: This describes the core function and structure of the axon.
12. The fatty, insulating layer that speeds up nerve impulse transmission is the _____________.
Rationale: The myelin sheath is critical for efficient and rapid signal propagation in many neurons.
13. In the Peripheral Nervous System (PNS), the glial cells that form myelin sheaths are called _____________.
Rationale: This distinguishes the myelin-forming cells in the PNS from those in the CNS (oligodendrocytes).
14. The specialized junctions where neurons communicate with other cells by releasing neurotransmitters are called _____________.
Rationale: Synapses are the crucial points of information transfer between neurons or between neurons and effector cells.
15. Star-shaped glial cells that help form the blood-brain barrier and regulate the chemical environment in the CNS are called _____________.
Rationale: Astrocytes are the most abundant and versatile glial cells in the CNS, with numerous vital supportive roles.
Muscle tissue is composed of highly specialized, contractile cells that generate force to produce movement. The cells within all three types of muscle tissue are specialized for contraction (shortening), a process enabled by the interaction of specialized protein fibers. This contraction enables the movement of the whole body and many internal organs, in addition to producing heat energy.
An important characteristic is that mature muscle cells have generally lost the ability to divide, so destroyed muscle cells often cannot be replaced.
General Characteristics
All muscle tissues share a set of key properties that allow them to function effectively.
Excitability (Responsiveness)
The ability to receive and respond to a stimulus (like a nerve impulse).
Contractility
The ability to shorten forcibly when stimulated.
Extensibility
The ability to be stretched or extended.
Elasticity
The ability to recoil and resume its resting length after stretching.
The Three Types of Muscle Tissue
Muscle tissue is classified into three types based on location, structure, and functional characteristics. While the cells in smooth and cardiac muscle are referred to as muscle cells, the long, cylindrical cells of skeletal muscle are often called muscle fibers.
1. Skeletal Muscle
Striated
(Striped appearance)
Voluntary
(Under conscious control)
Multinucleate
(Long, cylindrical cells)
Location: Primarily attached to the skeleton, enabling body movement.
2. Cardiac Muscle
Striated
(Striped appearance)
Involuntary
(Not under conscious control)
Branched Cells
(Connected by intercalated discs)
Location: Found exclusively in the wall of the heart.
3. Smooth Muscle
Non-striated
(Smooth appearance)
Involuntary
(Not under conscious control)
Spindle-shaped Cells
(Single central nucleus)
Location: Found in the walls of hollow organs like the stomach, bladder, and blood vessels.
Skeletal Muscle
Named for its location, skeletal muscle tissue is usually attached to bones and skin, enabling movement of the head, trunk, and limbs. Its contractions are voluntary (under conscious control).
Key Characteristics:
Striated: Appears striped or banded due to the highly organized arrangement of contractile proteins (actin and myosin).
Voluntary: Contraction is consciously controlled by the nervous system.
Multi-nucleated Fibers: The cells (muscle fibers) are long, cylindrical, and contain multiple nuclei located at the periphery.
General Organization (Macroscopic to Microscopic)
A whole skeletal muscle is a complex organ containing muscle fibers, blood vessels, nerve fibers, and extensive connective tissue wrappings that hold everything together and transmit the force of contraction.
1. Entire Muscle
The whole organ, surrounded by a dense irregular CT layer called the Epimysium.
2. Muscle Fascicle
A bundle of muscle fibers, surrounded by a fibrous CT layer called the Perimysium.
3. Muscle Fiber (Cell)
A single muscle cell, surrounded by a delicate areolar CT layer called the Endomysium.
These three "mysiums" are continuous and converge to form tendons, which transmit the contractile force to the bones.
Microscopic Organization of a Muscle Fiber
A skeletal muscle fiber is a highly specialized, elongated cell optimized for rapid and powerful contraction.
Sarcolemma & Sarcoplasm
The Sarcolemma is the cell membrane, featuring deep invaginations called T-tubules. The Sarcoplasm is the cytoplasm, rich in glycogen (glycosomes) and oxygen-storing myoglobin.
Sarcoplasmic Reticulum (SR)
A specialized smooth ER that surrounds each myofibril. Its primary role is to store and release calcium ions (Ca²⁺), the critical trigger for muscle contraction.
Myofibrils and the Sarcomere
Myofibrils are the rod-like contractile elements that make up ~80% of the muscle fiber's volume. Each myofibril is a chain of repeating sarcomeres, the smallest functional unit of muscle contraction.
Sarcomere Banding Pattern (Striations)
A-Band (Dark): Represents the full length of the thick (myosin) filaments.
I-Band (Light): Contains only thin (actin) filaments.
Z-Disc (Line): A protein sheet that anchors thin filaments and defines the boundaries of one sarcomere.
Myofilaments (Contractile Proteins)
Thick Filaments (Myosin): Composed of myosin protein with globular heads that bind to actin and use ATP to generate force.
Thin Filaments (Actin): Composed of actin protein, which has binding sites for myosin heads. Also contains two regulatory proteins:
Tropomyosin: Blocks the myosin-binding sites on actin in a relaxed muscle.
Troponin: Binds to Ca²⁺, which causes it to move tropomyosin, exposing the binding sites and allowing contraction to begin.
The Sliding Filament Model of Contraction
This is how muscles contract:
A nerve impulse triggers the release of Ca²⁺ from the Sarcoplasmic Reticulum.
Ca²⁺ binds to troponin, causing it to move tropomyosin away from actin's binding sites.
Myosin heads bind to actin, forming a cross-bridge.
The myosin heads pivot, pulling the thin filaments toward the center of the sarcomere (the "power stroke"). This uses ATP.
The myosin head detaches, re-cocks, and is ready for another cycle as long as Ca²⁺ and ATP are present.
This sliding action shortens all the sarcomeres simultaneously, causing the entire muscle fiber to contract.
Satellite Cells
These are quiescent (inactive) stem cells located on the surface of mature muscle fibers. When a muscle fiber is injured, satellite cells become activated. They divide and differentiate into new muscle cells to repair the damaged tissue and also contribute to muscle growth (hypertrophy) in response to exercise.
Cardiac Muscle Tissue
The muscle tissue located in the walls of the heart is cardiac muscle tissue. It consists of branching cells that interconnect in a netlike arrangement. The rhythmic contractions of cardiac muscle are involuntary because they cannot be consciously controlled.
General Characteristics
Location: Found exclusively in the myocardium, the middle and thickest layer of the heart wall.
Function: Responsible for the forceful, rhythmic contractions that pump blood throughout the body.
Control: Involuntary. It possesses its own intrinsic electrical conduction system (autorhythmicity).
Appearance: It is striated, similar to skeletal muscle, due to the organized arrangement of contractile proteins.
Energy Needs: Extremely high metabolic demand, with abundant mitochondria, and relies almost exclusively on aerobic respiration.
Microscopic Organization (Cardiomyocyte)
Cardiac muscle cells, or cardiomyocytes, are highly specialized cells with several unique features.
