Eye & Ear Anatomy: Comprehensive Master Guide
By the conclusion of this exhaustive master guide, you will be deeply conversant with:
- The complex bony framework, foramina, and neurovascular contents of the orbit.
- The precise origins, insertions, and actions of the extraocular muscles, along with their associated cranial nerve palsies.
- The intricate multi-layered anatomy of the eyeball (fibrous, vascular, and nervous tunics), including fluid dynamics and glaucoma.
- The autonomic pathways governing pupillary responses (mydriasis and miosis) and the complete visual pathway.
- The anatomical subdivisions of the temporal bone and ear (external, middle, inner), including the mechanical amplification of the auditory ossicles.
- The physiological mechanics of sound transduction and vestibular equilibrium.
- The complete, segment-by-segment course of the Facial Nerve (CN VII).
I. The Orbit: Overview & Bony Framework
The orbit is a bilateral, pyramidal bony cavity situated in the upper facial skeleton. It serves to house, protect, and support the eyeball, extraocular muscles, highly delicate vessels, cranial nerves, the lacrimal apparatus, and a protective cushion of orbital adipose (fat) tissue.
- Shape & Volume: It is pyramidal, with the apex directed posteriorly (pointing towards the optic canal) and the base facing anteriorly (forming the orbital margin). The total volume of the orbit is approximately ~30 mL, of which the eyeball occupies only about ~7 mL (the rest is fat, muscles, and neurovasculature).
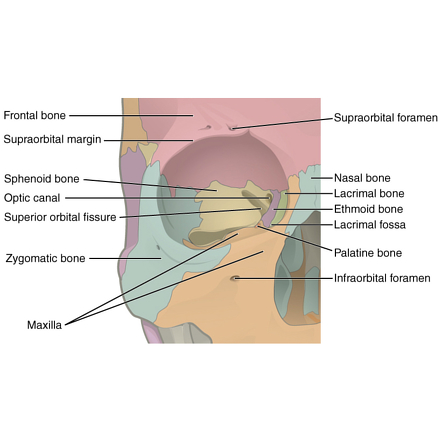
The Seven Bones of the Orbit
The orbital walls are constructed by contributions from seven different bones. (Mnemonic: Many Friendly Zebras Enjoy Lazy Summer Picnics → Maxilla, Frontal, Zygomatic, Ethmoid, Lacrimal, Sphenoid, Palatine).
| Orbital Wall | Bony Composition | Clinical & Anatomical Relations |
|---|---|---|
| Roof (Superior) | Frontal bone (anteriorly) + Lesser wing of sphenoid (posteriorly). | Directly separates the orbit from the frontal sinus (inferiorly) and the anterior cranial fossa (superiorly). |
| Floor (Inferior) | Maxilla (main portion) + Zygomatic (anterolateral) + Palatine (tiny posteromedial contribution). | Separates the orbit from the underlying maxillary sinus. Highly prone to "blowout" fractures. |
| Medial Wall | Maxilla (anterior lacrimal crest), Lacrimal bone (lacrimal sac fossa), Ethmoid (the paper-thin lamina papyracea), Sphenoid body (posteriorly). | THE THINNEST WALL (0.2–0.4 mm thick). Most susceptible to fracture and provides the easiest, most dangerous route for sinus infections (ethmoid sinusitis) to spread directly into the orbit, causing orbital cellulitis. |
| Lateral Wall | Zygomatic (anterior) + Greater wing of sphenoid (posterior). | THE THICKEST WALL. Separates the orbit from the temporal fossa and the middle cranial fossa. |
II. Orbital Openings, Foramina & Neurovasculature
The structural integrity of the orbit is perforated by specific gaps and canals that allow critical nerves and blood vessels to communicate between the brain, the face, and the eye.
- Location: Located exclusively within the lesser wing of the sphenoid bone, at the extreme orbital apex. Length is ~8-12 mm.
- Transmits: The OPTIC NERVE (CN II) and the OPHTHALMIC ARTERY.
- Function: Connects the orbit directly to the middle cranial fossa.
- Location: A dramatic, comma-shaped gap between the lesser wing (above) and greater wing (below) of the sphenoid. It is wider medially and narrows laterally.
- Transmits: CN III (Oculomotor), CN IV (Trochlear), CN V1 (Ophthalmic division of trigeminal—specifically its Frontal, Lacrimal, and Nasociliary branches), CN VI (Abducens), Superior Ophthalmic Vein, and Sympathetic fibers.
- Location: Between the maxilla (anterior/medial) and the greater wing of the sphenoid (posterior/lateral).
- Transmits: Infraorbital nerve (branch of V2/maxillary), Infraorbital vessels, Zygomatic nerve (branch of V2), and the Inferior Ophthalmic Vein (which notably connects to the pterygoid venous plexus).
- Supraorbital Notch/Foramen: In the frontal bone. Transmits the supraorbital nerve (V1 branch) and vessels to the forehead.
- Infraorbital Foramen: In the maxilla. Transmits the infraorbital nerve (V2 branch) and vessels to the cheek.
- Nasolacrimal Canal: In the maxilla, medial wall. Transmits the nasolacrimal duct, dumping tears into the inferior nasal meatus.
