The Eye, Orbit, and Extraocular Muscles
I. Embryology of the Eye
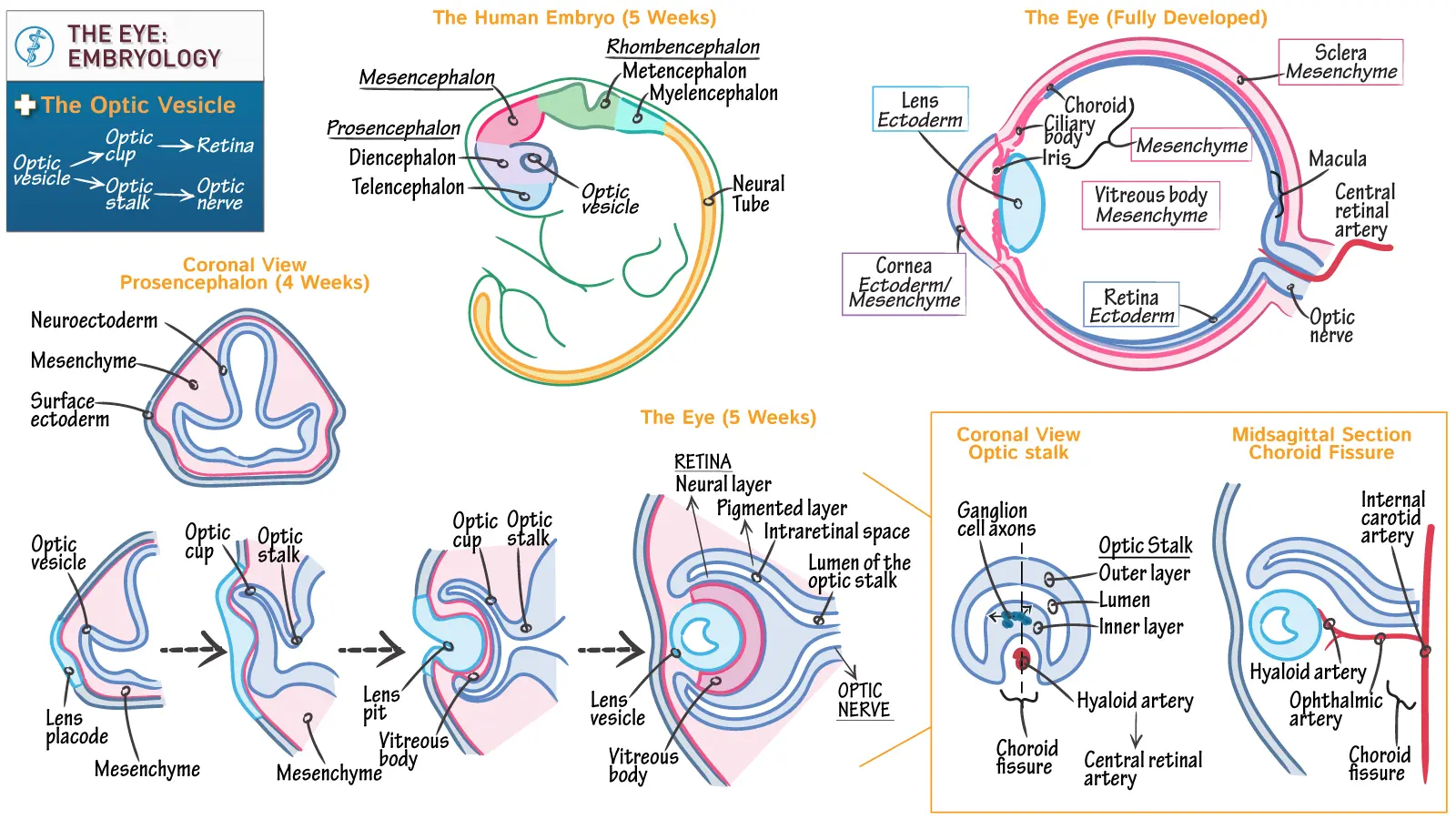
The development of the eye is a complex process involving interactions between neural ectoderm, surface ectoderm, and mesenchyme.
1. Early Development (Optic Vesicles):
- Around day 22 of embryonic development, the eye begins as a pair of shallow optic grooves on the sides of the forebrain.
- With the closure of the neural tube, these grooves evaginate to form optic vesicles, which are outpocketings of the forebrain.
- These optic vesicles then grow laterally to make contact with the surface ectoderm.
2. Lens Formation:
- The optic vesicle induces the overlying surface ectoderm to thicken and invaginate, forming the lens placode.
- The lens placode then invaginates further to form the lens vesicle.
- By the 5th week of intrauterine life, the lens vesicle loses contact with the surface ectoderm and comes to lie within the mouth of the optic cup.
- Germ Layer Origin: The lens is formed from the surface ectoderm.
3. Optic Cup Formation:
- As the lens vesicle forms, the optic vesicle simultaneously invaginates to form a double-walled structure called the optic cup. This invagination also creates the choroid fissure (or optic fissure) along the inferior surface of the optic cup.
- The choroid fissure serves as a pathway for the hyaloid artery (which later becomes the central artery of the retina) to reach the inner chamber of the eye.
- During the 7th week, the lips of the choroid fissure fuse. Failure of this fusion results in a coloboma.
- The anterior opening of the optic cup, formed by the fusion of the choroid fissure lips, becomes the future pupil.
| Optic Cup Layer | Derived Retinal Layers (Posterior 4/5, Pars Optica Retinae) | Derived Iris & Ciliary Body Layers (Anterior 1/5) |
|---|---|---|
| Outer Pigmented Layer | Pigment epithelium of the retina | Outer layer of the iris (pigmented epithelium) and pigmented epithelium of the ciliary body. |
| Inner (Neural) Layer |
|
Inner layer of the iris (pigmented epithelium) and non-pigmented epithelium of the ciliary body (which forms the ciliary processes and contributes to aqueous humor production). |
Congenital Eye Abnormalities
These developmental errors can lead to a range of visual impairments.
1. Coloboma
- Cause: Failure of the choroid fissure to close during the 7th week of development.
- Presentation: A persistent cleft, most commonly in the iris (coloboma iridis), resulting in a keyhole-shaped pupil. It can extend into the ciliary body, retina, choroid, or optic nerve.
- Association: Often associated with other eye defects. Optic nerve colobomas are linked to PAX2 gene mutations and can be part of renal coloboma syndrome (involving kidney defects).
2. Persistence of the Iridopupillary Membrane
- Cause: Failure of the embryonic membrane covering the pupil to resorb during the formation of the anterior chamber.
- Presentation: Fine strands of tissue across the pupil, often benign but can impair vision if dense.
3. Congenital Cataracts
- Cause: The lens becomes opaque during intrauterine life.