The Defining Feature: Intercalated Discs
These are complex, specialized junctions that connect adjacent cardiomyocytes end-to-end, appearing as dark, wavy lines. They contain two vital components:
Desmosomes: Act as strong anchoring points, preventing cells from separating during powerful contractions.
Gap Junctions: Channels that allow electrical impulses to pass directly from cell to cell, ensuring the entire heart muscle contracts as a coordinated unit (a functional syncytium).
Other Microscopic Features:
Cell Shape & Nuclei: Cells are shorter, thicker, and branched. Most contain a single, large, centrally located nucleus.
Sarcoplasmic Reticulum (SR): Less extensive than in skeletal muscle. Cardiac muscle relies on both the SR and extracellular calcium to trigger contraction.
Myofibrils & Sarcomeres: Contains organized myofibrils and sarcomeres, which produce the characteristic striations.
Mechanism of Contraction
Cardiac muscle contracts via the sliding filament model, but with key differences in initiation and regulation.
Initiation (Autorhythmicity): Specialized pacemaker cells (e.g., in the SA node) spontaneously generate electrical impulses without nervous input. These impulses spread rapidly through the gap junctions.
Calcium Handling: An initial influx of extracellular Ca²⁺ triggers the release of a larger amount of Ca²⁺ from the sarcoplasmic reticulum (calcium-induced calcium release).
Long Refractory Period: Cardiac muscle has a long period where it cannot be re-stimulated. This is a critical safety feature that prevents tetanic (sustained) contractions, ensuring the heart has time to relax and refill with blood between beats.
Cardiac vs. Skeletal Muscle: Key Differences
Feature
Skeletal Muscle
Cardiac Muscle
Control
Voluntary
Involuntary (autorhythmic)
Cell Shape
Long, cylindrical, unbranched
Shorter, branched
Nuclei
Many, peripheral
One or two, central
Intercalated Discs
Absent
Present (Desmosomes & Gap Junctions)
Ca²⁺ Source
Almost entirely from SR
SR + significant extracellular Ca²⁺
Refractory Period
Short (can tetanus)
Long (prevents tetanus)
Mitochondria
~2% of cell volume
25-35% of cell volume
Smooth Muscle Tissue
Smooth muscle is very distinct from skeletal and cardiac muscle. It is specialized for slow, sustained, involuntary contractions and is found in the walls of hollow internal organs (viscera). It performs many of the involuntary functions essential for life, such as digestion, blood pressure regulation, and elimination.
General Characteristics
Location: Walls of hollow organs like the digestive tract, urinary bladder, reproductive tract, blood vessels, and respiratory airways.
Function: Propulsion of substances (peristalsis), regulation of flow and pressure (vasoconstriction), and expulsion of contents (urination).
Control: Involuntary. Regulated by the autonomic nervous system, hormones, and local chemical changes.
Appearance:Non-striated, as its contractile proteins are not arranged in organized sarcomeres.
Microscopic Organization (Leiomyocyte)
Smooth muscle cells (leiomyocytes) are relatively simple in their morphology but have a sophisticated contractile mechanism.
Key Microscopic Features
Spindle-shaped Cells: Elongated cells, widest in the middle and tapering to pointed ends, each with a single, centrally located nucleus.
No Sarcomeres: Actin and myosin filaments are present but arranged diagonally in a lattice-like network, anchored by dense bodies (analogous to Z-discs).
Calcium Source: The sarcoplasmic reticulum (SR) is much less developed. The majority of Ca²⁺ for contraction comes from the extracellular fluid.
No Troponin: Instead of troponin, smooth muscle uses a protein called Calmodulin to bind Ca²⁺ and initiate contraction.
Types of Smooth Muscle
Smooth muscle is broadly categorized into two types based on its neural and functional characteristics:
1. Single-Unit (Visceral)
The most common type. Cells are electrically coupled by numerous gap junctions and contract rhythmically as a single unit (functional syncytium). Found in the walls of most hollow organs.
2. Multi-Unit
Consists of individual, structurally independent cells with few or no gap junctions. Each cell has its own nerve ending, allowing for fine, precise control. Found in large airways, large arteries, and the iris of the eye.
Smooth vs. Striated Muscle: Key Differences
Feature
Striated Muscle (Skeletal/Cardiac)
Smooth Muscle
Striations
Yes (due to sarcomeres)
No (no sarcomeres)
Control
Voluntary (Skel), Involuntary (Card)
Involuntary
Cell Shape
Long, cylindrical/branched
Spindle-shaped
Troponin
Present (binds Ca²⁺)
Absent (Calmodulin binds Ca²⁺)
Ca²⁺ Source
Primarily SR (Skel), SR + ECF (Card)
Primarily Extracellular Fluid (ECF)
Contraction Speed
Fast, rapid
Slow, prolonged
Fatigue Resistance
Moderate (Skel), High (Card)
Very High
Test Your Knowledge
Check your understanding of the concepts covered in this post.
1. Which type of muscular tissue is characterized by striations, multinucleated cells, and voluntary control?
Smooth muscle
Cardiac muscle
Skeletal muscle
All muscle types
Rationale: Skeletal muscle fibers are long, cylindrical, multinucleated, display prominent striations, and their contraction is under conscious, voluntary control.
2. The ability of muscle tissue to shorten forcibly when adequately stimulated is called:
Excitability
Extensibility
Contractility
Elasticity
Rationale: Contractility is the defining characteristic of muscle tissue, its ability to shorten forcibly and generate tension.
3. Intercalated discs are a unique feature found in which type of muscular tissue?
Skeletal muscle
Smooth muscle
Cardiac muscle
Both skeletal and cardiac muscle
Rationale: Intercalated discs are complex junctions unique to cardiac muscle, containing desmosomes for strength and gap junctions for electrical coupling.
4. Which muscular tissue type is primarily responsible for peristalsis in the digestive tract?
Skeletal muscle
Cardiac muscle
Smooth muscle
Both skeletal and smooth muscle
Rationale: Peristalsis, the wave-like contractions that propel substances through hollow organs like the digestive tract, is a primary function of smooth muscle.
5. What is the primary role of the sarcoplasmic reticulum in muscle contraction?
Generating ATP
Storing calcium ions (Ca2+)
Producing neurotransmitters
Providing elasticity to the muscle fiber
Rationale: The sarcoplasmic reticulum (SR) is a specialized endoplasmic reticulum in muscle cells that stores and releases calcium ions, which are essential for initiating muscle contraction.
6. Which of the following statements about smooth muscle is TRUE?
It has a rapid, powerful contraction.
It contains highly organized sarcomeres.
It is under involuntary control.
It fatigues quickly.
Rationale: Smooth muscle is regulated by the autonomic nervous system, hormones, and local factors, not conscious control.
7. The regulatory protein that binds calcium in skeletal and cardiac muscle is:
Calmodulin
Myosin
Troponin
Actin
Rationale: In skeletal and cardiac muscle, calcium ions bind to troponin, which then causes a conformational change in the troponin-tropomyosin complex, exposing myosin-binding sites on actin.
