The Menstrual Cycle
The menstrual cycle is a monthly series of natural changes in hormone production and the structures of the uterus and ovaries. It is a complex, highly coordinated process that prepares the female body for the possibility of pregnancy.
Averaging around 28 days (though a normal range is strictly defined as 21 to 35 days), the cycle is designed to produce and release an egg (ovulation) and prepare the uterus for potential implantation. If pregnancy does not occur, the uterine lining is shed, resulting in menstruation.
1. Key Organs & Hormones Involved (The HPO Axis)
The entire cycle is a masterful conversation between the brain and the reproductive organs, regulated by a precise cascade of hormones known as the Hypothalamic-Pituitary-Ovarian (HPO) Axis.
Releases Gonadotropin-Releasing Hormone (GnRH) to start the cascade.
Deep Detail: GnRH must be released in a strictly pulsatile manner (every 60-90 minutes). Continuous release of GnRH actually shuts down the entire system via receptor downregulation.
Releases FSH (Follicle-Stimulating Hormone) & LH (Luteinizing Hormone) to stimulate the ovaries in response to GnRH.
Mature the eggs and act as the primary endocrine factories, producing Estrogen (specifically Estradiol, E2), Progesterone, and Inhibins.
The target organ. Its inner lining (the endometrium) thickens and sheds in direct response to ovarian hormones. Hormones then feedback to the brain to regulate the cycle.
Clinical Correlation: Pharmacological Menopause
Because the hypothalamus must release GnRH in pulses, doctors can use continuous long-acting GnRH agonists (like Leuprolide) to intentionally shut down the pituitary. This stops FSH and LH production, halting the menstrual cycle entirely. This is used to treat severe endometriosis, uterine fibroids, and hormone-responsive cancers.
The Purpose of the Cycle
The menstrual cycle is elegantly designed to ensure that if fertilization occurs, the uterus is perfectly prepared to nurture the developing embryo. If fertilization doesn't happen, the system resets itself, and the cycle begins anew, ready for the next opportunity.