Clinical Correlates: SOFS vs. Orbital Apex Syndrome
Superior Orbital Fissure Syndrome (SOFS): Compression or injury (due to skull base fractures, tumors, or cavernous sinus thrombosis) of the structures passing purely through the SOF.
Symptoms: Complete ophthalmoplegia (paralysis of eye movement due to CN III, IV, VI palsies), a fixed dilated pupil (parasympathetic fibers of CN III lost), loss of corneal sensation (V1), and proptosis (bulging eye due to blocked venous drainage). Vision is SPARED.
Orbital Apex Syndrome: This occurs when the pathology extends just slightly deeper to involve the Optic Canal as well.
Key Distinction: Orbital Apex Syndrome presents exactly like SOFS, but WITH profound vision loss because the Optic Nerve (CN II) is now involved.
Orbital Blood Supply Overview
The eye is supplied primarily by the Ophthalmic Artery, which is the very first branch of the Internal Carotid Artery (arising just after the ICA exits the cavernous sinus). It enters the orbit via the optic canal, positioned inferolaterally to the optic nerve, and then typically crosses over the optic nerve from lateral to medial, giving off multiple branches.
- Central Retinal Artery: The most critical branch. Enters the optic nerve ~10-12 mm behind the globe, running perfectly within its dural sheath. It enters the eye at the optic disc and bifurcates to supply the inner retina.
- Lacrimal Artery: Supplies the lacrimal gland and lateral rectus.
- Posterior Ciliary Arteries: Short ones supply the choroid; long ones supply the iris and ciliary body.
Central Retinal Artery Occlusion (CRAO)
If an embolus blocks the Central Retinal Artery, it causes acute, painless, profound monocular vision loss. Upon fundoscopic examination, the retina is pale and swollen, with a classic "Cherry-red spot" visible at the macula (because the extremely thin macula is supplied by the underlying choroid circulation, which shines red against the pale dead retina).
Retinal Ischemia Time Window: You have approximately 90-100 minutes to restore blood flow before irreversible, permanent blindness occurs!
III. Extraocular Muscles & Detailed Actions
There are exactly SIX extraocular muscles that control the precise movement of the globe: Four recti (superior, inferior, medial, lateral) and two obliques (superior, inferior).
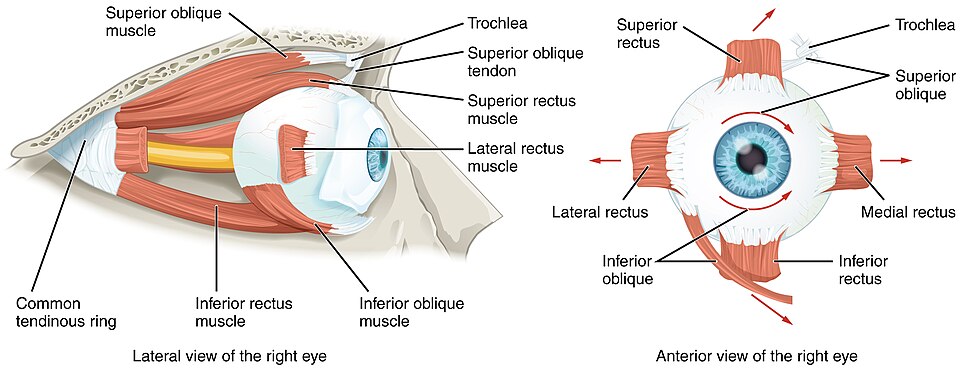
- Common Tendinous Ring (Annulus of Zinn): A fibrous ring at the orbital apex that surrounds the optic canal and part of the superior orbital fissure. It is the anatomical origin for ALL four rectus muscles and the superior oblique. The only muscle that does not originate here is the Inferior Oblique.
- Rectus Muscles: They form a "muscle cone" (intraconal space) as they travel forward. They insert onto the anterior sclera at varying distances from the limbus (corneocorneal junction). Medial rectus is closest (~5.5mm), Superior rectus is furthest (~7.7mm).
Detailed Actions of the Muscles
Understanding the actions requires knowing that the primary action is the strongest pull, followed by secondary and tertiary torsional actions due to the angle of the orbit.
| Muscle | Innervation | Primary Action | Secondary / Tertiary Actions |
|---|---|---|---|
| Superior Rectus (SR) | CN III (Superior div.) | Elevation | Adduction, Intorsion |
| Inferior Rectus (IR) | CN III (Inferior div.) | Depression | Adduction, Extorsion |
| Medial Rectus (MR) | CN III | Adduction | None. It is the STRONGEST extraocular muscle. |
| Lateral Rectus (LR) | CN VI (Abducens) | Abduction | None. It is the WEAKEST extraocular muscle. |
| Superior Oblique (SO) | CN IV (Trochlear) | Intorsion | Depression (best when adducted), Abduction (minimal) |
| Inferior Oblique (IO) | CN III (Inferior div.) | Extorsion | Elevation (best when adducted), Abduction (minimal) |
Why do Obliques have "opposite" vertical actions?
Because they insert POSTERIOR to the equator of the globe (unlike recti which insert anteriorly). When the superior oblique pulls, it pulls the BACK of the eye UP, causing the FRONT of the eye (the pupil) to go DOWN.