8. Which type of muscular tissue would you expect to find in the walls of the urinary bladder and blood vessels?
Skeletal muscle
Cardiac muscle
Smooth muscle
Both skeletal and cardiac muscle
Rationale: Smooth muscle forms the walls of most hollow internal organs, including the urinary bladder and blood vessels, where it regulates their diameter and propels contents.
9. What is the function of the T-tubules in skeletal and cardiac muscle?
To store glycogen for energy.
To transmit the action potential deep into the muscle fiber.
To synthesize contractile proteins.
To produce new muscle cells.
Rationale: T-tubules (transverse tubules) are invaginations of the sarcolemma that penetrate deep into the muscle fiber, allowing the action potential to rapidly reach all myofibrils simultaneously.
10. A key difference in the initiation of contraction for smooth muscle compared to skeletal muscle is that smooth muscle uses primarily Ca2+ from:
The sarcoplasmic reticulum only.
Extracellular fluid and binds it to calmodulin.
Intracellular fluid and binds it to troponin.
The synaptic cleft.
Rationale: Unlike skeletal muscle, smooth muscle primarily relies on Ca2+ influx from the extracellular fluid, and this Ca2+ binds to calmodulin (not troponin) to initiate the contraction cascade.
11. The specialized plasma membrane of a muscle cell is called the _____________.
Rationale: "Sarco-" is a prefix often used in muscle terminology, and the sarcolemma is the muscle cell's equivalent of a plasma membrane.
12. The functional unit of contraction in skeletal and cardiac muscle, characterized by a highly organized arrangement of myofilaments, is the _____________.
Rationale: Sarcomeres are the repeating units of actin and myosin filaments, giving striated muscle its characteristic banded appearance and enabling contraction.
13. In cardiac muscle, gap junctions and desmosomes are found within specialized structures called ______________, which allow for rapid electrical communication and strong adhesion between cells.
Rationale: Intercalated discs are crucial for the synchronized, unified contraction of cardiac muscle.
14. The ability of a muscle cell to return to its original length after being stretched or contracted is known as _____________.
Rationale: Elasticity is a key property of muscle tissue, allowing it to snap back to its resting length after being deformed.
15. Smooth muscle cells are typically spindle-shaped and contain a single, centrally located _____________.
Rationale: This describes the basic morphology of a smooth muscle cell, distinguishing it from the multinucleated skeletal muscle or the often branched cardiac muscle cells.
Connective Tissue (CT) is a diverse group of tissues that connect, support, and bind other tissues and organs together. All connective tissues are derived from an embryonic tissue called mesenchyme.
Key Distinguishing Features
Origin: All connective tissues arise from mesenchyme.
Vascularity: Most are well vascularized, with notable exceptions being cartilage (avascular) and dense regular CT (poorly vascularized).
Extracellular Matrix (ECM): This is the defining characteristic. Cells are widely scattered within a large amount of non-living material that they produce. The ECM, consisting of ground substance and protein fibers, is responsible for the tissue's physical properties.
Components of Connective Tissue
All connective tissues share three fundamental components: Ground Substance, Fibers, and Cells.
1. Ground Substance
An unstructured, gel-like material that fills the space between cells and contains the fibers. It is composed of:
Interstitial Fluid: Watery fluid that bathes the cells.
Adhesion Proteins: (e.g., fibronectin, laminin) Act as glue, allowing cells to attach to the matrix.
Proteoglycans: Large molecules that trap water, forming a gel that allows for diffusion of nutrients and waste.
2. Fibers
Fibers provide support and strength to the connective tissue. There are three types:
Collagen Fibers
The strongest and most abundant type. Thick, rope-like bundles that provide high tensile strength (resist pulling forces).
Elastic Fibers
Long, thin, stretchy fibers containing elastin. Allow tissues to stretch and recoil. Found in skin, lungs, and blood vessels.
Reticular Fibers
Short, fine, branched collagenous fibers that form delicate networks (stroma) to support soft organs like the spleen and lymph nodes.
3. Cells of Connective Tissue
Connective tissues contain a variety of resident and migrating cells with distinct roles.
Primary Cell Types
"Blast" Cells (Immature & Active)
Fibroblasts: In CT proper.
Chondroblasts: In cartilage.
Osteoblasts: In bone.
Hematopoietic Stem Cells: In blood.
"Cyte" Cells (Mature & Maintaining)
Fibrocytes: In CT proper.
Chondrocytes: In cartilage.
Osteocytes: In bone.
Other Important Cell Types:
Adipocytes (Fat Cells): Store energy (fat), provide insulation, and cushion organs.
Mast Cells: Initiate local inflammatory responses by releasing histamine. Found near blood vessels.
Macrophages: "Big eaters" that engulf foreign materials and dead cells as part of the immune system.
Plasma Cells: Produce antibodies.
Leukocytes (White Blood Cells): Migrate from the bloodstream to fight infection.
Primary Functions & Main Categories
The diverse composition of connective tissues allows them to perform a wide range of functions, from binding and support to transportation and immune response. They are broadly classified into four main categories.
1. Connective Tissue Proper
Includes Loose CT (e.g., Areolar, Adipose) and Dense CT (e.g., tendons, dermis of the skin).
2. Cartilage
Strong and flexible tissue that provides support and shock absorption. Includes Hyaline, Elastic, and Fibrocartilage.
3. Bone Tissue
Hard connective tissue that forms the skeleton, with a calcified matrix.
4. Blood
A fluid connective tissue where the extracellular matrix is the liquid plasma.
Connective Tissue Proper
This is the most diverse group of connective tissues. It is divided into two main categories: Loose Connective Tissues, which have more ground substance and fewer fibers, and Dense Connective Tissues, which have more fibers and less ground substance.
A. Loose (Areolar) Connective Tissues
Loose Areolar Connective Tissue
Features a loose, gel-like matrix with all three fiber types (collagen, elastic, reticular) and various cells, including fibroblasts, macrophages, and mast cells.
Histology Hint:
Look for a sparse, web-like appearance with randomly arranged thick pink (collagen) and thin black/purple (elastic) fibers, plus many scattered black dots (cell nuclei).
Function: Wraps and cushions organs, holds tissue fluid, plays a key role in inflammation.
Location: Widely distributed under epithelia; forms the lamina propria of mucous membranes.
Adipose Tissue (Fat)
Primarily composed of large, tightly packed adipocytes (fat cells) with very little matrix. It is highly vascularized.
Histology Hint:
Characterized by large, empty-looking circular cells (adipocytes), as the fat droplet is typically dissolved during processing. Nuclei are flattened and pushed to the periphery.
Function: Energy storage, insulation, and organ protection/cushioning.
Location: Under the skin (hypodermis), around kidneys and eyeballs, in the abdomen and breasts.
Reticular Connective Tissue
A network of fine reticular fibers in a loose ground substance, with reticular cells (specialized fibroblasts) as the main cell type.
Histology Hint:
Look for a fine, branching network of dark-staining reticular fibers forming a delicate meshwork (stroma), typically filled with numerous small, round cells (like lymphocytes in a lymph node).
Function: Forms a soft internal skeleton (stroma) that supports other cell types in lymphoid organs.