2. Phases of the Menstrual Cycle
The entire process is best understood by looking at two main, overlapping cycles that happen simultaneously:
- The Ovarian Cycle: Focuses on what happens in the ovaries (egg maturation and release).
- The Uterine Cycle: Focuses on what happens in the uterus (preparation and shedding of the lining).
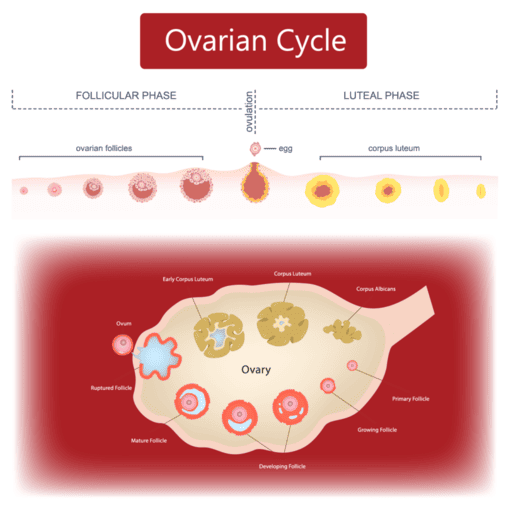
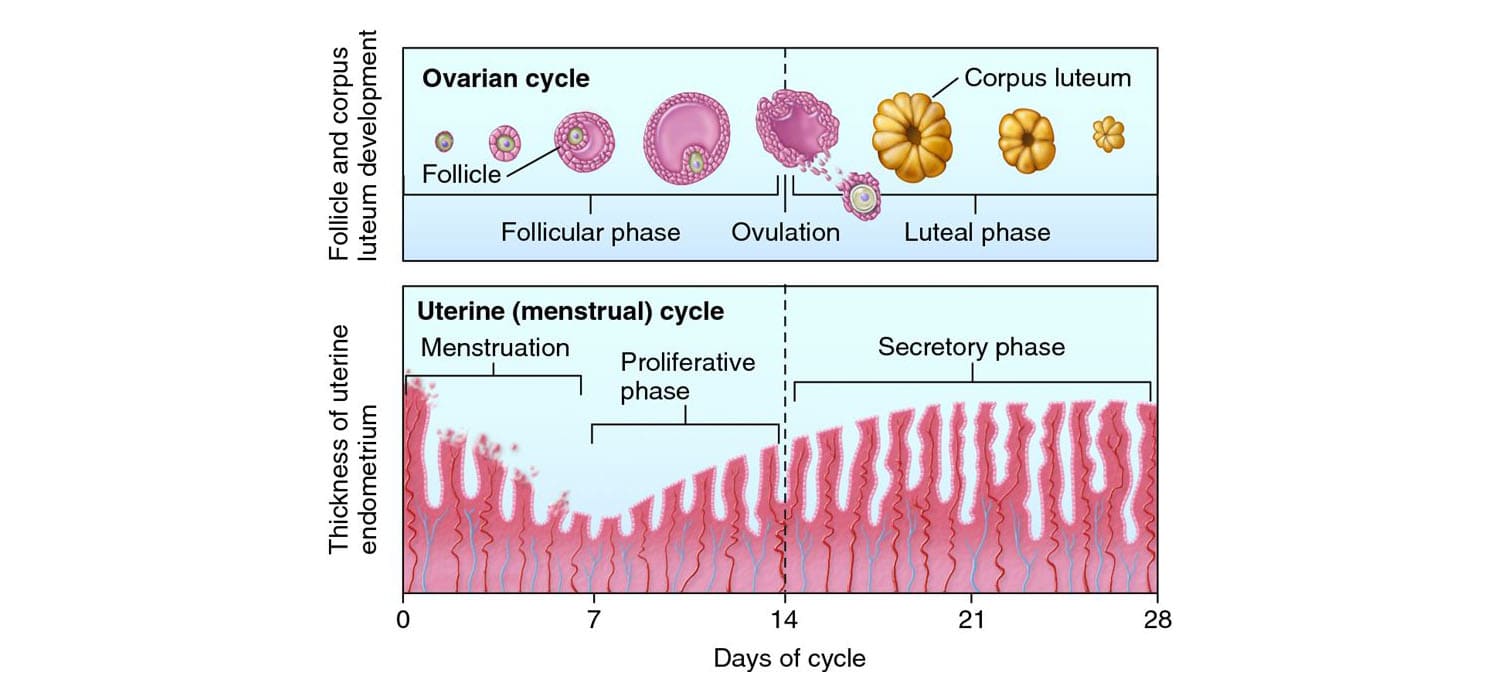
3. The Ovarian Cycle
This cycle describes the series of changes that occur within the follicles of the ovary, driven by fluctuating hormones. It is divided into three distinct phases.
A. The Follicular Phase (Day 1 to ~14)
This phase is highly variable in length among different women, which accounts for the difference between a 28-day and a 35-day cycle.
What happens in the Ovary:
- Follicle Development: Under the influence of FSH, several primordial follicles begin to grow into primary, then secondary follicles.
- Dominant Follicle Selection: Usually, only one follicle becomes the dominant (Graafian) follicle and continues to mature, while the others undergo atresia (programmed cell death).
- Estrogen Production: The growing dominant follicle produces rapidly increasing amounts of estrogen.
Estrogen isn't just magically produced; it requires teamwork between two cell layers in the follicle:
- Theca Cells: Stimulated by LH, they take cholesterol and convert it into Androgens (like testosterone). They cannot make estrogen directly.
- Granulosa Cells: Stimulated by FSH, they take the androgens produced by the theca cells and use an enzyme called Aromatase to convert them into Estrogens (Estradiol).
Hormonal Control:
- FSH (Follicle-Stimulating Hormone): Stimulates initial follicle growth.
- Estrogen: Initially provides negative feedback on FSH (to prevent too many follicles from growing), but as it peaks, it undergoes a unique physiological phenomenon: it switches to positive feedback, leading to the LH surge.