Isolating Muscle Actions in Different Gaze Positions
To clinically test a specific muscle, you must put the eye in a position where the other muscles are at a mechanical disadvantage.
- To isolate Superior Rectus (SR): Ask the patient to look UP and OUT (Abducted).
- To isolate Inferior Rectus (IR): Ask the patient to look DOWN and OUT.
- To isolate Superior Oblique (SO): Ask the patient to look DOWN and IN (Adducted).
- To isolate Inferior Oblique (IO): Ask the patient to look UP and IN.
Mnemonic: "IOU" → Inferior Oblique acts when the eye is looking In for Up (Elevation).
IV. Cranial Nerves of the Eye & Associated Palsies
The innervation of the extraocular muscles follows the classic medical formula: LR6-SO4-Rest3. (Lateral Rectus = CN VI, Superior Oblique = CN IV, All others = CN III).
1. Cranial Nerve III (Oculomotor)
- Course: Exits the midbrain through the interpeduncular fossa, passing dangerously between the posterior cerebral artery and superior cerebellar artery. It travels through the cavernous sinus and enters the orbit via the SOF, dividing into superior and inferior divisions.
- Complete CN III Palsy: Results in a "DOWN AND OUT" eye position. Why? Because the lateral rectus (abduction) and superior oblique (depression + intorsion) are the only muscles still working, pulling the eye inferolaterally.
- Accompanying Signs:
- Ptosis: Complete eyelid droop due to paralyzed levator palpebrae superioris. (Ironically, this "protects" the patient from seeing double vision because the lid covers the deviated eye).
- "Blown Pupil": Dilated, non-reactive pupil. The parasympathetic fibers run on the superficial exterior of CN III, making them highly vulnerable to compression.
- Loss of Accommodation: Cannot focus on near objects due to ciliary muscle paralysis.
- "Surgical" vs "Medical" CN III Palsy:
- Pupil-Involved (Dilated) = Surgical Emergency! This indicates external COMPRESSION (e.g., an aneurysm of the Posterior Communicating Artery pressing on the outside of the nerve).
- Pupil-Spared = Medical Issue. This indicates internal ISCHEMIA (e.g., microvascular disease from Diabetes). The inner motor fibers die, but the outer superficial pupillary fibers survive.
2. Cranial Nerve IV (Trochlear)
- Course: The ONLY cranial nerve to exit dorsally from the brainstem. It decussates (crosses over) immediately, meaning a right brainstem lesion affects the left eye. It has the longest, thinnest intracranial course, making it highly susceptible to trauma.
- Palsy Clinical Features: Presents as Vertical Diplopia (images stacked on top of each other), which is notably worse when looking DOWN and IN (like reading a book or walking down stairs).
- Bielschowsky Head Tilt Test: The patient will consciously tilt their head AWAY from the affected side to minimize the double vision. Pathophysiology: The vestibular system counter-rolls the eyes when the head tilts. In an SO palsy, the affected eye cannot internally rotate (intort) properly. Tilting the head away stops the brain from demanding intorsion from the broken muscle.
3. Cranial Nerve VI (Abducens)
- Course: Exits the brainstem at the pontomedullary junction, ascends the clivus, makes a sharp 90-degree bend over the petrous apex (Dorello canal), travels through the cavernous sinus (medial to the ICA), and enters the SOF.
- Vulnerability: Because it has the longest intracranial course across the skull base and makes a sharp bend, any increase in Intracranial Pressure (ICP) will stretch and paralyze this nerve. Therefore, a CN VI palsy is often a "False Localizing Sign" (it tells you ICP is high, but the actual tumor/bleed might be far away on the other side of the brain).
- Palsy Clinical Features: Esotropia (the eye turns INWARD toward the nose, forming a "crossed eye"). The patient has an absolute inability to abduct the eye past the midline. Horizontal diplopia is worse when looking TOWARD the affected side.
V. Eyelid & Lacrimal Apparatus Anatomy
Eyelid Anatomy (Superficial to Deep)
- Skin: Extremely thin, virtually no subcutaneous fat. Easy visibility of vascular structures.
- Orbicularis Oculi: Skeletal muscle innervated by CN VII. Closes the eye. Three parts: Orbital (voluntary tight squeeze), Palpebral (gentle involuntary blink), Lacrimal (aids tear pump drainage).
- Tarsal Plates: Dense connective tissue (NOT cartilage) providing rigid structural support. Upper tarsus is larger (~10-12 mm) than the lower (~4-5 mm).
- Tarsal (Meibomian) Glands: Modified sebaceous glands housed within the tarsal plates. They secrete the essential lipid (oil) layer of the tear film, which prevents evaporation.
Clinical Note: Meibomian Gland Dysfunction (MGD) is the most common cause of evaporative dry eye. Glands block, lipids don't secrete, tears evaporate instantly, causing ocular surface damage. - Conjunctiva: Mucous membrane lining the inner lid.
Lid Elevators:
- Levator Palpebrae Superioris: Skeletal muscle (CN III). The main lifter. Inserts into the tarsus and skin (creating the upper eyelid crease).
- Müller Muscle (Superior Tarsal Muscle): Smooth muscle fibers (Sympathetic innervation). Provides an extra ~2 mm of lift. Paralyzed in Horner Syndrome, causing mild ptosis.