- Etiology: Can be genetically determined or caused by intrauterine infections, particularly Rubella (German measles) infection in the mother between the 4th and 7th weeks of pregnancy. Infection after the 7th week might spare the lens but can cause deafness due to cochlear abnormalities.
4. Persistence of the Hyaloid Artery
- Normal Degeneration: The distal portion of the hyaloid artery (which supplied the developing lens) normally degenerates, with the proximal part forming the central artery of the retina.
- Anomaly: Persistence can lead to a fibrous cord or cyst in the vitreous humor, potentially obstructing vision.
5. Microphthalmia
- Definition: Eye is abnormally small, sometimes only 2/3 of its normal volume.
- Association: Usually associated with other ocular abnormalities.
- Causes: Intrauterine infections like cytomegalovirus and toxoplasmosis.
6. Anophthalmia
- Definition: Complete absence of the eye.
- Association: Often accompanied by severe cranial abnormalities.
7. Congenital Aphakia & Aniridia
- Aphakia: Absence of the lens.
- Aniridia: Absence of the iris.
- Rarity: Both are rare.
- Causes: Disturbances in the induction and formation of the tissues involved.
- Genetic Link: Mutations in the PAX6 gene are associated with aniridia and can also contribute to anophthalmia and microphthalmia.
8. Cyclopia & Synophthalmia
- Cyclopia: Single eye.
- Synophthalmia: Fusion of the eyes (partial or complete).
- Spectrum: Represent a spectrum of defects due to a loss of midline tissue during early gestation (days 19-21 or later, affecting facial development).
- Association: Invariably linked to severe cranial defects like holoprosencephaly (merged cerebral hemispheres).
- Etiology: Factors affecting the midline include alcohol exposure, mutations in Sonic Hedgehog (SHH) signaling pathway, and abnormalities in cholesterol metabolism that disrupt SHH signaling.
Bony Orbit
The orbit is a pyramidal-shaped bony cavity that houses the eyeball and its associated structures.
1. Bones Forming the Orbit:
- Each bony orbit is formed by seven bones:
- Maxilla
- Zygomatic
- Frontal
- Ethmoid
- Lacrimal
- Sphenoid
- Palatine
2. Boundaries of the Orbit:
- Apex: The optic foramen (located in the lesser wing of the sphenoid bone).
- Base (Orbital Rim):
- Superiorly: Frontal bone.
- Medially: Frontal process of the maxilla.
- Inferiorly: Zygomatic process of the maxilla and the zygomatic bone.
- Laterally: Zygomatic bone, frontal process of the zygomatic bone, and zygomatic process of the frontal bone.
- Roof (Superior Wall):
- Mainly orbital part of the frontal bone.
- Posteriorly, the lesser wing of the sphenoid bone.
- Medial Wall:
- Composed of four bones: frontal process of maxilla, lacrimal bone, orbital plate of the ethmoid bone, and a small part of the sphenoid bone (body).
- The medial walls of the two orbits are parallel to each other.
- Floor (Inferior Wall):
- Primarily the orbital surface of the maxilla.
- Anterolaterally, the zygomatic bone.
- Posteriorly, the orbital process of the palatine bone.
- Lateral Wall:
- Anteriorly, the zygomatic bone.
- Posteriorly, the greater wing of the sphenoid bone.
3. Orbital Fissures and Foramina:
These openings serve as crucial passageways for nerves, vessels, and other structures.
| Orbital Opening | Boundaries | Contents |
|---|---|---|
| Optic Canal (Foramen) | Lies within the lesser wing of the sphenoid bone, between its two roots. | Optic Nerve (CN II) and the Ophthalmic Artery (a branch of the internal carotid artery). |
| Superior Orbital Fissure | Located between the greater and lesser wings of the sphenoid bone. Connects the orbit with the middle cranial fossa. |
Cranial Nerves: Oculomotor (CN III), Trochlear (CN IV), Ophthalmic division of Trigeminal (CN V1) - branches include Lacrimal, Frontal, Nasociliary nerves, Abducens (CN VI). Vessels: Superior Ophthalmic Vein. Other: Sympathetic fibers to the ciliary ganglion. |
| Inferior Orbital Fissure | Located between the lateral wall (greater wing of sphenoid and zygomatic bone) and the floor (maxilla and orbital process of palatine bone) of the orbit. Connects the orbit with the pterygopalatine and infratemporal fossae. |
Nerves: Zygomatic nerve (branch of CN V2), Infraorbital nerve (another branch of CN V2), Orbital branches of pterygopalatine ganglion. Vessels: Inferior Ophthalmic Vein (which drains into the pterygoid plexus), Infraorbital Artery and Vein. |
| Supraorbital Foramen (or Notch) | Located on the superior orbital margin (frontal bone). | Supraorbital Nerve (terminal branch of the frontal nerve, which is a branch of V1) and Supraorbital Artery. |
| Infraorbital Foramen | Located on the anterior surface of the maxilla, below the inferior orbital rim. | Infraorbital Nerve (continuation of V2 after passing through the infraorbital canal) and Infraorbital Artery and Vein. |
| Anterior Ethmoidal Foramen | Located in the medial wall of the orbit, between the frontal bone and the ethmoid bone. | Anterior Ethmoidal Nerve (branch of nasociliary nerve, from V1) and Anterior Ethmoidal Artery and Vein. |
| Posterior Ethmoidal Foramen | Located in the medial wall of the orbit, posterior to the anterior ethmoidal foramen, between the frontal bone and the ethmoid bone. | Posterior Ethmoidal Nerve (branch of nasociliary nerve, from V1) and Posterior Ethmoidal Artery and Vein. |
| Nasolacrimal Canal | Formed by the lacrimal bone and maxilla, drains tears from the lacrimal sac into the inferior meatus of the nasal cavity. | Contains the nasolacrimal duct. |
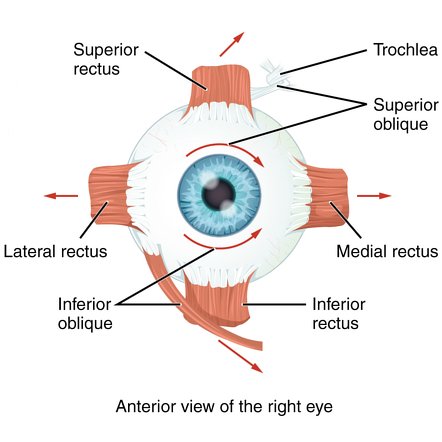
Extrinsic (Extraocular) Muscles of the Eye
These muscles control the movement of the eyeball. They are primarily innervated by CN III, IV, and VI.
1. Origin and Insertion:
- Common Origin: All extrinsic muscles (except the inferior oblique) arise from a common tendinous ring (annulus of Zinn), which surrounds the optic canal and part of the superior orbital fissure.