Location: Lymphoid organs (lymph nodes, spleen, bone marrow).
B. Dense (Fibrous) Connective Tissues
Dense Regular Connective Tissue
Densely packed, primarily parallel collagen fibers with fibroblasts as the major cell type. It is poorly vascularized.
Histology Hint:
Characterized by dense, wavy, parallel bundles of pink collagen fibers running in a single direction, with fibroblast nuclei squeezed and flattened between them.
Function: Attaches muscles to bones (tendons) or bones to bones (ligaments). Provides great tensile strength in one direction.
Location: Tendons, most ligaments, aponeuroses.
Dense Irregular Connective Tissue
Primarily irregularly arranged, thick collagen fibers with some elastic fibers and fibroblasts.
Histology Hint:
Shows thick bundles of pink collagen fibers running in many different directions, creating a chaotic appearance.
Function: Withstands tension exerted in many directions, providing structural strength.
Location: Dermis of the skin, fibrous capsules of organs and joints.
Elastic Connective Tissue
A type of dense regular connective tissue with a high proportion of elastic fibers.
Histology Hint:
Displays prominent, wavy, dark-staining elastic fibers arranged in parallel, often with a background of lighter pink collagen.
Function: Allows tissue to recoil after stretching; maintains pulsatile blood flow and aids passive recoil of lungs.
Location: Walls of large arteries, certain ligaments of the vertebral column, walls of bronchial tubes.
Cartilage
Cartilage is a tough, flexible connective tissue that consists of a firm, gelatinous matrix in which cartilage cells, or chondrocytes, are embedded within fluid-filled spaces called lacunae. It is avascular (lacks blood vessels) and lacks nerves, relying on diffusion for nutrients.
Key Characteristics:
Cells:Chondroblasts produce the matrix, which mature into chondrocytes that maintain it from within their lacunae.
Matrix: A firm, gel-like ground substance rich in water, proteoglycans, and fibers.
Perichondrium: Most cartilages are surrounded by a dense irregular connective tissue membrane that provides nutrients.
Types of Cartilage
1. Hyaline Cartilage
The most abundant type, with a smooth, glassy, bluish-white appearance. It provides a protective covering on bone surfaces, forms the larynx, connects ribs to the sternum, and supports air passages.
Histology Details:
What is in between the lacunae? A firm, glassy matrix of water, proteoglycans, and very fine collagen fibers (not usually visible).
How far apart are the lacunae? Moderately spaced, allowing for an even distribution of chondrocytes.
Function: Supports and reinforces, provides resilient cushioning, and resists compressive stress.
Location: Articular cartilages of joints, costal cartilages of ribs, cartilages of the nose, trachea, and larynx.
2. Elastic Cartilage
Similar to hyaline cartilage, but contains an abundance of visible elastic fibers that provide greater elasticity and flexibility.
Histology Details:
What is in between the lacunae? A matrix containing visible, dark-staining elastic fibers in addition to collagen and proteoglycans.
How far apart are the lacunae? Moderately spaced, similar to hyaline, but the elastic fibers give it a more flexible appearance.
Function: Maintains the shape of a structure while allowing great flexibility.
Location: External ear (pinna), epiglottis.
3. Fibrocartilage
The matrix contains many tightly packed, thick collagen fibers that lie between short rows of chondrocytes. It is especially tough and able to absorb significant shocks and pressure.
Histology Details:
What is in between the lacunae? A matrix dominated by thick, often parallel bundles of collagen fibers, with less ground substance.
How far apart are the lacunae? Chondrocytes are often arranged in rows between the thick fiber bundles, making them more sparsely distributed than in other cartilage types.
Function: High tensile strength with the ability to absorb compressive shock.
Location: Intervertebral discs, pubic symphysis, menisci of the knee joint.
Bone (Osseous Tissue)
Of all the supportive connective tissues, bone is the hardest and most rigid. This results from its unique matrix, which is composed of inorganic calcium salts (for hardness) and organic collagen fibers (for flexibility). It is well vascularized and contains specialized cells: osteoblasts (which form the matrix) and osteocytes (which maintain it from within lacunae).
Compact Bone (The "Hard Outer Shell")
This is the dense, solid outer layer of almost all bones, built for strength and protection. It is organized into repeating, cylindrical units called osteons (Haversian systems).
Analogy: Think of a bundle of straws packed tightly together. Each straw is an osteon.
Spongy Bone (The "Porous Inner Core")
This is the lighter, porous inner layer of most bones, made of a network of needle-like pieces called trabeculae. The spaces between trabeculae are filled with red bone marrow, where blood cells are produced.
Analogy: Think of a honeycomb. It has many interconnected spaces but is still structurally sound.
Blood
Blood is the only fluid connective tissue. It consists of blood cells (formed elements) suspended in a fluid matrix called plasma.
Primary Functions:
Transportation: Delivers oxygen, nutrients, and hormones; carries away waste products.
Regulation: Helps maintain body temperature, pH, and fluid volume.
Protection: Prevents blood loss through clotting and prevents infection with antibodies and white blood cells.
1. Plasma (The Extracellular Matrix)
The non-living, straw-colored fluid matrix that makes up about 55% of total blood volume. It is ~90% water and contains numerous solutes.
Other Solutes: Nutrients, electrolytes, respiratory gases, hormones, and waste products.
2. Formed Elements (The Cells)
The living cellular components suspended in plasma, making up about 45% of total blood volume. All are formed in the bone marrow.
a. Erythrocytes (Red Blood Cells - RBCs)
Anucleated, biconcave discs filled with hemoglobin. Their primary function is oxygen transport.
b. Leukocytes (White Blood Cells - WBCs)
Complete cells crucial for immunity and defense. Includes Neutrophils, Lymphocytes, Monocytes, Eosinophils, and Basophils.
c. Thrombocytes (Platelets)
Cytoplasmic fragments, not true cells. Essential for blood clotting (hemostasis).
Test Your Knowledge
Check your understanding of the concepts covered in this post.
1. Which of the following is a primary characteristic of all connective tissues?
Cells are tightly packed with little extracellular material.
It is always avascular.
It contains a significant amount of extracellular matrix.
Its primary function is protection from abrasion.
Rationale: This is the hallmark characteristic distinguishing connective tissue from other tissue types. The extracellular matrix (ECM) is typically abundant and determines the tissue's specific functions.
2. The major components of the extracellular matrix in connective tissue are:
Cells and ground substance.
Ground substance and protein fibers.
Protein fibers and specialized cells.
Blood vessels and nerve endings.
Rationale: The extracellular matrix is defined as the non-living material produced by the cells themselves, consisting of ground substance (the unstructured material) and protein fibers (collagen, elastic, reticular).
3. Which cell type is primarily responsible for producing the fibers and ground substance in most connective tissues?
Macrophages
Adipocytes
Fibroblasts
Chondrocytes
Rationale: Fibroblasts are the most common fixed cells in most connective tissues, actively synthesizing and secreting the protein fibers and components of the ground substance.