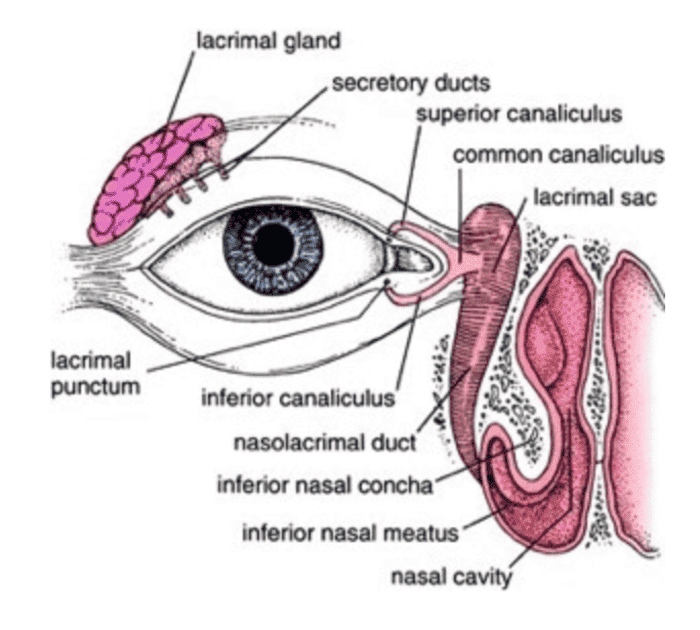
Lacrimal Apparatus & Tear Drainage
The tear film requires three layers: Lipid (Meibomian glands), Aqueous (Lacrimal gland - main volume), and Mucin (Conjunctival goblet cells - sticks tears to the eye).
- Lacrimal Gland: Almond-shaped, sits superolaterally. Parasympathetic secretomotor innervation from CN VII (via the complex path: greater petrosal nerve → pterygopalatine ganglion → zygomatic nerve → lacrimal nerve).
- Drainage Pathway: Puncta (medial dots) → Canaliculi → Lacrimal Sac → Nasolacrimal Duct → Inferior Nasal Meatus (under the inferior concha).
- Valve of Hasner: A mucosal fold at the end of the duct. If imperforate in newborns, it causes congenital nasolacrimal duct obstruction (tearing, chronic mucoid discharge).
- The Lacrimal Pump: Blinking creates negative pressure in the lacrimal sac, sucking tears in, and then squeezing them down the duct. (Mnemonic: "Tears flow DOWN and IN" - from the superolateral gland across the eye, down the duct into the nose. This is why crying gives you a runny nose!).
VI. Anatomy of the Eyeball (The Three Tunics)
The eyeball is ~24 mm in diameter and consists of three concentric coats.
- Sclera: Opaque, tough, white collagenous layer. Thickest posteriorly, thinnest right behind the rectus muscle insertions. Contains emissary canals for vessels. (Blue sclera indicates Osteogenesis Imperfecta—the sclera is abnormally thin, showing the dark uvea underneath).
- Cornea: Transparent, highly innervated, avascular. Provides 2/3 of the eye's total refractive power (~43 diopters).
5 Layers: Epithelium (regenerates), Bowman layer (no regeneration), Stroma (90% thickness, perfectly ordered collagen), Descemet membrane, Endothelium.
Endothelial Cell Loss: These cells act as water pumps to keep the cornea dehydrated and clear. They NEVER divide. Density drops from 3,500/mm² at birth to 2,000 in old age. If it drops below ~500/mm², the cornea floods with fluid (bullous keratopathy), turning blind and cloudy, requiring a transplant.
- Choroid: Highly vascular layer supplying the outer retina. Contains melanocytes to absorb scattered light.
- Ciliary Body: Contains the Pars Plicata (anterior folds that produce aqueous humor) and the Pars Plana (flat posterior section—the safest entry point for intraocular surgery).
- Iris: The colored diaphragm. Contains the Sphincter pupillae (circular, parasympathetic, miosis) and Dilator pupillae (radial, sympathetic, mydriasis).
- Retina: Complex neural tissue with 10 distinct histological layers (from Retinal Pigment Epithelium to the Inner Limiting Membrane).
- Photoreceptors:
- Rods (~120 million): High sensitivity, scotopic (low-light, night vision), no color, located in the periphery.
- Cones (~6 million): Lower sensitivity, photopic (bright light), color vision, highly concentrated in the center. - Macula & Fovea: The center of the retina. The Fovea Centralis contains ONLY cones, possesses NO blood vessels, and NO ganglion cells above the photoreceptors, allowing light an unimpeded path for the highest visual acuity.
- Optic Disc (Blind Spot): Where the optic nerve exits. No photoreceptors exist here. Physiologic cup-to-disc ratio is <0.3. If >0.5, suspect Glaucoma!
Aqueous Humor Dynamics & Glaucoma ("The Silent Thief of Sight")
Aqueous humor is actively secreted (~2.5 μL/min) by the non-pigmented ciliary epithelium into the posterior chamber. It flows through the pupil into the anterior chamber, then drains out the iridocorneal angle via the Trabecular Meshwork into Schlemm's Canal, finally emptying into episcleral veins.