- Inferior Oblique Origin: The inferior oblique muscle originates from the orbital surface of the maxilla, near the inferior orbital rim.
- Insertions: They insert onto the sclera of the eyeball. The recti muscles insert anterior to the equator of the eyeball, while the oblique muscles insert posterior to the equator.
2. Muscle Actions and Innervation:
| Muscle | Innervation | Primary Action (from primary gaze) | Secondary Action(s) |
|---|---|---|---|
| Superior Rectus | Oculomotor Nerve (CN III) | Elevation (moves eye upward) | Adduction, Intorsion (medial rotation) |
| Inferior Rectus | Oculomotor Nerve (CN III) | Depression (moves eye downward) | Adduction, Extorsion (lateral rotation) |
| Medial Rectus | Oculomotor Nerve (CN III) | Adduction (moves eye medially/inward) | - |
| Lateral Rectus | Abducens Nerve (CN VI) | Abduction (moves eye laterally/outward) | - |
| Superior Oblique | Trochlear Nerve (CN IV) | Intorsion (medial rotation, especially when the eye is adducted) | Depression (when eye is abducted), Abduction |
| Inferior Oblique | Oculomotor Nerve (CN III) | Extorsion (lateral rotation, especially when the eye is adducted) | Elevation (when eye is abducted), Abduction |
| Levator Palpebrae Superioris | Oculomotor Nerve (CN III) (and sympathetic fibers for Müller's muscle) | Elevates the upper eyelid | - |
Key Considerations for Muscle Actions:
- Recti Muscles: All recti muscles pull the eye towards their origin at the apex of the orbit. Because they originate medially to the sagittal axis of the eyeball, all recti (except the lateral rectus) have an adduction component.
- Oblique Muscles: The oblique muscles insert posterior to the equator of the eyeball.
- The Superior Oblique depresses and intorts when the eye is adducted, and abducts. It passes through the trochlea (a cartilaginous pulley) before inserting.
- The Inferior Oblique elevates and extorts when the eye is adducted, and abducts.
3. Laws of Innervation:
- Hering's Law of Equal Innervation: States that synergistic muscles (muscles that work together to produce a gaze direction) receive equal and simultaneous innervation. For example, when looking to the right, the right lateral rectus and left medial rectus receive equal innervation.
- Sherrington's Law of Reciprocal Innervation: States that when an agonist muscle contracts, its antagonist muscle simultaneously relaxes. For example, when the medial rectus contracts to adduct the eye, the lateral rectus relaxes.
Clinical Correlates of Extraocular Muscle Palsies
Damage to the cranial nerves innervating the extraocular muscles results in specific patterns of strabismus (misalignment of the eyes) and diplopia (double vision).
1. Oculomotor Nerve (CN III) Palsy:
- Muscles Affected: Superior rectus, inferior rectus, medial rectus, inferior oblique, and levator palpebrae superioris. Also affects parasympathetic fibers to the iris and ciliary body.
- Clinical Signs:
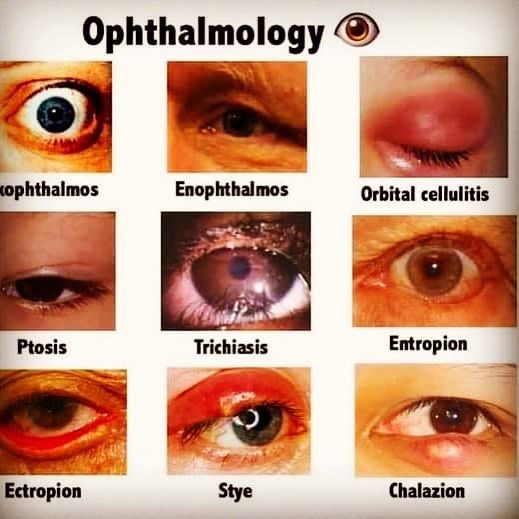
- Ptosis: Drooping of the upper eyelid due to paralysis of the levator palpebrae superioris.
- "Down and Out" Eye: The unopposed action of the superior oblique (depresses and intorts) and lateral rectus (abducts) causes the eye to look inferolaterally.
- Diplopia: Double vision.
- Mydriasis (Dilated Pupil): Due to paralysis of the constrictor pupillae muscle (parasympathetic fibers).
- Loss of Accommodation: Due to paralysis of the ciliary muscle (parasympathetic fibers).
2. Trochlear Nerve (CN IV) Palsy:
- Muscle Affected: Superior oblique.
- Clinical Signs:
- Vertical Diplopia: Especially when looking down and in (e.g., walking down stairs).
- Extorsion: The superior oblique normally intorts the eye, so its paralysis leads to unopposed extorsion.
- Head Tilt: Patients often compensate by tilting their head to the opposite shoulder (chin tuck and head turned away from the affected side) to reduce diplopia, as this position helps to intort the affected eye. This is known as the Bielschowsky head tilt test (or more accurately, the head tilt phenomenon, Bielschowsky test is for differentiating paretic vs non-paretic strabismus).
3. Abducens Nerve (CN VI) Palsy:
- Muscle Affected: Lateral rectus.
- Clinical Signs:
- Medial Deviation (Esotropia): The unopposed action of the medial rectus pulls the eye medially.
- Inability to Abduct the Eye: The affected eye cannot move laterally past the midline.
- Horizontal Diplopia: Especially when looking laterally towards the affected side.
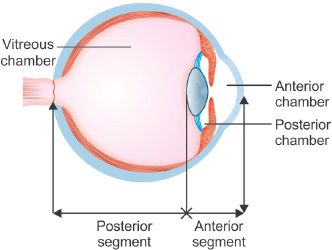
Anterior & Posterior Chambers of the Eye
These fluid-filled spaces are crucial for maintaining intraocular pressure and nourishing the avascular lens and cornea.
1. Aqueous Humor:
- Production: Produced by the ciliary processes (non-pigmented epithelium) of the ciliary body.
- Circulation:
- From the ciliary processes, it flows into the posterior chamber (space between the iris and the lens).
- Passes through the pupil into the anterior chamber (space between the cornea and the iris).
- Drains into the trabecular meshwork, located in the angle between the iris and cornea.
- From the trabecular meshwork, it flows into the canal of Schlemm (scleral venous sinus).
- Finally, it drains into the episcleral veins.
2. Clinical Significance - Glaucoma:
- Definition: A group of eye conditions that damage the optic nerve, often due to abnormally high intraocular pressure (IOP).
- Mechanism: Increased IOP is usually caused by an imbalance between the production and drainage of aqueous humor. Most commonly, it's due to impaired drainage through the trabecular meshwork and/or canal of Schlemm.
- Types:
- Open-angle glaucoma: The trabecular meshwork appears open, but drainage is still impaired.
- Angle-closure glaucoma: The iris blocks the trabecular meshwork, preventing drainage.
Innervation of the Eye
A summary of the complex nervous supply to the eye and its associated structures.