4. All of the following are types of protein fibers found in connective tissue EXCEPT:
Collagen fibers
Elastic fibers
Reticular fibers
Myosin fibers
Rationale: Myosin is a contractile protein found in muscle cells, not an extracellular fiber in connective tissue. Collagen, elastic, and reticular are the three main types of protein fibers in the ECM.
5. Which type of fiber provides great tensile strength, allowing tissue to resist stretching and pulling, and is the most abundant protein in the body?
Elastic fibers
Collagen fibers
Reticular fibers
Actin fibers
Rationale: Collagen is known for its incredible tensile strength and is the most abundant protein in the human body, providing structural integrity.
6. The "ground substance" of connective tissue primarily consists of:
Water, ions, and lipids.
Interstitial fluid, cell adhesion proteins, and proteoglycans.
Collagen and elastic fibers.
Blood plasma and platelets.
Rationale: The ground substance is the shapeless material that fills the space between cells and fibers, consisting primarily of interstitial fluid, cell adhesion proteins (to anchor cells to fibers), and large polysaccharides and proteoglycans that give it its gel-like consistency and trap water.
7. Which type of connective tissue cell is responsible for storing fat and providing insulation?
Mast cells
Macrophages
Adipocytes
Lymphocytes
Rationale: Adipocytes are specialized fat cells that store triglycerides, serving as energy reserves, insulation, and cushioning.
8. A rich blood supply, or vascularity, is a general feature of most connective tissues, with the notable exception of:
Areolar connective tissue
Dense regular connective tissue
Adipose tissue
Cartilage
Rationale: Cartilage is unique among most connective tissues for being avascular (lacking a direct blood supply). It receives nutrients via diffusion from surrounding perichondrium or synovial fluid.
9. What is the primary function of mast cells in connective tissue?
Phagocytosis of foreign invaders.
Production of antibodies.
Initiation of the inflammatory response.
Storage of energy reserves.
Rationale: Mast cells detect foreign substances and initiate local inflammatory responses by releasing histamine and other chemicals that cause vasodilation and increased permeability.
10. Which statement best describes the general organization of connective tissue?
Cells are closely opposed and form continuous sheets.
It always forms the lining of cavities and surfaces.
Cells are often widely scattered within an abundant extracellular matrix.
It is primarily composed of contractile proteins.
Rationale: This fundamental characteristic sets connective tissue apart from epithelial tissue (where cells are tightly packed). The spacing of cells within a substantial ECM allows for diverse functions.
11. The protein fiber that allows for stretch and recoil in connective tissue is the ___________ fiber.
Rationale: Elastic fibers are composed of elastin, allowing them to stretch and then snap back to their original length, providing elasticity to tissues.
12. The jelly-like or fluid material that fills the space between cells and fibers in connective tissue is called the _____________.
Rationale: Ground substance is the amorphous component of the extracellular matrix, serving as a medium through which nutrients and waste can diffuse.
13. The most common fixed cell type in general connective tissue proper is the _____________, which synthesizes fibers and ground substance.
Rationale: Fibroblasts are the primary "builders" of connective tissue, responsible for creating its extracellular components.
14. _______________ are large, irregular cells in connective tissue that are specialized for phagocytosis to engulf foreign particles and cellular debris.
Rationale: Macrophages are critical immune cells in connective tissue, acting as professional phagocytes.
15. Unlike epithelial tissue, connective tissue is typically rich in _____________, allowing for efficient nutrient and waste exchange.
Rationale: Most connective tissues have a good blood supply, which provides oxygen and nutrients to the cells and removes waste products.
Epithelium forms continuous sheets of cells that line internal surfaces and cover the external surface of the body. It acts as a selective barrier that protects tissues and is often involved in absorption or secretion. A non-cellular layer called the basement membrane separates an epithelium from the underlying connective tissue.
Key Characteristics:
Anchorage & Polarity
Cells are anchored to a basement membrane and have an apical surface (facing a free space) and a basal surface (attached to the basement membrane).
Avascularity & Cellularity
Epithelium contains no blood vessels (avascular) and is composed almost entirely of tightly packed cells with very little extracellular matrix (cellularity).
Origin of the Epithelial Tissues
Epithelial tissues are diverse in function and location, which is reflected in their origins from all three primary germ layers formed during embryonic development. These are the primary layers of cells from which all tissues and organs of the body are derived.
Ectoderm (Outermost layer)
Gives rise to structures that interact with the outside world and the nervous system.
Epithelial Derivatives:
Epidermis of the skin
Lining of the oral & nasal cavities
Lining of the anal canal
Glands derived from skin
Mesoderm (Middle layer)
Forms structures related to movement, support, and circulation.
Epithelial Derivatives:
Endothelium (lining blood vessels)
Mesothelium (lining serous cavities)
Epithelium of kidney tubules
Epithelium of the gonads
Endoderm (Innermost layer)
Forms the lining of the digestive and respiratory systems and associated glands.
Epithelial Derivatives:
Lining of the GI tract
Lining of the respiratory tract
Lining of the urinary bladder
Epithelium of thyroid, pancreas, liver
The Basement Membrane
The basement membrane (BM) is a thin, acellular, extracellular layer that underlies all epithelial tissues, separating them from the adjacent connective tissue. It is a critical structural and functional component.
Composition & Structure
The BM is primarily composed of glycoproteins (like laminin), proteoglycans, and various types of collagen (especially Type IV collagen). Under an electron microscope, it is seen to have two main layers:
Basal Lamina: Produced by the epithelial cells. It has a clearer layer (lamina lucida) and a denser layer (lamina densa).
Reticular Lamina: Produced by the underlying connective tissue. It is composed of reticular fibers (Type III collagen) that anchor the basal lamina.
Functions of the Basement Membrane
Structural Support: Provides a stable base for epithelial cells.
Filtration Barrier: Regulates passage of molecules (e.g., in the kidney).
Cell Adhesion: Mediates strong attachment of epithelium.
Maintains Polarity: Helps define the apical-basal orientation.
Regulates Cell Behavior: Influences growth and differentiation.
Tissue Repair: Acts as a scaffold for regeneration.
Summary of Key Characteristics
Anchored to basement membrane
Apical and Basal surfaces (Polarity)
No extracellular matrix (Cellularity)
Avascular (no blood vessels)
Clinical Correlation: Invasion and Cancer
The basement membrane is a critical marker in cancer diagnosis. Benign tumors remain confined above the BM. A hallmark of malignant tumors (cancer) is their ability to produce enzymes that degrade the BM, allowing them to invade the underlying connective tissue and metastasize (spread).
Classification of Epithelium
Epithelium is classified based on two main features: the number of cell layers and the shape of the cells at the apical (free) surface.
Simple Squamous
Function: Ideal for diffusion and filtration. | Location: Alveoli of the lungs, lining of blood vessels (endothelium).
Simple Cuboidal
Function: Secretion and absorption. | Location: Kidney tubules, glands.
Simple Columnar
Function: Absorption and secretion. | Location: Gastrointestinal tract.
Stratified Squamous
Function: Protection against abrasion.
Keratinized: Surface cells are dead and filled with keratin. (Location: Epidermis of the skin).