- Primary Open-Angle Glaucoma (POAG): Most common (~90%). The drainage angle appears structurally open, but there is microscopic resistance deep inside the trabecular meshwork. Leads to chronic, painless, insidious elevation of Intraocular Pressure (IOP), destroying the optic nerve and causing peripheral vision loss.
- Primary Angle-Closure Glaucoma (PACG): An acute emergency. The iris physically bows forward, sealing off the trabecular meshwork. IOP spikes suddenly from normal (10-21 mmHg) to dangerous levels (30-80 mmHg). Symptoms: Severe eye pain, rock-hard eyeball, nausea, blurred vision with colored halos, and a fixed, mid-dilated pupil. Requires instant pressure-lowering drugs and laser iridotomy to punch a relief hole in the iris.
The Lens & Accommodation
A biconvex, transparent, entirely avascular structure suspended by zonular fibers. It provides the remaining ~15-20 diopters of refractive power. As it ages, the central nucleus becomes hard and sclerotic.
- Accommodation (Near Vision Focus): To look at something close, the ciliary muscle CONTRACTS (parasympathetic CN III). This acts like a sphincter, making the muscle ring smaller, which paradoxically causes the zonular fibers to RELAX and go slack. Freed from tension, the highly elastic lens snaps into a MORE CONVEX (rounder) shape, increasing its power to bend near light rays onto the retina.
- Presbyopia: Age-related loss of accommodation. The lens hardens and loses elasticity. By age 40-45, people complain their "arms are too short" to read a book, requiring reading glasses.
- Cataract: Opacification (clouding) of the lens. Risk factors include age, UV exposure, diabetes, smoking, and steroids. Treatment is surgical phacoemulsification and artificial lens implantation.
VII. Autonomic Pathways & The Pupil
The size of the pupil is a constant tug-of-war between Sympathetic (dilation) and Parasympathetic (constriction) forces.
1. Sympathetic Pathway (Mydriasis / Dilation)
A long, complex 3-order neuron pathway. (Mnemonic path: Hypothalamus → T1 → Superior Cervical → Eye).
- 1st Order (Central): Posterior hypothalamus down the brainstem to the ciliospinal center of Budge (T1 spinal cord).
- 2nd Order (Preganglionic): Exits T1, travels UP the sympathetic chain over the apex of the lung to synapse in the Superior Cervical Ganglion.
- 3rd Order (Postganglionic): Ascends physically wrapped around the Internal Carotid Artery (carotid plexus), passes through the cavernous sinus, and enters the orbit to innervate the Dilator Pupillae and Müller's eyelid muscle.
Horner Syndrome
A lesion anywhere along this 3-neuron sympathetic chain causes the classic triad: 1. Ptosis (mild, paralyzed Müller muscle), 2. Miosis (constricted pupil, unopposed parasympathetic tone), and 3. Anhidrosis (absent sweating on that half of the face).
Localization trick: A Pancoast tumor (lung cancer at the apex) compresses the 2nd order neuron. A carotid artery dissection tears the 3rd order neuron.
Pharmacologic Testing: Apraclonidine 0.5% drops. A normal pupil ignores it. A Horner's pupil has "denervation supersensitivity" and will dramatically DILATE, confirming the diagnosis.
2. Parasympathetic Pathway (Miosis & Accommodation)
A much shorter, 2-neuron pathway for "rest and digest" tasks.
- Preganglionic: Originates in the Edinger-Westphal nucleus in the midbrain. Travels on the superficial exterior of CN III to the Ciliary Ganglion behind the eye.
- Postganglionic: Short ciliary nerves travel to the Sphincter Pupillae (causes miosis) and Ciliary Muscle (causes accommodation).
3. Light Reflex & Pupil Abnormalities
When you shine light in one eye, BOTH pupils constrict. The Afferent limb is CN II (Optic nerve to pretectal nucleus). The Efferent limb is CN III bilaterally.
| Pupil Abnormality | Pathophysiology & Presentation |
|---|---|
| Argyll Robertson Pupil | "Accommodates but does not react" to light (Light-near dissociation). Small, irregular pupils. Strongly associated with tertiary Neurosyphilis (lesion in the dorsal midbrain). |
| Marcus Gunn Pupil (RAPD) | Relative Afferent Pupillary Defect. Due to asymmetric optic nerve damage (e.g., Optic Neuritis in MS). Swinging flashlight test: When moving the light from the good eye to the sick eye, BOTH pupils paradoxically DILATE because the brain perceives the sick eye's signal as "darkness". |
| Adie Tonic Pupil | A large, poorly reactive pupil that constricts very slowly and dilates very slowly. Due to ciliary ganglion degeneration. Often seen in young women with diminished tendon reflexes. |
VIII. The Visual Pathway & Visual Field Defects
Understanding the wiring of the visual system allows precise anatomical localization of brain tumors or strokes based entirely on what a patient cannot see.
