Pelvic Walls & Floor: Comprehensive Anatomy
The pelvic walls and floor form a dynamic, closure-producing partition at the base of the abdominopelvic cavity. They function to support the pelvic viscera against gravity and fluctuations in intra-abdominal pressure, while permitting controlled passage of the gastrointestinal, urinary, and reproductive tracts through specific apertures.
1. Structural Boundaries & Pelvic Walls
The pelvis is essentially a bony ring, lined by muscles and fascia. Understanding its boundaries is the first step in mastering pelvic anatomy.
Anterior Pelvic Wall
The anterior wall is the shallowest boundary of the pelvis. It is primarily formed by:
- Posterior aspects of the pubic bodies: The flat posterior surfaces of the left and right pubic bones.
- Pubic rami: Both the superior and inferior pubic rami contribute to the anterior wall structure.
- Interpubic fibrocartilage disc (pubic symphysis): The secondary cartilaginous joint uniting the two pubic bones anteriorly.
Symphysis Pubis Dysfunction (SPD)
The anterior wall is relatively weak compared to the lateral and posterior walls. During pregnancy, the hormone relaxin causes physiological widening of the pubic symphysis (up to 4-9 mm). If this widening is excessive, it can lead to severe pain and instability, a condition known as symphysis pubis dysfunction.
Posterior Pelvic Wall
The posterior wall is the most extensive boundary, providing the primary structural support and weight transfer for the body.
- Bony sacrum and coccyx: The fused sacral vertebrae (S1-S5) and the terminal coccyx form the central bony framework.
- Sacroiliac (SI) joints: The incredibly strong synovial and fibrous joints linking the auricular surfaces of the sacrum and the ilium.
- Anterior sacroiliac ligaments: Thin ligaments reinforcing the anterior aspect of the SI joints.
- Sacrotuberous ligaments: Broad, robust bands extending from the sacrum to the ischial tuberosity.
- Sacrospinous ligaments: Triangular ligaments running from the sacrum to the ischial spine.
Note: The posterior wall is the strongest and most stable component of the pelvic ring. The SI joints, reinforced by massive interosseous ligaments, are among the strongest joints in the human body, essential for transferring weight from the axial skeleton to the lower limbs.
Lateral Pelvic Walls
The lateral walls form the sides of the pelvic basin and are formed by:
- Internal aspect of the hip bones (os coxae): Specifically the iliac fossa, arcuate line, and the pelvic surface of the hip bone.
- Obturator membrane: A strong fibrous sheet that largely seals the obturator foramen.
- Obturator Canal: A small gap at the superior/anterior part of the obturator foramen. It transmits the obturator nerve, artery, and vein from the pelvis into the medial compartment of the thigh.
- Obturator internus & Piriformis muscles: These form the fleshy padding of the lateral and posterolateral walls.
2. Musculature of the Pelvic Walls
The muscles of the pelvic walls contribute to both pelvic stability and lower limb movement. The two principal muscles—the piriformis and obturator internus—have unique pathways that organize the neurovascular structures exiting the pelvis.
Piriformis Muscle (The Gateway Muscle)
The piriformis serves as a critical anatomical landmark, dividing the greater sciatic foramen into two functional spaces.
- Origin: Anterior surface of sacral segments S2-S4.
- Insertion: Greater trochanter of the femur (superior border).
- Innervation: Branches from the sacral plexus (S1, S2).
- Action: Lateral rotation of the thigh at the hip joint; abduction of the thigh (when the hip is flexed); stabilizes the femoral head in the acetabulum.
- Pathway: Passes laterally out of the pelvis through the greater sciatic foramen. By doing so, it divides this foramen into the suprapiriform (above) and infrapiriform (below) spaces. All structures exiting the greater sciatic foramen must pass either above or below this muscle.
Piriformis Syndrome
When the piriformis muscle becomes tight, hypertrophied, or spasmodic, it can compress the sciatic nerve (which usually passes directly beneath the muscle). This causes deep buttock pain, tingling, and numbness radiating down the posterior thigh and leg. This accounts for approximately 6-8% of all cases of clinical sciatica.
Obturator Internus Muscle (The Lateral Wall Liner)
The obturator internus lines the pelvic surface of the obturator membrane and forms a significant portion of the lateral pelvic wall.