1. Motor Innervation:
- Oculomotor (CN III): Superior rectus, inferior rectus, medial rectus, inferior oblique, levator palpebrae superioris.
- Trochlear (CN IV): Superior oblique.
- Abducens (CN VI): Lateral rectus.
2. Sensory Innervation:
- Trigeminal Nerve (CN V):
- Ophthalmic Division (CN V1): Supplies sensation to the cornea, conjunctiva, eyelids, forehead, and nasal bridge.
- Lacrimal Nerve: Sensory to lacrimal gland, upper eyelid, conjunctiva.
- Frontal Nerve: Divides into supraorbital and supratrochlear nerves, supplying forehead, scalp, upper eyelid.
- Nasociliary Nerve: Sensory to eyeball (cornea, iris, ciliary body), conjunctiva, part of nasal mucosa. Branches include long ciliary nerves (sensory to iris and cornea) and anterior/posterior ethmoidal nerves.
- Ophthalmic Division (CN V1): Supplies sensation to the cornea, conjunctiva, eyelids, forehead, and nasal bridge.
3. Autonomic Innervation:
- Parasympathetic Innervation (Pupillary Constriction and Accommodation):
- Origin: Edinger-Westphal nucleus (midbrain).
- Pathway: Preganglionic fibers travel with CN III, synapse in the ciliary ganglion. Postganglionic fibers (short ciliary nerves) innervate the sphincter pupillae muscle (causing miosis/pupillary constriction) and the ciliary muscle (causing accommodation/lens thickening for near vision).
- Reflexes: Important for pupillary light reflex and accommodation reflex.
- Sympathetic Innervation (Pupillary Dilation):
- Origin: Hypothalamus (first-order neuron) -> Ciliospinal center of Budge (T1-T2 spinal cord) (second-order neuron).
- Pathway: Preganglionic fibers ascend through the sympathetic chain, synapse in the superior cervical ganglion. Postganglionic fibers form a plexus around the internal carotid artery, then join the long ciliary nerves (via ophthalmic artery and nasociliary nerve) to reach the eye.
- Action: Innervates the dilator pupillae muscle (causing mydriasis/pupillary dilation) and Müller's muscle (superior tarsal muscle, contributes to upper eyelid elevation).
- Clinical Significance - Horner's Syndrome: Damage to the sympathetic pathway results in:
- Ptosis: Mild drooping of the upper eyelid (due to paralysis of Müller's muscle).
- Miosis: Constricted pupil (due to paralysis of dilator pupillae).
- Anhidrosis: Absence of sweating on the ipsilateral face.
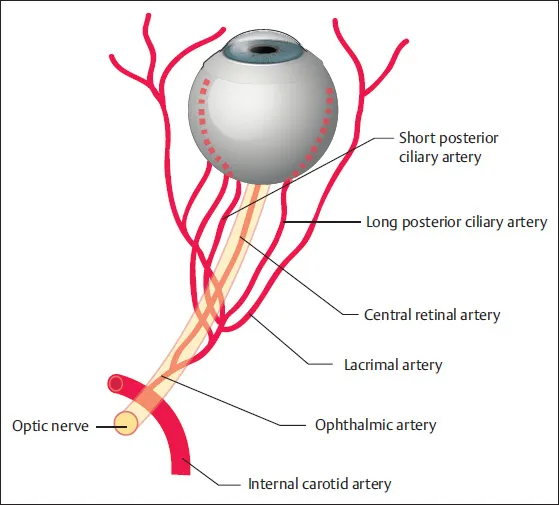
Arterial Supply and Venous Drainage of the Orbit
1. Arterial Supply:
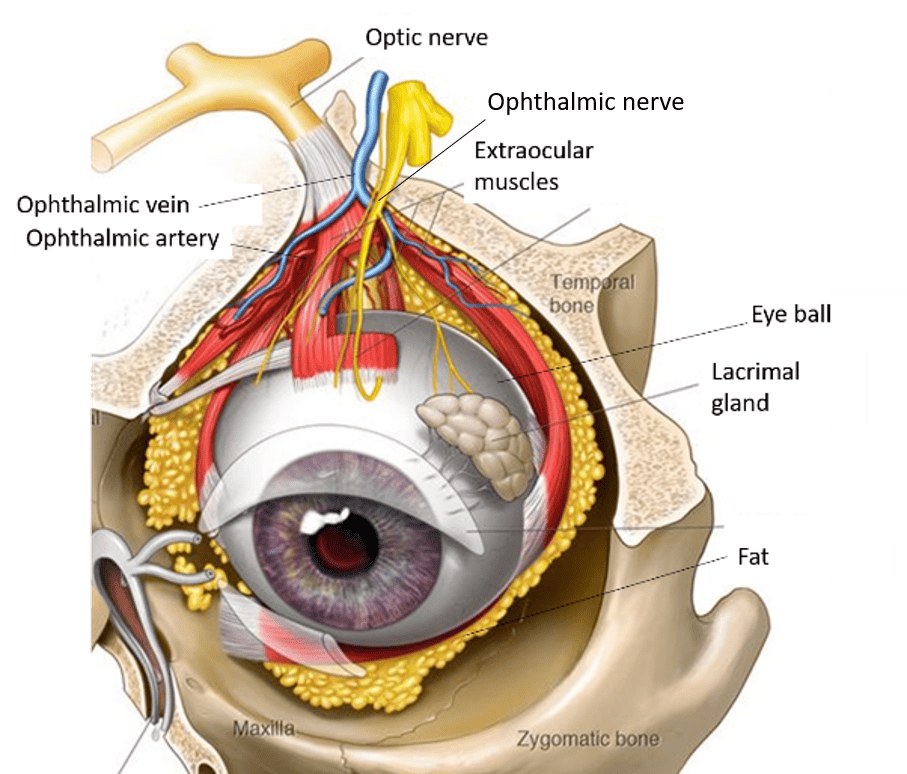
- Main Artery: The ophthalmic artery, a branch of the internal carotid artery.
- Branches of Ophthalmic Artery:
- Central Retinal Artery: Enters the optic nerve, supplies the inner layers of the retina.
- Lacrimal Artery: Supplies lacrimal gland, eyelids, conjunctiva. Gives off zygomatic branches.
- Posterior Ciliary Arteries (long and short): Supply choroid, ciliary body, iris.
- Anterior Ethmoidal Artery and Posterior Ethmoidal Artery: Supply ethmoidal air cells and nasal cavity.
- Supraorbital Artery and Supratrochlear Artery: Supply forehead and scalp.
2. Venous Drainage:
- Superior Ophthalmic Vein: Drains into the cavernous sinus. Communicates with the facial vein.
- Inferior Ophthalmic Vein: Drains into the cavernous sinus and/or the pterygoid venous plexus. Communicates with the facial vein.