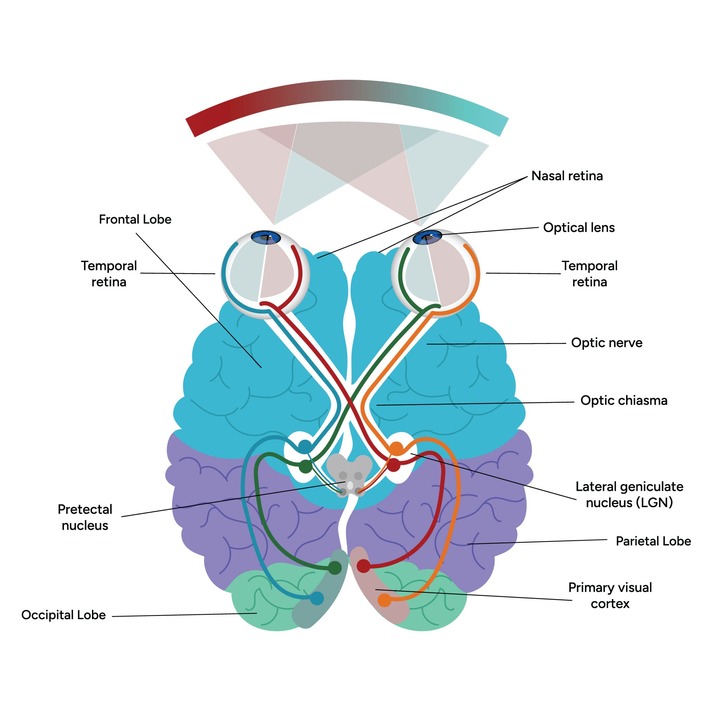
- Retina & Optic Nerve (CN II): Ganglion cell axons form the optic nerve. A lesion here causes complete monocular visual loss (blindness in one eye).
- Optic Chiasm: Located directly above the pituitary gland. Rule: "Nasal crosses, Temporal stays." The fibers from the nasal half of the retina (which process the temporal/outer visual field) cross over. A large pituitary tumor pressing up on the chiasm cuts these crossing fibers, causing Bitemporal Hemianopia (tunnel vision; missing the outer halves of both visual fields).
- Optic Tract: Post-chiasm. Now contains fibers from the same side of both visual fields. A lesion here causes Homonymous Hemianopia (loss of the same half of the visual field in both eyes).
- Lateral Geniculate Nucleus (LGN): Relay station in the thalamus.
- Optic Radiations: Sweeping tracts to the back of the brain.
- Temporal Lobe (Meyer's Loop): Carries inferior retinal fibers (processing superior vision). A temporal lobe stroke destroys Meyer's loop, causing "Pie in the sky" (Superior Quadrantanopia).
- Parietal Lobe Radiations: Carries superior retinal fibers (processing inferior vision). A parietal stroke causes "Pie on the floor" (Inferior Quadrantanopia).
- Primary Visual Cortex (Occipital Lobe): A stroke here causes Homonymous Hemianopia, but uniquely WITH Macular Sparing. Because the macula is so vital, its representation at the very tip of the occipital pole receives dual blood supply from both the Posterior Cerebral Artery (PCA) and Middle Cerebral Artery (MCA). A PCA stroke kills the peripheral vision, but the MCA keeps the central macular vision alive!
IX. Venous Drainage & The Cavernous Sinus
Orbital veins (Superior and Inferior Ophthalmic Veins) drain the eye and exit posteriorly. Crucially, they possess NO VALVES. Blood can flow in either direction. This anatomical quirk allows infections from the face (the "danger triangle" around the nose/upper lip) to travel directly backwards into the brain, specifically into the Cavernous Sinus.
The Cavernous Sinus
Located on either side of the sella turcica. It is a massive venous pool that has critical structures running directly through its center and along its lateral walls.
- Running directly through the center (with the blood): The Internal Carotid Artery (plus sympathetic plexus) and CN VI (Abducens). (This makes CN VI highly vulnerable to cavernous sinus pathology).
- Embedded in the lateral wall: CN III, CN IV, CN V1 (Ophthalmic), and CN V2 (Maxillary).
Cavernous Sinus Thrombosis (CST): A lethal septic clot inside the sinus. Symptoms include violent headache, high fever, massive chemosis (swollen conjunctiva), proptosis, and total ophthalmoplegia ("frozen eye" as CN III, IV, and VI are paralyzed). Facial sensory loss occurs due to V1 and V2 compression.
X. The Ear: Temporal Bone & External/Middle Ear Anatomy
Hearing and balance are housed within the intricate cavities of the Temporal Bone.
1. Temporal Bone Subdivisions
- Squamous: Thin, flat, forms the side of the skull and the zygomatic process.
- Mastoid: Contains air cells. Provides attachment for the sternocleidomastoid muscle.
- Tympanic: Curved plate forming the external auditory meatus.
- Petrous: Pyramid-shaped, incredibly dense bone. Houses the entire inner ear (cochlea, vestibule), the internal carotid artery, and the jugular vein. Its density protects delicate hearing structures but makes surgical access a nightmare.
2. External Ear
Comprises the Auricle (pinna) made of elastic cartilage to collect sound, and the External Acoustic Meatus (canal). The outer 1/3 is cartilage containing ceruminous glands (producing earwax for protection); the inner 2/3 is solid bone.
Pediatric Note: An infant's ear canal is shorter and more horizontal. To see the eardrum, you pull the pinna DOWN and BACK. In adults, you pull UP and BACK.