Non-keratinized: Surface cells are living. (Location: Esophagus, vagina).
Transitional (Urinary) Epithelium
Function: Allows for distension (stretching). | Location: Urinary bladder, ureters.
Function: Secretion and movement of mucus. | Location: Trachea, bronchi.
Simple squamous epithelium
Simple squamous epithelium is a single layer of thin, flattened cells that forms a delicate lining in areas where rapid diffusion, filtration, or smooth movement of substances is needed. The extreme thinness of the cells provides minimal protection but allows for quick transport of molecules.
Classification & Defining Characteristics
Simple
Consists of a single layer of cells, crucial for rapid transport across the membrane.
Squamous
Cells are flat, thin, and scale-like ("squashed"), resembling a tiled floor from the surface.
Permeable
The extreme thinness of the single layer makes it highly permeable for quick exchange.
Structure & Appearance
Cell Shape: Irregularly shaped, flattened cells that interlock like puzzle pieces.
Nucleus: Oval or flattened, often appearing as a central bulge in the thin cell.
Cytoplasm: Scanty (very little), reflecting its primary role in passive transport.
Basement Membrane: Rests on a thin basement membrane, separating it from underlying connective tissue.
Locations and Functions
Simple squamous epithelium is strategically located in areas where rapid diffusion, filtration, or a slick, friction-reducing surface is required.
Lining of Blood & Lymphatic Vessels (Endothelium)
Provides a smooth, clot-preventing surface for blood flow and facilitates the exchange of gases, nutrients, and waste.
Lining of Serous Cavities (Mesothelium)
Lines the pleura, pericardium, and peritoneum, producing a slippery serous fluid that lubricates organs and prevents friction.
Alveoli of the Lungs (Type I Pneumocytes)
Forms the extremely thin "air-blood barrier" essential for rapid gas exchange (oxygen in, carbon dioxide out).
Glomerular Capsules (Bowman's Capsule) in the Kidneys
Forms the filtration membrane for blood, allowing water and small solutes to pass into the renal tubule while retaining large molecules.
Clinical Significance
Understanding the structure of simple squamous epithelium is key to diagnosing and managing several clinical conditions.
Pathological Considerations
Edema: Fluid accumulation (e.g., in heart failure) increases the diffusion distance across the alveolar epithelium, impairing gas exchange.
Inflammation: Inflammation of serous membranes (pleuritis, peritonitis) causes fluid accumulation (effusions) and painful friction.
Cancer: Malignant mesotheliomas can arise from the mesothelium, and a disrupted endothelium is a key factor in various vascular diseases.
Simple cuboidal epithelium
Simple cuboidal epithelium is a single layer of cube-shaped cells, often with round, central nuclei, primarily performing secretion and absorption. It is found lining surfaces like kidney tubules, ducts of glands, and the surface of the ovary, where it plays a vital role in regulating substances and producing secretions.
Classification & Defining Characteristics
Simple
Consists of a single layer of cells, allowing for controlled secretion and absorption.
Cuboidal
Cells are cube-like in shape, with a height and width that are approximately equal in cross-section.
Central Nucleus
The nucleus is spherical and centrally located, a key identifying feature.
Structure & Appearance
Overall Shape: Forms a single layer of cells that often line a duct or tubule, encircling a central lumen (open space).
Cytoplasm: Contains more cytoplasm and organelles than squamous cells, reflecting its active role in secretion and absorption.
Specializations: The apical surface may have microvilli (a "brush border") to increase surface area, especially in the kidney tubules.
Locations and Functions
Simple cuboidal epithelium is found in locations primarily involved in secretion, absorption, and transport.
1. Kidney Tubules
Highly active in the absorption of water and nutrients from filtrate back into the blood, and secretion of waste products into the filtrate.
2. Small Ducts of Glands
Found in salivary glands, pancreas, and liver. Also forms the follicles of the thyroid gland, where it synthesizes and secretes thyroid hormones.
3. Ovary Surface (Germinal Epithelium)
Provides a protective covering for the surface of the ovary.
4. Choroid Plexus of the Brain
Specialized cuboidal cells that produce cerebrospinal fluid (CSF).
Clinical Significance
Dysfunction of simple cuboidal epithelium is linked to several significant diseases.
Pathological Considerations
Polycystic Kidney Disease (PKD): A genetic disorder where cysts lined by abnormal cuboidal cells form in the kidneys, leading to kidney failure.
Glandular Dysfunction: Thyroid disorders often involve altered function of the simple cuboidal cells that form the secretory follicles.
Carcinomas: Cancers originating from glandular tissue (adenocarcinomas), such as renal cell carcinoma, arise from these epithelial cells.
Simple columnar epithelium
Simple columnar epithelium is a single layer of tall, column-shaped cells lining organs like the stomach and intestines. These cells are highly specialized for absorption and secretion, featuring nuclei located near the basement membrane and often possessing apical specializations like microvilli or cilia.
Classification & Defining Characteristics
Simple: A single layer of cells, maximizing efficiency for absorption and secretion.
Columnar: The cells are distinctly taller than they are wide, providing ample cytoplasmic volume for metabolic machinery.
Basal Nucleus: The nucleus is typically oval-shaped and located basally (closer to the basement membrane), a key diagnostic feature.
Key Specializations
This is where simple columnar epithelium truly excels, often having specialized apical modifications to enhance its functions:
Microvilli (Brush Border)
Minute, finger-like projections that vastly increase surface area for absorption. Found in the small intestine.
Cilia
Longer, motile projections that propel substances along the surface. Found in uterine (fallopian) tubes.
Goblet Cells
Specialized unicellular glands that secrete mucus for lubrication and protection. Abundant in the GI tract.
Locations and Functions
Simple columnar epithelium is found in areas demanding high levels of absorption, secretion, and sometimes transport.
Gastrointestinal Tract (Stomach to Rectum)
In the stomach, it secretes mucus and enzymes. In the small intestine, it is the primary site for nutrient absorption, enhanced by microvilli. In the large intestine, it absorbs water and secretes mucus.
Gallbladder
Primarily for water absorption to concentrate bile. Contains microvilli but no goblet cells.
Uterine (Fallopian) Tubes
Contains ciliated columnar cells that help propel the ovum towards the uterus.
Clinical Significance
Damage or changes to simple columnar epithelium are central to many significant diseases, particularly in the gastrointestinal tract.
Pathological Considerations
Malabsorption Syndromes: In Celiac Disease, damage to the intestinal columnar epithelium flattens microvilli, drastically reducing nutrient absorption.
Metaplasia (Barrett's Esophagus): Chronic acid reflux can cause the esophageal lining to change into a columnar type, a precancerous condition.
Adenocarcinomas: Cancers arising from glandular tissue, like colorectal cancer, originate from simple columnar epithelium.
Cystic Fibrosis: Affects mucus-secreting goblet cells, producing abnormally thick mucus that impairs clearance in the respiratory tract and blocks ducts.
Stratified squamous epithelium
Stratified squamous epithelium is a protective tissue composed of multiple layers of cells, with flattened, scale-like cells at the surface. Its primary function is to provide a physical barrier against abrasion, microorganisms, and water loss. It is the most common type of stratified epithelium in the body.