- Clinical Significance: The connections between the ophthalmic veins and facial veins are clinically important because infections of the face (e.g., from a pimple on the nose) can potentially spread to the cavernous sinus, leading to cavernous sinus thrombosis.
Other Important Structures
1. Lacrimal Gland
- Function: Produces the watery component of tears.
- Location: Situated in the superolateral part of the orbit, within the lacrimal fossa of the frontal bone.
Innervation of the Lacrimal Gland: The lacrimal gland receives complex innervation involving sensory, secretomotor (parasympathetic), and sympathetic components.
Sensory Innervation
- Pathway: Sensory information from the lacrimal gland, such as irritation or pain, travels back to the central nervous system (CNS).
- Nerve: These sensory neurons travel via the lacrimal nerve, which is a branch of the ophthalmic division (V1) of the trigeminal nerve (CN V).
Secretomotor (Parasympathetic) Innervation
- Function: Stimulates fluid secretion (tear production) from the lacrimal gland. This is the primary secretomotor pathway.
- Pathway:
- Origin: Preganglionic parasympathetic neurons originate in the superior salivatory nucleus in the pons.
- Facial Nerve (CN VII): These fibers exit the brainstem within the facial nerve (CN VII).
- Greater Petrosal Nerve: They then branch off as the greater petrosal nerve.
- Nerve of the Pterygoid Canal (Vidian Nerve): The greater petrosal nerve joins with the deep petrosal nerve (sympathetic fibers) to form the nerve of the pterygoid canal.
- Pterygopalatine Ganglion: The nerve of the pterygoid canal passes into the pterygopalatine ganglion (located in the pterygopalatine fossa), where the preganglionic parasympathetic fibers synapse with postganglionic parasympathetic neurons.
- Maxillary Nerve (V2): The postganglionic parasympathetic fibers do not synapse in the pterygopalatine ganglion for the lacrimal gland. Instead, they "hitchhike" by joining the maxillary division (V2) of the trigeminal nerve.
- Zygomatic Nerve: They continue with the maxillary nerve until they branch off with the zygomatic nerve.
- Zygomaticotemporal Nerve: Within the orbit, the zygomatic nerve gives off the zygomaticotemporal nerve.
- Communicating Branch to Lacrimal Nerve: A small communicating branch from the zygomaticotemporal nerve (carrying the postganglionic parasympathetic fibers) then joins the lacrimal nerve.
- Lacrimal Gland: Finally, the postganglionic parasympathetic fibers, now traveling within the lacrimal nerve, reach and innervate the lacrimal gland, stimulating tear production.
Sympathetic Innervation
- Function: While sympathetic innervation to the lacrimal gland is present, its exact role in tear production is debated. It is thought to primarily influence blood flow to the gland and may have a minor inhibitory role in secretion, or stimulate mucous secretion.
- Pathway:
- Origin: Preganglionic sympathetic neurons originate in the interomediolateral cell column of the upper thoracic spinal cord (T1-T2).
- Superior Cervical Ganglion: These fibers ascend the sympathetic chain and synapse in the superior cervical ganglion.
- Deep Petrosal Nerve: Postganglionic sympathetic fibers form a plexus around the internal carotid artery. They then leave this plexus as the deep petrosal nerve.
- Nerve of the Pterygoid Canal: The deep petrosal nerve joins the greater petrosal nerve (parasympathetic) to form the nerve of the pterygoid canal.
- Pterygopalatine Ganglion: The sympathetic fibers pass through the pterygopalatine ganglion without synapsing.
- "Hitchhiking": From this point onward, the postganglionic sympathetic fibers follow the same intricate "hitchhiking" path as the postganglionic parasympathetic fibers: Join the maxillary division (V2) → Travel with the zygomatic nerve → Branch off into the zygomaticotemporal nerve → Transfer via a communicating branch to the lacrimal nerve → Reach the lacrimal gland.
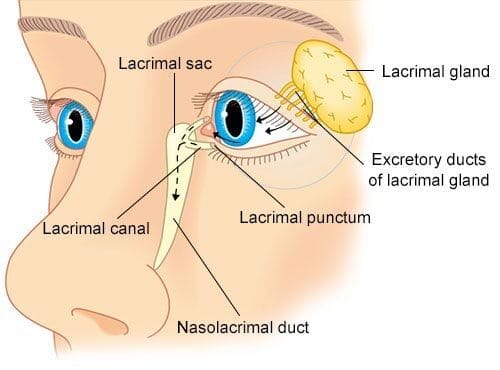
2. Lacrimal Apparatus:
- Lacrimal Gland: Located in the superolateral part of the orbit, produces tears. Innervated by parasympathetic fibers from the facial nerve (CN VII) via the pterygopalatine ganglion.
- Lacrimal Puncta and Canaliculi: Collect tears.
- Lacrimal Sac: Collects tears from canaliculi.
- Nasolacrimal Duct: Drains tears from the lacrimal sac into the inferior meatus of the nasal cavity.
3. Eyelids:
- Orbicularis Oculi Muscle: Closes the eyelids. Innervated by the facial nerve (CN VII).
- Levator Palpebrae Superioris: Elevates the upper eyelid. Innervated by CN III.
- Müller's Muscle (Superior Tarsal Muscle): Smooth muscle that helps elevate the upper eyelid, contributes to widening the palpebral fissure. Innervated by sympathetic fibers.
- Meibomian Glands (Tarsal Glands): Modified sebaceous glands within the tarsal plates, secrete lipid component of tear film to prevent evaporation.