B. Ovulation (Around Day 14)
The Trigger:
The sustained high surge of estrogen from the dominant follicle over 48 hours causes a sudden, dramatic release of Luteinizing Hormone (LH) from the pituitary gland (known as the "LH surge").
What happens in the Ovary:
The LH surge acts on the ovary to trigger the mature dominant follicle to rupture, expelling the secondary oocyte (which is arrested in Metaphase II of meiosis) into the fallopian tube. The egg remains viable for fertilization for around 12 to 24 hours.
Clinical Correlations at Ovulation
- Mittelschmerz: Roughly 20% of women experience mild, unilateral lower abdominal pain during ovulation, caused by the localized peritoneal irritation from the ruptured follicle bleeding slightly.
- Cervical Mucus Changes: The high estrogen peak just before ovulation causes cervical mucus to become thin, clear, and extremely stretchy (resembling raw egg whites). This is called Spinnbarkeit and is highly favorable for sperm penetration and survival.
- Ovulation Predictor Kits (OPKs): These over-the-counter urine tests specifically detect the LH Surge. Since ovulation occurs 24-36 hours after the LH surge begins, it marks the optimal window for conception.
C. The Luteal Phase (~Day 14 to 28)
Unlike the follicular phase, the luteal phase has a strictly fixed duration of exactly 14 days in almost all women.
What happens in the Ovary:
- Corpus Luteum Formation: After ovulation, the ruptured follicle collapses and, driven by LH, transforms into the corpus luteum (literally "yellow body," due to lipid accumulation).
- Hormone Production: The corpus luteum acts as a temporary endocrine gland, producing massive amounts of Progesterone and some estrogen.
- Fate of Corpus Luteum: It has an inherent lifespan. It degenerates into a white scar called the Corpus Albicans after 10-14 days if no pregnancy occurs. If pregnancy occurs, it is "rescued" by hCG to continue producing progesterone.
Hormonal Control:
- Progesterone: Becomes the dominant hormone, preparing the uterus for implantation and raising the basal body temperature by ~0.5°C.
- Negative Feedback: High progesterone, estrogen, and inhibin A levels profoundly inhibit FSH and LH release from the brain, absolutely preventing new follicle development while waiting to see if a pregnancy takes hold.
Clinical Correlation: Luteal Phase Defect
If the corpus luteum is weak and does not produce enough progesterone, the uterine lining cannot be maintained long enough for a fertilized egg to implant. This is a known cause of recurrent early miscarriages. It is often treated clinically by prescribing supplemental progesterone during the second half of the cycle.
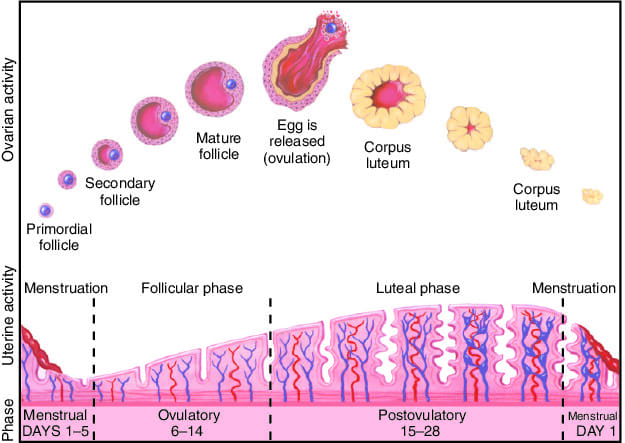
4. The Uterine (Endometrial) Cycle
This cycle describes the corresponding changes occurring in the lining of the uterus (the endometrium). These changes are driven directly by the ovarian hormones, estrogen and progesterone, and are perfectly timed to coincide with the events of the ovarian cycle.
The uterine lining consists of two distinct layers:
- Stratum Basalis: The deep, permanent base layer. It does not shed during menstruation. Its job is to regenerate the layer above it every month.