3. Middle Ear (The Tympanic Cavity)
An air-filled, mucosa-lined space containing the ossicles. Think of it as a square box with 6 specific walls:
- Roof (Tegmental wall): Paper-thin bone separating it from the brain (middle cranial fossa). A fracture here leaks CSF out the ear.
- Floor (Jugular wall): Separates it from the massive Internal Jugular Vein.
- Anterior (Carotid wall): Separates it from the Internal Carotid Artery. Contains the opening to the Eustachian tube.
- Posterior (Mastoid wall): Has an opening (aditus) leading back into the mastoid air cells. Contains the pyramidal eminence housing the stapedius muscle.
- Medial (Labyrinthine wall): Separates it from the inner ear. Features the Promontory (bulge of the cochlea), the Oval window (where the stapes pushes in), and the Round window (pressure release). The Facial Nerve (CN VII) canal bulges just above the oval window, making it highly vulnerable during middle ear surgery!
- Lateral (Membranous wall): Formed primarily by the Tympanic Membrane (eardrum).
Three tiny bones bridge the gap from the eardrum to the inner ear: Malleus (hammer) → Incus (anvil) → Stapes (stirrup).
Sound traveling from air (middle ear) into fluid (inner ear) naturally loses 99.9% of its energy due to impedance mismatch. The ossicles perform a mechanical miracle to fix this:
- Area Ratio: The large surface area of the eardrum funnels all its force down onto the tiny footplate of the stapes (a ~17:1 ratio). This acts like a stiletto heel, concentrating the pressure massively.
- Lever Action: The malleus handle is longer than the incus, adding a 1.3x mechanical lever advantage.
Total Result: ~22x pressure amplification at the oval window. Without this, we would essentially be deaf to airborne sounds.
To prevent this massive amplification from blowing out our inner ear during loud noises, we have two protective dampening muscles:
- Tensor Tympani: Attaches to the malleus. Innervated by CN V3 (Mandibular nerve). Tenses the eardrum.
- Stapedius: The smallest muscle in the body. Attaches to the stapes. Innervated by CN VII (Facial nerve). It physically pulls the stapes away from the oval window during loud sounds (the Acoustic Reflex).
Pathology: Paralysis of the stapedius (e.g., in Bell's Palsy) causes Hyperacusis, where normal sounds are perceived as painfully, brutally loud.
4. The Eustachian (Pharyngotympanic) Tube
Connects the anterior middle ear to the nasopharynx. Its main job is to ventilate the middle ear, keeping the pressure exactly equal to the atmospheric pressure outside, allowing the eardrum to vibrate freely.
- Normally closed, it opens during swallowing or yawning via the pull of the Tensor Veli Palatini muscle (CN V3).
- Pediatric Vulnerability: In infants, the tube is shorter, wider, and much more HORIZONTAL. When a baby lies on their back and cries or refluxes, bacteria from the throat easily slide horizontally straight into the middle ear, causing high rates of Otitis Media (middle ear infections).
XI. Inner Ear: Hearing & Balance (Cochlea & Vestibular System)
The inner ear is a complex maze of fluid-filled tubes hollowed out of the petrous bone (the Bony Labyrinth), containing soft tissue tubes inside them (the Membranous Labyrinth).
- Perilymph: Fills the bony labyrinth (outside the membrane). Chemically identical to CSF and extracellular fluid (High Na+, Low K+).
- Endolymph: Fills the membranous labyrinth (inside the membrane). Chemically identical to intracellular fluid (High K+, Low Na+). Secreted by the highly vascular Stria Vascularis.
Pathology: Ménière Disease is caused by Endolymphatic Hydrops—an overproduction or under-drainage of endolymph that swells the membranous labyrinth, causing episodic vertigo, roaring tinnitus, and low-frequency hearing loss.
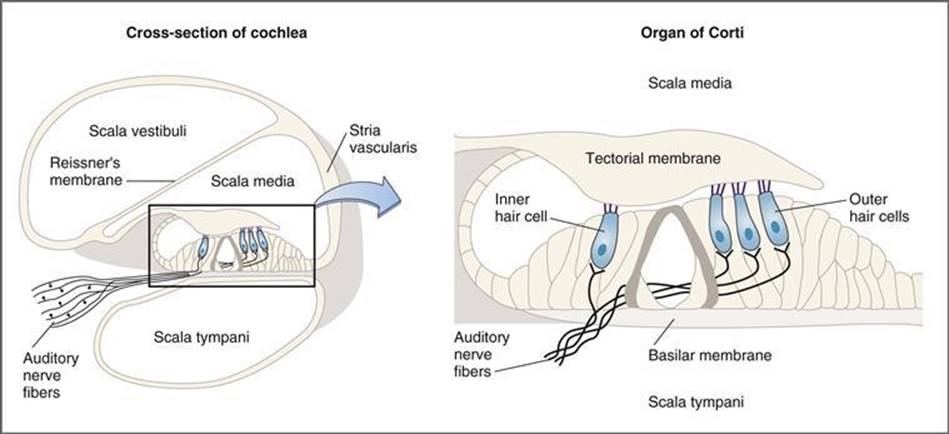
1. The Cochlea & Sound Transduction
A snail-shaped tube with three internal fluid channels. The central triangular channel is the Scala Media (filled with endolymph). The floor of this channel is the flexible Basilar Membrane, which houses the true hearing apparatus: the Organ of Corti.