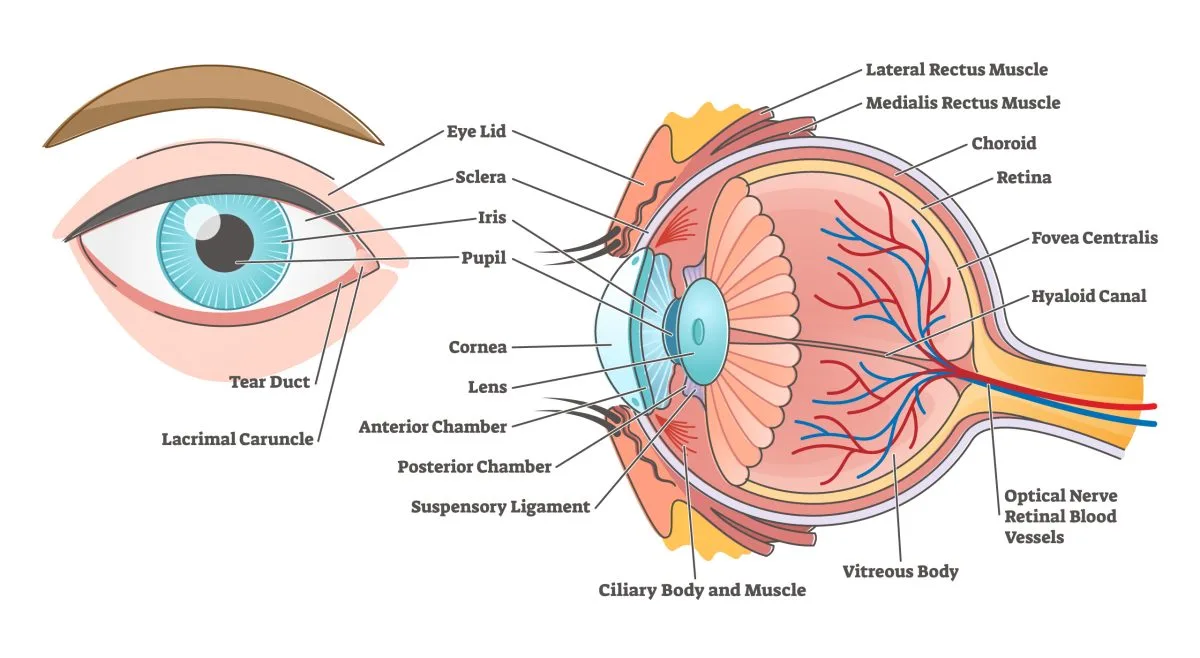
The Eye
The eye is a complex sensory organ responsible for vision. It can be broadly divided into three main coats or tunics, and its internal contents.
1. Structure of the Eyeball
The eyeball is composed of three concentric layers (tunics) and internal structures.
A. Fibrous Coat (Outer Layer)
This is the outermost protective layer, providing shape and strength to the eyeball.
- Sclera:
- The posterior, opaque, and tough part of the fibrous coat.
- Composed of dense connective tissue.
- Continuous posteriorly with the dura mater of the optic nerve.
- Lamina Cribrosa: An area of the sclera near the posterior pole that is perforated by the axons of the retinal ganglion cells (forming the optic nerve) and central retinal vessels. This is a weak point susceptible to damage from increased intraocular pressure.
- Clinical Note: Staphylomas (anterior/posterior) are localized bulges of the sclera, often thinned.
- Cornea:
- The anterior, transparent, and avascular part of the fibrous coat.
- Refracts light, contributing significantly to the eye's focusing power.
- Highly innervated by sensory nerves, making it very sensitive to touch.
B. Vascular Coat (Uvea - Middle Layer)
This layer is rich in blood vessels and pigment.
- Choroid:
- The highly vascular and pigmented layer located between the retina and the sclera.
- Consists of an outer pigmented layer and an inner vascular layer.
- Its primary function is to nourish the outer layers of the retina.
- Ciliary Body:
- Located anterior to the choroid, extending from the ora serrata to the iris.
- Comprises:
- Ciliary Ring: The posterior part.
- Ciliary Processes: Folds that produce aqueous humor.
- Ciliary Muscle: Smooth muscle arranged in meridional and radial fibers. Contraction of this muscle plays a crucial role in accommodation (focusing for near vision) by changing the shape of the lens.
- Iris:
- The pigmented, contractile diaphragm that forms the colored part of the eye.
- Contains a central opening called the pupil.
- Regulates the amount of light entering the eye through two intrinsic muscles:
- Sphincter Pupillae: Circularly arranged fibers that constrict the pupil (miosis) under parasympathetic stimulation.
- Dilator Pupillae: Radially arranged fibers that dilate the pupil (mydriasis) under sympathetic stimulation.
C. Nervous Coat (Retina - Inner Layer)
This is the light-sensitive layer of the eye.
- Composed of an outer pigmented layer and an inner nervous layer.
- Posterior ¾: This part is the receptor organ, containing the photoreceptors (rods and cones).
- Anterior Edge: Forms the ora serrata, the jagged anterior margin of the retina, where the nervous layer ends.
- Anterior ¼: This part is non-receptive and covers the inner surface of the ciliary body and iris.
- Macula Lutea: A yellow-pigmented area near the center of the retina, responsible for central and most distinct vision.
- Fovea Centralis: A small, central depression within the macula lutea, containing the highest concentration of cones, thus providing the sharpest visual acuity.
- Optic Disc (Blind Spot): The area where the optic nerve leaves the eyeball and retinal blood vessels enter and exit. It contains no photoreceptors, hence it's a "blind spot" in the visual field.
Layers of the Retina (from outermost to innermost):
- Pigment cells (part of the retinal pigment epithelium)
- Photoreceptor layer (rods and cones)
- External limiting membrane
- Outer nuclear layer (nuclei of rods and cones)
- Outer plexiform layer
- Inner nuclear layer (bipolar, horizontal, amacrine cells)
- Inner plexiform layer
- Ganglion cell layer
- Nerve fiber layer (axons of ganglion cells, forming the optic nerve)
- Internal limiting membrane
D. Contents of the Eyeball
The eyeball contains various structures and fluid-filled chambers.
- Aqueous Humor:
- A clear, watery fluid produced by the ciliary processes.
- Fills the anterior chamber (between cornea and iris) and posterior chamber (between iris and lens).
- Maintains intraocular pressure and nourishes the avascular cornea and lens.
- Lens:
- A transparent, biconvex, elastic structure located posterior to the iris and anterior to the vitreous humor.
- Focuses light onto the retina by changing its shape (accommodation).
- Vitreous Humor:
- A clear, gelatinous mass that fills the vitreous chamber (posterior to the lens, anterior to the retina).
- Maintains the shape of the eyeball and helps hold the retina in place.
E. Intrinsic Muscles of the Eye (Orbit)
These are smooth muscles within the eyeball, involved in controlling pupil size and lens shape.
- Sphincter Pupillae: Constricts the pupil (miosis).
- Dilator Pupillae: Dilates the pupil (mydriasis).
- Ciliary Muscle: Changes the shape of the lens for accommodation.
2. Blood Supply of the Eyeball
A. Arterial Supply
The primary arterial supply to the eyeball is from the ophthalmic artery, a branch of the internal carotid artery.
- Central Artery of the Retina:
- Enters the eyeball at the center of the optic disc, running within the optic nerve.
- Supplies the inner layers of the retina. Occlusion leads to sudden, painless vision loss.
- Ciliary Arteries:
- Anterior Ciliary Arteries: Supply the anterior structures of the eye, particularly the corneoscleral junction.
- Posterior Ciliary Arteries (Short and Long): Supply the choroid, ciliary body, and iris. The short posterior ciliary arteries are numerous and supply the choroid directly. The long posterior ciliary arteries run forward to supply the ciliary body and iris.
- Cilioretinal Artery:
- Present in a small percentage of individuals.
- A branch of the posterior ciliary arteries that supplies the macula, potentially preserving central vision in central retinal artery occlusion.
B. Venous Drainage
- Central Retinal Vein: Drains the inner layers of the retina and usually accompanies the central retinal artery into the optic nerve. It typically drains into the cavernous sinus.