- Origin: Pelvic surface of the obturator membrane and surrounding bony margins.
- Insertion: Medial surface of the greater trochanter (trochanteric fossa) of the femur.
- Innervation: Nerve to obturator internus (L5, S1, S2).
- Action: Lateral rotation of the thigh; stabilizes the hip joint during weight-bearing.
- Pathway: The muscle fibers converge posteriorly, turning at a sharp right angle around the lesser sciatic notch to pass through the lesser sciatic foramen to reach the femur.
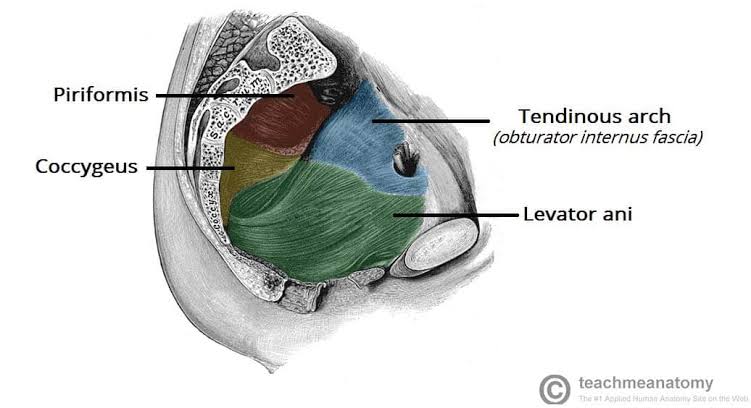
- Tendinous Arch (White Line): The fascia covering the obturator internus thickens along a line running from the pubic body to the ischial spine. This creates the tendinous arch of the levator ani, a critical suspension point/origin for the pelvic floor muscles.
3. The Pelvic Floor (Pelvic Diaphragm)
The pelvic diaphragm is a broad, bowl-shaped muscular partition suspended between the anterior, lateral, and posterior pelvic walls. It supports the pelvic viscera while maintaining continence.
It consists of two paired muscles on each side: the large Levator Ani and the smaller Coccygeus.
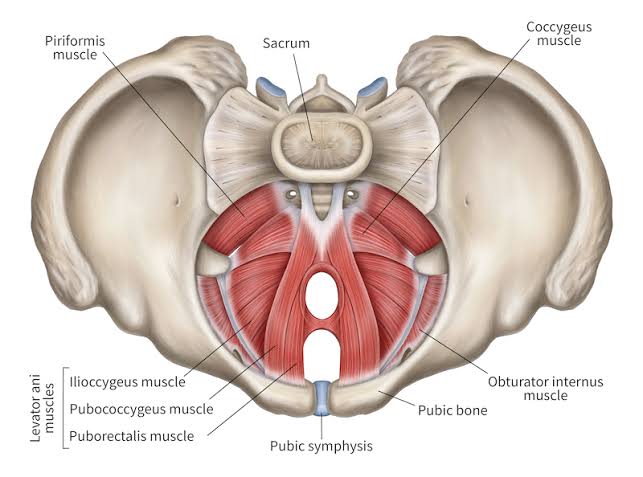
1. Levator Ani Muscle Complex
The levator ani is the largest and most functionally important component of the pelvic floor. It is subdivided into three distinct parts based on their attachments and fiber directions:
- A. Puborectalis (The Fecal Continence Sling):
- The medialmost, thickest subdivision.
- Origin: Posterior surface of the pubic body.
- Insertion: Forms a U-shaped muscular sling around the anorectal junction, merging with its opposite partner.
- Innervation: Branches from S3-S4 (levator ani nerve).
- Function: Maintains the anorectal angle at approximately 80-90 degrees. This acute angle acts as a mechanical flap valve to prevent involuntary passage of stool. During defecation, the puborectalis relaxes, straightening the angle to allow evacuation.
- B. Pubococcygeus (The Main Muscle Bulk):
- The intermediate and largest subdivision.
- Origin: Posterior pubis and anterior portion of the tendinous arch.
- Insertion: Coccyx and the anococcygeal ligament (the midline raphe).