Tonotopic Organization (The Piano Keyboard)
The basilar membrane acts like an unrolled piano. It is physically stiff and narrow at the BASE of the cochlea (responding only to HIGH frequencies, 20,000 Hz) and wide and floppy at the APEX (responding only to LOW frequencies, 20 Hz). This physically maps sound frequencies to specific nerve fibers.
The Transduction Pathway:
- Sound vibrates the stapes at the oval window, creating a fluid wave in the perilymph.
- The fluid wave physically displaces the basilar membrane up and down.
- This bouncing causes the microscopic hair cells (Inner Hair Cells) of the Organ of Corti to shear and grind against the gelatinous Tectorial Membrane hanging above them.
- This mechanical shearing physically bends the stereocilia on top of the hair cells, popping open mechanically-gated ion channels.
- Potassium (K+) from the endolymph floods into the cell, depolarizing it and firing the auditory nerve (CN VIII), sending the signal to the brainstem, thalamus (Medial Geniculate Nucleus), and finally the primary auditory cortex.
The Round Window Necessity: Fluid is incompressible. If the stapes pushes IN at the oval window, the membrane of the Round Window MUST bulge OUT to release the pressure. Without the round window, the fluid couldn't move, the basilar membrane wouldn't bounce, and we would be deaf!
2. The Vestibular System (Balance)
Detects head position and movement to maintain equilibrium and visual stability.
| Vestibular Organ | Detects | Mechanism & Receptors |
|---|---|---|
| Otolith Organs (Utricle & Saccule) |
Linear Acceleration & Static head tilt (Gravity). (Utricle = horizontal/driving a car. Saccule = vertical/riding an elevator). |
The sensory maculae contain hair cells embedded in jelly topped with heavy calcium crystals (Otoliths). When you accelerate or tilt your head, inertia makes the heavy crystals lag behind, dragging the jelly and bending the hair cells to fire the nerve. |
| Semicircular Canals (Anterior, Posterior, Lateral) |
Angular (Rotational) Acceleration. (Shaking head "yes" or "no", or cartwheels). |
The three canals sit in X, Y, Z planes. When you spin your head, the fluid (endolymph) inside the canal sloshes backwards due to inertia, pushing against a gelatinous sail (the cupula) inside the ampulla, bending the hair cells. |
Clinical Correlate: Benign Paroxysmal Positional Vertigo (BPPV)
The most common cause of vertigo in adults. It occurs when the calcium crystals (otoconia) break loose from the Utricle and accidentally fall into the posterior Semicircular Canal. Now, when the patient rolls over in bed, the heavy crystals roll down the canal, dragging fluid with them, sending a false, violent "spinning" signal to the brain.
Treatment: Cured mechanically in 5 minutes using the Epley Maneuver to physically roll the patient and dump the crystals back out of the canal.
XII. The Facial Nerve (CN VII) - Complete Course
The facial nerve is highly complex, carrying motor, parasympathetic, and special sensory fibers through a tortuous path in the temporal bone.
- Brainstem: Motor fibers originate in the pons, loop completely around the abducens (CN VI) nucleus (creating the facial colliculus bulge in the 4th ventricle), and exit the brainstem.
- Internal Acoustic Meatus: CN VII enters the petrous temporal bone alongside CN VIII.
- Facial Canal & Geniculate Ganglion: Travels through bone. At its sharp bend (the genu), it houses the Geniculate Ganglion (sensory cell bodies). Here, it gives off the Greater Petrosal Nerve (carrying parasympathetic fibers to the lacrimal gland for tears).
- Middle Ear: Descends the posterior wall of the middle ear. Gives off the Nerve to the Stapedius (muscle).
- Chorda Tympani: Branches off and physically crosses the eardrum space. Carries special sensory taste from the anterior 2/3 of the tongue and parasympathetics to the submandibular/sublingual salivary glands.
- Exit: Drops out the bottom of the skull via the Stylomastoid Foramen.
- Parotid Gland & Face: Plunges directly into the Parotid salivary gland (Note: it does NOT innervate the parotid; CN IX does). Inside the gland, it splits into its 5 terminal motor branches to control all muscles of facial expression: Temporal, Zygomatic, Buccal, Marginal Mandibular, and Cervical.
XIII. References & Further Reading
- Moore, K. L., Dalley, A. F., & Agur, A. M. R. (2018). Clinically Oriented Anatomy (8th ed.). Lippincott Williams & Wilkins. (Comprehensive macroscopic and clinical anatomy of the orbit and temporal bone).
- Snell, R. S. (2011). Clinical Anatomy by Regions (9th ed.). Lippincott Williams & Wilkins. (Detailed neural pathways, foramina, and cranial nerve palsies).
- Standring, S. (Ed.). (2020). Gray's Anatomy: The Anatomical Basis of Clinical Practice (42nd ed.). Elsevier. (Exhaustive detail on the membranous labyrinth, cochlear mechanics, and autonomic orbital pathways).
- Kanski, J. J., & Bowling, B. (2015). Clinical Ophthalmology: A Systematic Approach (8th ed.). Saunders. (Pathophysiological correlates including Glaucoma, Horner's Syndrome, and Oculomotor Palsies).