- Vorticose Veins (4-7 in number): Drain the choroid and exit the sclera obliquely, usually draining into the superior and inferior ophthalmic veins.
- No Lymph Vessels: The eyeball itself lacks lymphatic vessels.
3. Innervation of the Eyeball
The eyeball receives sensory, parasympathetic, and sympathetic innervation.
- Sensory Innervation:
- Primarily via the long ciliary nerves (branches of the nasociliary nerve, from V1 of the trigeminal nerve). These provide general sensation to the cornea, iris, and ciliary body.
- Short ciliary nerves also carry some sensory fibers.
- Parasympathetic Innervation (from Oculomotor Nerve - CN III):
- Pathway: Preganglionic fibers originate in the Edinger-Westphal nucleus, travel with CN III, and synapse in the ciliary ganglion.
- Postganglionic fibers: Travel via the short ciliary nerves.
- Action: Innervate the sphincter pupillae muscle (causing pupillary constriction/miosis) and the ciliary muscle (for accommodation/thickening of the lens for near vision).
- Sympathetic Innervation:
- Pathway: Postganglionic fibers originate in the superior cervical ganglion. They travel along the internal carotid artery plexus.
- Innervation: These fibers reach the eye via the long ciliary nerves (and sometimes also via the short ciliary nerves after passing through the ciliary ganglion without synapsing).
- Action: Innervate the dilator pupillae muscle (causing pupillary dilation/mydriasis) and the smooth muscle components of the levator palpebrae superioris (Müller's muscle, contributing to upper eyelid elevation).
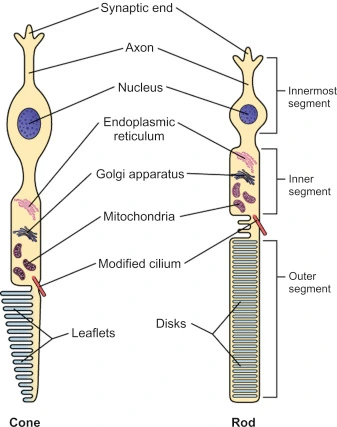
What is a Rod / a Cone?
Rods and cones are the photoreceptor cells in the retina responsible for converting light into electrical signals.
- Rods:
- Shape: Long and cylindrical.
- Function: Responsible for vision in dim light (scotopic vision) and detecting movement. They are highly sensitive but do not detect color.
- Distribution: More numerous than cones, found primarily in the peripheral retina.
- Cones:
- Shape: Shorter and conical.
- Function: Responsible for color vision and high acuity vision in bright light (photopic vision). There are three types of cones, sensitive to different wavelengths (red, green, blue).
- Distribution: Concentrated in the macula lutea, especially the fovea centralis.
Describe the Visual Pathway
The visual pathway describes the route of nerve impulses from the retina to the visual cortex in the brain.
- Photoreceptors (Rods and Cones): In the retina, light activates rods and cones.
- Bipolar Neurons: Photoreceptors synapse with bipolar neurons.
- Ganglion Cells: Bipolar neurons synapse with retinal ganglion cells. The axons of these ganglion cells form the optic nerve.
- Optic Nerve (CN II): Exits the eyeball at the optic disc.
- Optic Chiasm: The optic nerves from both eyes converge. Fibers from the nasal (medial) half of each retina decussate (cross over) to the opposite side, while fibers from the temporal (lateral) half remain uncrossed. This arrangement ensures that the left visual field from both eyes projects to the right side of the brain, and vice-versa.
- Optic Tract: After the chiasm, the fibers form the optic tracts. Each optic tract contains fibers from both eyes corresponding to the contralateral visual field.
- Lateral Geniculate Nucleus (LGN) of the Thalamus: Most fibers in the optic tracts synapse here. The LGN acts as a relay station, organizing and processing visual information.
- Optic Radiations (Geniculocalcarine Tract): Fibers from the LGN form the optic radiations, which project to the visual cortex.
- Primary Visual Areas of the Occipital Lobes: The optic radiations terminate in the primary visual cortex (Brodmann area 17) in the occipital lobes, where visual information is consciously perceived and processed.
Explain Accommodation
Accommodation is the process by which the eye changes its optical power to maintain a clear image (focus) of an object as its distance varies. This is primarily achieved by changing the curvature of the lens.
- For Far Vision (Object > 6 meters):
- Ciliary muscles: Relax.
- Ciliary body: Moves backward and outward, increasing tension on the suspensory ligaments.
- Suspensory ligaments: Taut.
- Lens: Pulled thinner and flatter due to the tension, reducing its refractive power.
- Pupils: Tend to dilate slightly.
- For Near Vision (Object < 6 meters):
- Ciliary muscles: Contract.
- Ciliary body: Moves forward and inward, reducing tension on the suspensory ligaments.
- Suspensory ligaments: Relax.
- Lens: Becomes thicker and rounder due to its inherent elasticity, increasing its refractive power.
- Pupils: Constrict (miosis), which increases the depth of field and improves focus.
- Convergence: The eyes also turn inward (adduct) to maintain focus on the near object.
How does the Light Reflex and the Blink Reflex work?
A. Pupillary Light Reflex
This is an involuntary reflex that controls the diameter of the pupil in response to the intensity of light entering the eye, protecting the retina from overstimulation and optimizing visual acuity. It has both direct and consensual components.
- Afferent Arm:
- Light stimulates photoreceptors in the retina.
- Signals travel via the optic nerve (CN II).
- At the optic chiasm, some fibers cross.
- Fibers continue through the optic tract to the pretectal nucleus in the midbrain (bypassing the LGN).
- From the pretectal nucleus, interneurons project to the Edinger-Westphal nucleus (parasympathetic nucleus of CN III) on both sides of the brainstem.
- Efferent Arm:
- Preganglionic parasympathetic fibers from the Edinger-Westphal nucleus travel with the oculomotor nerve (CN III).
- They synapse in the ciliary ganglion.
- Postganglionic parasympathetic fibers (short ciliary nerves) innervate the sphincter pupillae muscle.
- Result: Contraction of the sphincter pupillae causes pupillary constriction (miosis).
- Direct Light Reflex: Constriction of the pupil in the eye illuminated by light.
- Consensual Light Reflex: Simultaneous constriction of the pupil in the other eye, even though it was not directly illuminated.
B. Blink Reflex (Corneal Reflex)
This is an involuntary protective reflex that causes rapid blinking (closure of the eyelids) in response to stimulation of the cornea or a sudden bright light, or a perceived threat.
- Afferent Arm:
- Stimulation of the cornea (e.g., by touch, foreign body, or sudden bright light).
- Sensory impulses travel via the nasociliary branch of the ophthalmic division (V1) of the trigeminal nerve (CN V).
- Signals are relayed to the spinal nucleus of the trigeminal nerve (V) in the brainstem.