Classification & Defining Characteristics
Stratified: Consists of multiple layers of cells, providing robust protection.
Squamous: The cells in the most superficial (apical) layer are flat and scale-like. The classification name is always based on this top layer.
Basal Layer: The deepest (basal) layer consists of cuboidal or columnar cells that are actively mitotic, constantly producing new cells that are pushed towards the surface.
Layers and Structure
The tissue is organized into distinct layers, from the actively dividing basal layer to the flattened superficial layer.
Basal Layer (Stratum Basale): A single layer of cuboidal/columnar stem cells resting on the basement membrane.
Intermediate Layers: Cells become more polyhedral and then progressively flatter as they are pushed upwards. They are strongly connected by numerous desmosomes.
Superficial Layer: Composed of flattened, squamous cells, which are eventually shed from the surface.
The Two Main Subtypes
Stratified squamous epithelium is further divided based on the presence or absence of a key protein—keratin—in its superficial layers.
A. Keratinized Stratified Squamous
The most superficial layers are composed of dead cells filled with keratin, a tough, water-resistant protein. These cells lack nuclei.
Key Features & Locations:
Appearance: Dry, flaky surface.
Function: Waterproofing, protection from abrasion and pathogens.
Location: Epidermis of the skin.
B. Non-Keratinized Stratified Squamous
The superficial cells do not contain significant keratin and remain alive, retaining their nuclei.
Key Features & Locations:
Appearance: Moist surface.
Function: Protection against abrasion in moist areas.
As a primary protective barrier, this epithelium is central to many disease processes and clinical assessments.
Pathological Considerations
Psoriasis: Hyperproliferation and abnormal keratinization of the epidermis, leading to thick, scaly plaques.
Cancer: A high percentage of human cancers (e.g., squamous cell carcinoma of the skin, mouth, cervix) originate from this tissue. A Pap smear checks for precancerous changes in the cervical epithelium.
Leukoplakia: A precancerous condition involving the thickening of non-keratinized epithelium (e.g., in the mouth) due to chronic irritation like tobacco use.
Transitional epithelium
Transitional epithelium, also known as urothelium, is a specialized, multi-layered type of stratified epithelium found exclusively in the urinary system. Its most remarkable feature is its ability to stretch and recoil, allowing organs like the bladder to expand significantly without losing structural integrity or allowing the toxic components of urine to leak into underlying tissues.
Classification & Defining Characteristics
While stratified, its key feature is its ability to change shape, or "transition," based on the degree of stretch.
Relaxed / Contracted State
Appears to have 4-6+ layers. The most superficial (apical) cells are large, dome-shaped, and often bi-nucleated. These are known as "umbrella cells."
Distended / Stretched State
The entire epithelial layer thins to just 2-3 layers. The umbrella cells flatten out, becoming more squamous-like in appearance to accommodate the increased volume.
Umbrella Cells & Impermeability
The large, outermost umbrella cells are highly specialized. They have a thickened apical plasma membrane, sometimes called a "crust," formed by specialized proteins called uroplakins. This unique feature makes the epithelium impermeable, forming a crucial barrier that protects the underlying cells from the hypertonic and toxic effects of urine.
Locations and Functions
Transitional epithelium is exclusively found lining the hollow organs of the urinary tract:
Renal Pelvis
Ureters
Urinary Bladder
Proximal part of the Urethra
Clinical Significance
As the primary lining of the urinary tract, urothelium is central to many common and serious urological conditions.
Pathological Considerations
Bladder Cancer (Urothelial Carcinoma): The vast majority of cancers of the bladder, ureters, and renal pelvis originate from this tissue. Smoking is a major risk factor.
Urinary Tract Infections (UTIs): Pathogens like E. coli can adhere to and invade urothelial cells, leading to infections.
Cystitis: Inflammation of the bladder lining due to infection or irritation, leading to symptoms like pain, urgency, and frequency.
Pseudostratified columnar epithelium
Pseudostratified columnar epithelium is a single layer of cells that appears multi-layered because the nuclei are at different heights, though all cells are anchored to the basement membrane. It is found in areas like the trachea and upper respiratory tract, where it often bears cilia to move mucus.
Classification & Defining Characteristics
Pseudostratified: The key feature. It appears stratified because its nuclei are at different levels, but it is a single layer as all cells touch the basement membrane.
Columnar: The cells that reach the apical surface are tall and column-shaped.
Ciliated: The surface cells typically possess numerous motile, hair-like cilia.
Goblet Cells: Almost always contains numerous interspersed goblet cells that secrete mucus.
Structure & Cell Types
This "crowded" arrangement gives the illusion of stratification and contains three main cell types:
Columnar Ciliated Cells
Tall cells that reach the surface and bear the motile cilia.
Goblet Cells
Mucus-secreting unicellular glands interspersed among the other cells.
Basal Cells
Small stem cells that sit on the basement membrane and regenerate the other cell types.
Locations and Functions
This highly specialized epithelium is almost exclusively found in the respiratory tract, where it performs its vital role in the "mucociliary escalator."
The Mucociliary Escalator
This is its most famous function. Goblet cells produce a sticky layer of mucus that traps inhaled dust, pollen, and pathogens. The cilia then beat in a coordinated rhythm, sweeping the mucus upwards towards the pharynx, where it can be swallowed or expelled. This prevents foreign substances from reaching the delicate lung tissue.
Key Locations:
Nasal Cavity, Paranasal Sinuses, Nasopharynx
Trachea and Bronchi (large and medium-sized)
Exception: In the Epididymis, it has immotile stereocilia and functions in absorption for sperm maturation.
Clinical Significance
As the first line of defense against airborne pathogens, dysfunction of this epithelium has severe consequences for respiratory health.
Pathological Considerations
Smoking: Chronic smoking paralyzes and destroys cilia, compromising the mucociliary escalator and leading to mucus buildup, chronic bronchitis, and increased infection risk.
Squamous Metaplasia: Due to chronic irritation (like smoking), this tissue can change into stratified squamous epithelium. While more protective, it lacks cilia and goblet cells, losing the vital escalator function and increasing the risk of cancer.
Cystic Fibrosis: A genetic disease causing abnormally thick mucus that impairs ciliary function, clogs airways, and leads to chronic respiratory infections.
Kartagener Syndrome (PCD): A genetic disorder causing defective, immotile cilia, leading to chronic respiratory infections and male infertility.
Glandular Epithelium
Glandular epithelium is a specialized tissue composed of cells whose primary function is secretion. These cells are highly specialized to synthesize, store, and release substances such as hormones, mucus, enzymes, and sweat. All glands in the body develop from ingrowths of epithelial sheets into the underlying connective tissue.
Classification of Glands
Glands are primarily classified based on where they release their secretions:
A. Exocrine Glands (External Secretion)
Secrete their products onto an epithelial surface, either directly or through a duct.