- Function: Provides the main support for the bladder, uterus/vagina, and rectum against increases in intra-abdominal pressure (coughing, lifting). Damage to this muscle during childbirth is the primary cause of pelvic organ prolapse.
- C. Iliococcygeus (The Posterior Sheet):
- The thinnest, most posterior portion.
- Origin: Posterior tendinous arch and ischial spine.
- Insertion: Coccyx and anococcygeal ligament.
- Function: Supports the posterior pelvic floor and contributes to the overall bowl shape.
2. Coccygeus (Ischiococcygeus) Muscle
This is the posterior floor support, lying completely flat against the deep surface of the sacrospinous ligament.
- Origin: Ischial spine.
- Insertion: Lateral margins of the lower sacrum and coccyx.
- Innervation: Branches from S4-S5.
- Relationship: It blends heavily with the sacrospinous ligament; functionally and anatomically, they are virtually inseparable.
Diaphragmatic Apertures (Hiatuses)
The pelvic diaphragm is not a completely sealed sheet; it has two midline gaps to allow tracts to exit the body:
- Urogenital Hiatus: The anterior gap between the medial borders of the pubococcygeus muscles. It allows passage of the urethra (in both sexes) and the vagina (in females). This hiatus is a natural weak point; urethral hypermobility and stress incontinence stem from weakness here.
- Anal Hiatus: The posterior opening through which the anal canal passes. It is guarded by the puborectalis sling.
4. Pelvic Fascia & Spaces
The pelvic fascia is a complex connective tissue system providing structural compartmentalization, organ suspension, and defining surgical planes.
Parietal vs. Visceral Pelvic Fascia
- Parietal Pelvic Fascia: A membranous layer lining the internal surface of the pelvic wall muscles (covering the piriformis and obturator internus). It is continuous superiorly with the transversalis fascia of the abdomen. Its most important specialization is the Tendinous Arch.
- Visceral Pelvic Fascia (Endopelvic Fascia): The adventitial connective tissue that wraps around and invests the pelvic organs (bladder, uterus, vagina, rectum, and prostate).
Fascial Ligaments & Pelvic Support
The endopelvic fascia thickens into condensed, weight-bearing bands that structurally suspend the viscera. Without these, gravity and pressure would push the organs out of the pelvis.
| Ligament | Origin & Insertion | Function |
|---|---|---|
| Pubovesical Ligaments (Female) | Pubic bone → Bladder neck | Supports bladder neck; maintains urethrovesical angle. |
| Puboprostatic Ligaments (Male) | Pubic bone → Prostate capsule | Supports prostate and membranous urethra. |
| Uterosacral Ligaments | Posterolateral Cervix → Sacrum (S2-S4) | Supports the uterus in anteversion; prevents downward uterine descent. |
| Cardinal (Mackenrodt's) Ligaments | Lateral Cervix → Lateral pelvic wall | The primary support of the uterus and upper vagina. |
| Pubocervical Fascia | Pubic bone → Cervix/Anterior vaginal wall | Supports the anterior vaginal wall and bladder base (prevents cystocele). |
| Rectovaginal Fascia | Posterior vaginal wall → Rectal wall | Separates rectum from vagina; supports posterior compartment (prevents rectocele). |
- Level I (Suspension): Uterosacral and cardinal ligaments suspend the uterus/vaginal apex from the pelvic walls.
- Level II (Attachment): Pubocervical and rectovaginal fasciae attach the vagina to the lateral walls.
- Level III (Fusion): Perineal membrane and perineal body fuse the distal vagina and urethra to surrounding structures.
Potential Pelvic Spaces
These are avascular planes between fascial layers. They are normally collapsed but can expand rapidly due to pathology or surgical dissection.
- Retropubic Space (Space of Retzius): Located between the pubic symphysis (anterior) and bladder (posterior). Contains fat and loose tissue. Accessed for incontinence surgeries.
- Paravesical Spaces: Lateral to the bladder. Important landmarks for pelvic lymphadenectomy.
- Rectovesical (Male) / Rectovaginal (Female) Space: Between the rectum and the anterior organ (bladder/prostate or vagina).
- Pararectal Spaces: Lateral to the rectum. Communicates inferiorly with the ischioanal fossae.