- Efferent Arm:
- From the trigeminal nucleus, interneurons project to the motor nucleus of the facial nerve (CN VII) on both sides.
- Motor impulses travel via the facial nerve (CN VII).
- The facial nerve innervates the orbicularis oculi muscle.
- Result: Contraction of the orbicularis oculi muscle causes rapid closure of the eyelids (blinking).
Clinical Correlates
1. Horner's Syndrome
- Cause: Damage to the sympathetic innervation pathway to the eye and face.
- Symptoms (Triad):
- Ptosis (partial): Mild drooping of the upper eyelid due to paralysis of the superior tarsal muscle (Müller's muscle).
- Miosis: Constricted pupil due to paralysis of the dilator pupillae muscle.
- Anhidrosis: Absence of sweating on the ipsilateral side of the face and neck due to denervation of sweat glands.
2. Holmes-Adie Pupil (Adie's Tonic Pupil)
- Cause: Damage to the postganglionic parasympathetic innervation to the pupil and ciliary muscle, often idiopathic or associated with viral infections.
- Symptoms:
- Unilateral (usually) pupil is larger than the other and reacts poorly to light (slow, tonic constriction).
- Slow, delayed re-dilation after light stimulation.
- Blurred vision, especially for near objects, due to impaired accommodation (partial paralysis of ciliary muscle).
- Often seen in young women.
3. Argyll Robertson Pupil
- Cause: Associated with neurosyphilis and occasionally diabetes mellitus.
- Symptoms:
- "Prostitute's pupil": Accommodates but does not react to light (light-near dissociation).
- Small, irregular, and often unequal pupils.
- Bilateral involvement is common.
4. Tolosa-Hunt Syndrome
- Cause: A rare, painful ophthalmoplegia due to idiopathic granulomatous inflammation of the cavernous sinus or orbital apex.
- Symptoms:
- Unilateral, severe orbital pain.
- Palsies of cranial nerves III, IV, and/or VI, leading to ophthalmoplegia (paralysis of eye movements).
- Sometimes involves CN V1 and V2, causing sensory deficits in the forehead/face.
5. Cavernous Sinus Syndrome
- Cause: A mass lesion (e.g., tumor, aneurysm, infection, thrombosis) affecting the structures within or passing through the cavernous sinus.
- Symptoms:
- Ophthalmoplegia (due to involvement of CN III, IV, VI).
- Sensory loss in the V1 and V2 distribution (forehead, cheek) due to trigeminal nerve involvement.
- Proptosis (exophthalmos) and chemosis (conjunctival swelling) if venous outflow is obstructed (e.g., in cavernous sinus thrombosis).
- Horner's syndrome may also be present due to sympathetic fiber involvement.
6. Closed-Angle Glaucoma (Acute Angle-Closure Glaucoma - AACG)
- Cause: A sudden, significant increase in intraocular pressure (IOP) due to the iris blocking the trabecular meshwork, preventing aqueous humor drainage.
- Mechanism: The iris obstructs the angle between the iris and cornea, where the trabecular meshwork and Canal of Schlemm are located.
- Symptoms:
- Acute, severe eye pain.
- Red eye.
- Blurred vision, often with halos around lights.
- Nausea and vomiting.
- Fixed, mid-dilated pupil.
- Hard eyeball on palpation.
- This is an ophthalmic emergency requiring immediate treatment to prevent irreversible vision loss.
7. Orbital Fracture / Blowout Fracture
- Cause: Trauma to the orbit, often direct blunt trauma to the eye.
- Types:
- Blowout fracture: Fracture of the orbital floor (maxilla) or medial wall (ethmoid) where orbital contents herniate into the maxillary or ethmoid sinuses, respectively.
- Symptoms:
- Enophthalmos: Sunken eye (if significant herniation).
- Diplopia (double vision): Especially on upward gaze if the inferior rectus muscle is entrapped in a floor fracture.
- Impairment of eye movement: Due to muscle entrapment, orbital hemorrhage, or nerve damage.
- Orbital emphysema: Air from paranasal sinuses enters the orbit, causing swelling and crepitus (crackling sensation) when pressed.
- Infraorbital nerve anesthesia: Numbness in the cheek, upper lip, and upper teeth if the infraorbital nerve (branch of V2) is damaged in a floor fracture.
8. Ruptured Globe (Open Globe Injury)
- Cause: Penetrating trauma to the eye, leading to a full-thickness breach of the cornea or sclera and extravasation of intraocular contents.
- Symptoms:
- Severe pain, sudden decrease in vision.
- Hyphema: Blood in the anterior chamber.
- Loss of anterior chamber depth.
- "Tear-drop" pupil: Pupil becomes distorted and points towards the site of the scleral or corneal laceration due to iris prolapse or wound gaping.
- Severe subconjunctival hemorrhage that completely encircles the cornea.
- Consequences: Irreversible visual loss, endophthalmitis (intraocular infection/inflammation). This is a surgical emergency.
9. Central Retinal Artery Occlusion (CRAO)
- Cause: Blockage of the central retinal artery, often by an embolus.
- Symptoms:
- Sudden, painless, and severe monocular vision loss (often described as a curtain coming down).
- Fundoscopic Findings:
- "Cherry-red spot" in the macula (due to the thin macula still being supplied by the choroid, contrasting with the pale, edematous surrounding retina).
- Retinal pallor (paleness) and arterial narrowing.
- Prognosis: Often very poor for visual recovery.
10. Chalazion / Stye (Hordeolum)
- Chalazion:
- Cause: A chronic, sterile, granulomatous inflammation of a Meibomian gland (sebaceous gland in the eyelid).
- Symptoms: Painless, firm, round lump in the eyelid.
- Stye (Hordeolum):
- Cause: Acute bacterial infection of an eyelash follicle (external hordeolum) or a Meibomian gland (internal hordeolum).
- Symptoms: Painful, red, swollen lump on the eyelid margin (external) or within the eyelid (internal). Often tender to touch.

11. Retrobulbar Hematoma / Acute Orbital Compartment Syndrome
- Cause: Hemorrhage into the closed space of the orbit, often secondary to blunt or penetrating trauma (e.g., orbital fracture).
- Mechanism: The blood accumulation rapidly increases intraocular pressure (IOP) within the confined orbital space.
- Symptoms (Ophthalmological Emergency):
- Acute ocular pain.
- Proptosis: Forward displacement of the eyeball.
- Ophthalmoplegia: Restricted eye movements.
- Afferent Pupillary Defect (APD): Reduced or absent direct light reflex in the affected eye, while consensual reflex is intact.
- Diminished vision or vision loss due to compression of the optic nerve and/or retinal ischemia.
- Elevated IOP.
- Treatment: Urgent lateral canthotomy and cantholysis to decompress the orbit and prevent permanent vision loss.