Examples:
Sweat glands
Salivary glands
Pancreas (exocrine portion)
Mammary glands
Sebaceous (oil) glands
B. Endocrine Glands (Internal Secretion)
Secrete their products (hormones) directly into the bloodstream. They are ductless.
Examples:
Thyroid gland
Adrenal glands
Pituitary gland
Pancreas (endocrine islets)
Ovaries & Testes
Modes of Exocrine Secretion
Exocrine glands release their products in three different ways:
Merocrine (Eccrine)
Secretion via exocytosis with no loss of cytoplasm. (Most common)
Apocrine
A portion of the apical cytoplasm pinches off with the secretion.
Holocrine
The entire cell ruptures to release its contents, leading to cell death.
Types of Secretion
Serous: A watery fluid, often rich in enzymes (e.g., parotid salivary gland).
Mucous: A viscous, sticky fluid (mucus) for lubrication and protection (e.g., goblet cells).
Mixed: Produce both serous and mucous secretions (e.g., submandibular salivary gland).
Clinical Significance
The health and function of glandular epithelium are central to many physiological processes and disease states.
Pathological Considerations
Glandular Dysfunction: Many diseases involve hypo- or hyperfunction. Exocrine examples include Cystic Fibrosis (abnormal mucus). Endocrine examples include Diabetes (pancreas) and Thyroid disorders.
Tumors/Cancers: Many cancers originate from glandular epithelium. Benign tumors are called adenomas, and malignant cancers are called adenocarcinomas (e.g., breast, colon, prostate cancer).
Inflammation (Adenitis): Inflammation of glands, such as sialadenitis (salivary glands) or mastitis (mammary glands).
Test Your Knowledge
Check your understanding of the concepts covered in this post.
1. Which of the following is a general characteristic of epithelial tissue?
Contains abundant extracellular matrix.
Always highly vascularized.
Cells are closely packed with little intercellular space.
Primarily specialized for contraction.
Rationale: Epithelial tissues are characterized by tightly packed cells, forming continuous sheets, with very little extracellular material between them. This close packing is crucial for their barrier and protective functions.
2. Where would you most likely find simple squamous epithelium?
Lining the stomach and intestines.
Forming the outer layer of the skin.
Lining blood vessels (endothelium) and lung alveoli.
In the ducts of large glands.
Rationale: Simple squamous epithelium is very thin and flat, allowing for rapid diffusion and filtration. This makes it ideal for lining surfaces where exchange of substances occurs, such as in the capillaries (blood vessels) and air sacs of the lungs (alveoli).
3. A tissue consisting of multiple layers of cells, with the top layer being flat and squamous, would be classified as:
Simple cuboidal epithelium.
Stratified columnar epithelium.
Pseudostratified columnar epithelium.
Stratified squamous epithelium.
Rationale: "Stratified" indicates multiple layers, and "squamous" describes the flat shape of the cells at the surface. This type of epithelium is adapted for protection against abrasion, found in the skin and lining of the mouth.
4. Which type of epithelium is characterized by a single layer of cells of varying heights, all attached to the basement membrane, but not all reaching the free surface, often possessing cilia and goblet cells?
Simple columnar epithelium.
Stratified cuboidal epithelium.
Pseudostratified columnar epithelium.
Transitional epithelium.
Rationale: This description perfectly matches pseudostratified columnar epithelium, commonly found lining the trachea and upper respiratory tract, where cilia help move mucus. Its nuclei appear at different levels, giving a false impression of multiple layers.
5. Glands that secrete their products directly into the bloodstream (ductless glands) are classified as:
Exocrine glands.
Endocrine glands.
Merocrine glands.
Apocrine glands.
Rationale: Endocrine glands are ductless and release hormones directly into the interstitial fluid, which then diffuses into the bloodstream. Exocrine glands, in contrast, secrete products onto a surface or into a lumen via ducts.
6. Which statement correctly describes transitional epithelium?
It is found in the lining of the stomach and secretes digestive enzymes.
It allows for stretching and distension, found in the urinary bladder.
It is a single layer of tall, narrow cells with microvilli, found in the intestines.
It forms the protective outer layer of the skin.
Rationale: Transitional epithelium is a specialized stratified epithelium found exclusively in the urinary tract. Its cells have the unique ability to change shape, allowing the bladder and ureters to stretch and recoil without tearing.
7. A gland that releases its secretory product by exocytosis, without any loss of glandular cell cytoplasm, is classified as a:
Holocrine gland.
Apocrine gland.
Merocrine gland.
Sebaceous gland.
Rationale: Merocrine secretion is the most common mode, where products are released by exocytosis from vesicles, with the cell remaining intact. Examples include salivary glands and most sweat glands.
8. Goblet cells are unicellular glands commonly found within which type of epithelium, where they secrete mucus?
Stratified squamous epithelium.
Simple cuboidal epithelium.
Pseudostratified and simple columnar epithelium.
Simple squamous epithelium.
Rationale: Goblet cells are specialized mucus-secreting cells commonly interspersed within the columnar epithelial lining of the respiratory (pseudostratified) and digestive (simple columnar) tracts.
9. Which type of epithelial tissue is best adapted for absorption and secretion, often featuring microvilli on its apical surface?
Simple squamous epithelium.
Simple cuboidal epithelium.
Simple columnar epithelium.
Stratified cuboidal epithelium.
Rationale: Simple columnar epithelium, with its taller cells, provides more cytoplasmic volume for processing absorbed substances and synthesizing secretory products. Microvilli increase the surface area for absorption, as seen in the intestines.
10. A gland whose entire cell ruptures to release its secretory product (along with dead cell fragments) is a:
Merocrine gland.
Apocrine gland.
Holocrine gland.
Endocrine gland.
Rationale: Holocrine secretion involves the accumulation of secretory products within the cell, followed by the entire cell rupturing and becoming part of the secretion. Sebaceous glands are a classic example.
11. All epithelial tissues are attached to an underlying connective tissue layer by a non-cellular layer called the ________________.
Rationale: The basement membrane is a crucial anchoring structure that separates epithelial tissue from the underlying connective tissue, providing structural support and regulating substance passage.
12. Epithelial tissue is described as ________________ because it lacks direct blood vessels and receives nutrients by diffusion.
Rationale: Avascular means "without blood vessels." Epithelial tissues rely on diffusion from the underlying connective tissue for their nutrient supply and waste removal.
13. The type of epithelial tissue that forms the epidermis of the skin, providing protection against abrasion, is ________________ squamous epithelium.
Rationale: The outer layer of the skin (epidermis) is composed of multiple layers of flattened cells, indicating stratified squamous epithelium, specialized for protection.
14. Glands that secrete their products into ducts, which then carry the secretions to an epithelial surface, are known as ________________ glands.
Rationale: Exocrine glands are defined by their use of ducts to deliver their secretions (e.g., sweat, saliva, digestive enzymes) to specific locations.
15. The kidney tubules are typically lined by a single layer of cube-shaped cells, making this tissue type ________________ cuboidal epithelium.
Rationale: Simple cuboidal epithelium, with its single layer of cube-shaped cells, is well-suited for secretion and absorption functions found in structures like kidney tubules and small gland ducts.