Clinical Relevance: These potential spaces can fill massively with blood (Hematoma) following internal iliac trauma, or pus (Abscess) from diverticulitis or pelvic inflammatory disease.
5. Neurovascular Corridors & Relations
The pelvis contains major structures that supply the viscera, perineum, and lower limbs.
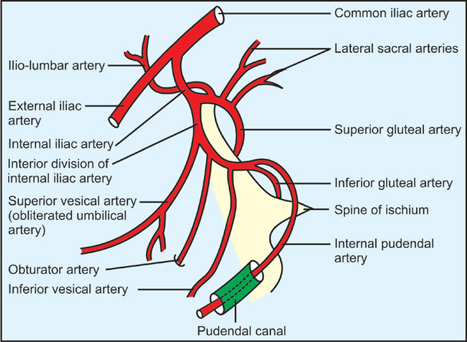
The Internal Iliac Artery
The principal artery of the pelvis. It bifurcates from the common iliac artery at the L5-S1 intervertebral disc and splits into two divisions.
- Anterior Division Branches:
- Umbilical artery: Gives off superior vesical artery (supplies bladder dome).
- Obturator artery: Exits through the obturator canal to the medial thigh.
- Inferior vesical artery (male) / Uterine artery (female).
- Middle rectal artery: Supplies the rectum.
- Internal pudendal artery: Exits the pelvis to supply the perineum via Alcock's canal.
- Inferior gluteal artery: Exits the pelvis via the infrapiriform foramen to supply the gluteus maximus.
- Posterior Division Branches:
- Iliolumbar artery: Ascends to psoas and iliacus muscles.
- Lateral sacral arteries: Supplies the sacrum and sacral canal contents.
- Superior gluteal artery: Exits via the suprapiriform foramen to supply gluteus medius/minimus.
Clinical note: The internal iliac system is the primary source of hemorrhage in pelvic fractures. A fractured pelvis can hide up to 4 liters of blood in the retroperitoneal space. Pelvic angiography with embolization is the definitive treatment.
The Sacral Plexus
Formed by somatic roots (L4-S4), it lies directly on the anterior surface of the piriformis muscle. It provides innervation to the posterior thigh, leg, foot, and perineum.
| Nerve | Roots | Exit Route | Distribution |
|---|---|---|---|
| Sciatic Nerve | L4-S3 | Greater sciatic foramen (Infrapiriform) | Posterior thigh, entire leg and foot. |
| Pudendal Nerve | S2-S4 | Greater sciatic foramen → lesser sciatic foramen → Alcock's canal | Perineum, external genitalia, anal canal (sensory & motor). |
| Superior Gluteal Nerve | L4-S1 | Greater sciatic foramen (Suprapiriform) | Gluteus medius, minimus, tensor fasciae latae. |
| Inferior Gluteal Nerve | L5-S2 | Greater sciatic foramen (Infrapiriform) | Gluteus maximus. |
Pudendal Canal (Alcock's Canal)
This is a fascial tunnel formed by a split in the obturator internus fascia on the lateral wall of the ischioanal fossa. It houses the pudendal nerve and the internal pudendal vessels as they travel from the lesser sciatic foramen to the perineum. It provides crucial sensory innervation to external genitalia and motor control to the external urethral and anal sphincters.
6. Clinical & Applied Anatomy
The structural relationships detailed above are essential for diagnosing and managing pelvic floor dysfunction and performing obstetric/surgical procedures.