- Stratum Functionalis: The thick, superficial layer. This is the layer that grows, becomes vascularized, and completely sheds during menstruation.
A. The Menstrual Phase (Day 1 to ~5-7)
What causes it:
This phase marks the official start of the cycle (Day 1). The sharp drop in progesterone and estrogen from the degeneration of the previous cycle's corpus luteum causes intense local release of Prostaglandins. These prostaglandins cause the spiral arteries feeding the stratum functionalis to undergo severe spasms (vasoconstriction).
This causes ischemic necrosis (death from lack of blood flow) of the tissue. The uterine lining breaks down and sheds, resulting in menstrual bleeding.
Purpose: To clear out the old, un-implanted uterine lining, making way for a new, fresh cycle to begin.
Clinical Correlation: Dysmenorrhea (Painful Periods)
The severe cramping many women feel during menstruation is directly caused by the excessive release of Prostaglandins (specifically PGF2α) causing the uterine muscle to strongly contract and the blood vessels to spasm. This is precisely why NSAIDs (Non-Steroidal Anti-Inflammatory Drugs like Ibuprofen), which block prostaglandin synthesis, are the first-line and most effective medical treatment for period pain.
B. The Proliferative Phase (~Day 5-7 to 14)
Driven by Estrogen: Overlapping with the ovarian follicular phase, the rising estrogen from the dominant follicle in the ovary travels to the uterus to stimulate the repair and massive regrowth of the endometrium from the surviving stratum basalis.
What happens in the Uterus:
The stratum functionalis thickens immensely. New blood vessels (spiral arteries) elongate, and straight tubular glands develop, making the lining lush and ready to receive a fertilized egg.
Clinical Correlation: Endometrial Hyperplasia & Cancer
Estrogen acts as a powerful "growth fertilizer" for the uterus. If a woman is exposed to continuous estrogen without any progesterone to balance it (e.g., in Polycystic Ovary Syndrome - PCOS or obesity), the proliferative phase never stops. The lining grows uncontrollably thick, leading to atypical hyperplasia, which is a major precursor to Endometrial Cancer.
C. The Secretory Phase (~Day 14 to 28)
Driven by Progesterone: Overlapping with the ovarian luteal phase, this phase is primarily driven by the massive amounts of progesterone released from the newly formed corpus luteum.
What happens in the Uterus:
While estrogen causes *growth*, progesterone causes *maturation*. Progesterone stops the physical thickening of the endometrium and forces the straight glands to become highly coiled, tortuous, and highly secretory. They begin producing nutrient-rich fluids (glycogen, lipids, mucus) to nourish a potential embryo and make the uterus perfectly receptive for a brief "Window of Implantation" (around days 20-24).
5. What Happens at the End of the Cycle?
There are two possible outcomes, which determine whether the cycle repeats or pauses.
- The corpus luteum reaches the end of its 14-day lifespan and rapidly degenerates (apoptosis) into the corpus albicans.
- Because the factory shut down, Progesterone and Estrogen levels plummet.
- This sudden hormone withdrawal removes the negative feedback on the brain, allowing FSH to start rising again to recruit new follicles.
- Simultaneously, the hormone withdrawal triggers prostaglandin release in the uterus, the spiral arteries spasm, the uterine lining breaks down, and a new period begins at Day 1.
- The fertilized egg becomes a blastocyst and implants into the secretory endometrium (approx. 6-8 days after ovulation).
- The developing outer layer of the embryo (the syncytiotrophoblast) immediately begins producing hCG (Human Chorionic Gonadotropin).
- Crucial Mechanism: hCG is structurally almost identical to LH. It travels to the ovary, binds to the LH receptors on the corpus luteum, and "rescues" it from dying.
- The rescued corpus luteum continues to pump out massive amounts of progesterone.
- Because progesterone remains high, the uterine lining is maintained (no menstruation), the HPO axis remains inhibited (no new eggs mature), and the pregnancy is safely supported until the placenta can take over hormone production around week 8-10.