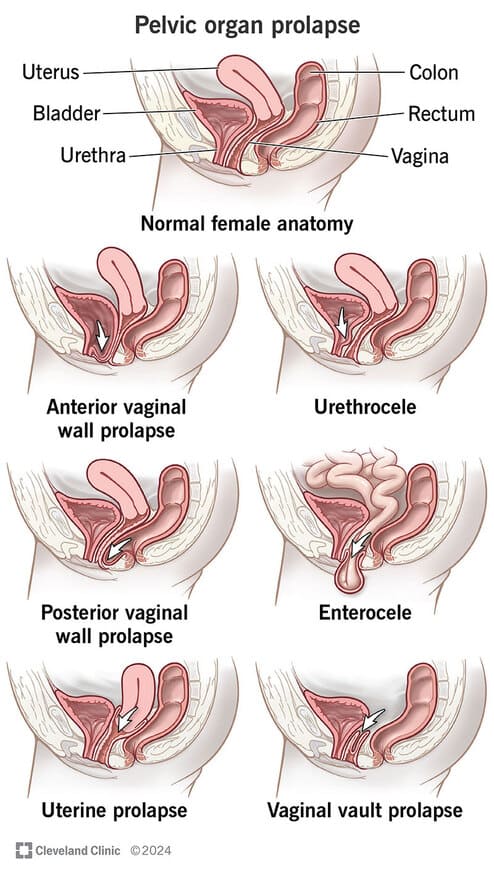
Pelvic Organ Prolapse (POP)
POP results from structural weakness, stretching, or tearing of the levator ani complex (specifically the pubococcygeus) and the endopelvic fascia. The most common etiology is birth trauma during vaginal delivery. Without support, organs herniate downward:
- Cystocele: The bladder descends into the anterior vaginal wall. Caused by a breakdown of the pubocervical fascia. Presents with urinary frequency, urgency, or incontinence.
- Rectocele: The rectum bulges into the posterior vaginal wall. Caused by weakness of the rectovaginal fascia and tearing of the perineal body. Presents with defecatory dysfunction.
- Uterine Prolapse: The uterus descends straight down the vaginal canal. Caused by failure of the uterosacral and cardinal ligaments (Level I support failure).
Risk Factors: Vaginal childbirth (especially prolonged pushing or forceps delivery), chronic increased intra-abdominal pressure (chronic cough, obesity, heavy lifting), aging/menopause (estrogen loss weakens collagen), and connective tissue disorders.
Continence Mechanics
- Fecal Continence: Depends heavily on the puborectalis sling (maintaining the 80-90 degree anorectal angle at rest) and the external anal sphincter (voluntary control via the pudendal nerve).
- Urinary Continence: Maintained by the levator ani elevating the bladder neck during stress, the urethrovesical angle (kept intact by pubovesical ligaments), and external urethral sphincter tone. Stress Urinary Incontinence (SUI) occurs when pubococcygeus weakness causes urethral hypermobility; intra-abdominal pressure forces urine out because the urethra drops below the structural support line.
Episiotomy Considerations
During the second stage of labor, if the perineum does not stretch adequately, a controlled surgical incision (episiotomy) is made to enlarge the vaginal opening and prevent ragged, uncontrolled tearing.
Median vs. Mediolateral Episiotomy
A median (midline) episiotomy cuts straight down toward the anus. While easier to repair, it carries a high risk of extending directly through the perineal body into the external anal sphincter and rectum (causing a 3rd or 4th-degree tear and subsequent fecal incontinence).
A mediolateral episiotomy (cutting at a 45-degree angle away from the midline) is the preferred approach. It directs the incision safely away from the perineal body and levator ani fibers, preserving structural integrity and drastically reducing the risk of severe rectal tearing and future prolapse.
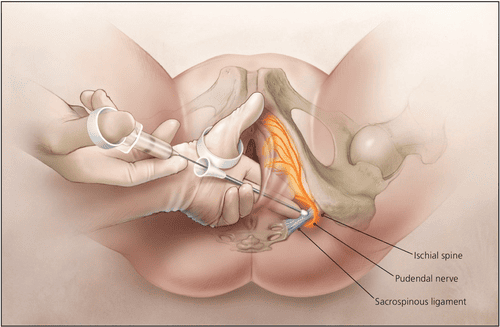
Pudendal Nerve Block
A common regional anesthesia technique used during vaginal delivery and perineal repairs.
- Target Landmark: The ischial spine is the critical bony landmark.
- Technique (Transvaginal): The provider palpates the ischial spine through the lateral vaginal wall. The needle is directed toward the spine, piercing the sacrospinous ligament, and the anesthetic is deposited just as the nerve enters Alcock's canal.
- Effect: Anesthetizes the perineum, vulva/labia, clitoris, and anal canal.
- Complications to Avoid: Intravascular injection (the internal pudendal artery runs right alongside the nerve, requiring aspiration before injecting), rectal perforation (if the needle angles too medially), and massive hematoma formation due to the rich venous plexus.