Pelvic Viscera
Comprehensive and exhaustive notes on the anatomy of the urinary, gastrointestinal, and reproductive systems within the pelvis, including peritoneum and neurovascular supply.
SECTION 01: Urinary System Components
The urinary system within the pelvis comprises the urinary bladder, the pelvic ureters, and the urethra. These structures are closely related to the reproductive organs and share neurovascular supplies, making their anatomy essential for both urological and gynecological practice.
Urinary Bladder
The urinary bladder is a hollow, muscular organ located posterior to the pubic symphysis. When empty, it assumes a pyramid-like shape confined within the pelvis. When distended, it expands superiorly into the abdominal cavity, rising as high as the umbilicus.
Anatomical Parts of the Bladder
- Apex - The pointed anterior part directed toward the pubic symphysis; connected to the median umbilical ligament (remnant of urachus).
- Body - The main central portion between the apex and fundus.
- Fundus (Base) - The posterior wall facing the rectum (male) or anterior vaginal wall (female).
- Neck - The most inferior part surrounding the internal urethral orifice; continuous with the urethra.
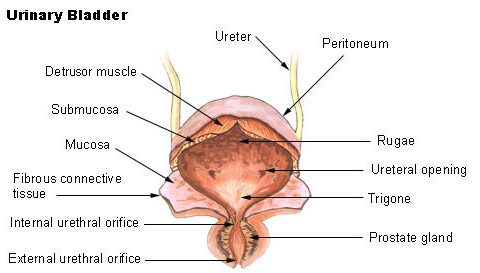
The Trigone of the Bladder
A smooth, triangular area on the internal surface of the bladder base, bounded by:
- Two ureteric orifices (superolateral angles) - The openings where the left and right ureters enter the bladder.
- Internal urethral orifice (inferior angle) - The opening where urine exits into the urethra.
The trigone is smooth (lacks rugae) because it is derived from the mesonephric duct, unlike the rest of the bladder which is endodermal. This makes it an important landmark during cystoscopy.
Muscular Architecture
| Layer | Description | Function |
|---|---|---|
| Detrusor Muscle | Three layers of smooth muscle (inner longitudinal, middle circular, outer longitudinal) | Contracts to expel urine during micturition; relaxed during filling. |
| Internal Urethral Sphincter | Thickened circular smooth muscle at the bladder neck | Involuntary control of urine outflow; prevents retrograde ejaculation in males. |
Pelvic Ureters
The ureters descend from the kidneys, cross the pelvic brim, and course through the pelvis to reach the bladder:
- Cross the pelvic brim anterior to the bifurcation of the common iliac arteries (at the sacroiliac joint level).
- Descend along the lateral pelvic wall, anterior to the internal iliac artery.
- Turn anteromedially to enter the bladder at the trigone.
"Water Under the Bridge"
In females, the ureter passes immediately inferior to the uterine artery (and superior to the vaginal artery) as it approaches the bladder. This relationship is critically important during hysterectomy, as the ureter is at high risk of injury when the uterine artery is ligated.
In males, the ureter passes anterior to the ductus deferens (vas deferens) near the bladder. The ductus deferens crosses the ureter from lateral to medial, then descends posterior to the bladder.
Urethra
Male Urethra (~20 cm)
The male urethra is divided into four distinct parts:
- Preprostatic - Short segment within the bladder neck.
- Prostatic (~3 cm) - Passes through the prostate; contains the urethral crest and seminal colliculus (verumontanum) where the ejaculatory ducts open.
- Membranous (~1 cm) - Passes through the deep perineal pouch (urogenital diaphragm); the narrowest and least dilatable part.
- Spongy/Penile (~15 cm) - Passes through the corpus spongiosum of the penis; the longest part.
Female Urethra (~4 cm)
The female urethra is significantly shorter:
- Extends from the internal urethral orifice to the external urethral orifice.
- Lies anterior to the vagina.
- Embedded within the pubourethral ligaments and surrounded by the external urethral sphincter.
- Its short length contributes to the higher incidence of UTIs in females (bacterial ascent is easier).
SECTION 02: Gastrointestinal System Components
The pelvic gastrointestinal tract comprises the rectum and anal canal. These structures are critical for fecal storage, continence, and controlled defecation. The anal canal is particularly important clinically due to its dual embryological origin and the profound differences in vascular, neural, and lymphatic supply above and below the pectinate line.
Rectum - Definition & Limits
- Beginning: At the level of the S3 vertebra, as a continuation of the sigmoid colon.
- Termination: At the anorectal junction, where it pierces the levator ani muscle (puborectalis sling).
- Length: Approximately 12-15 cm.
- Shape: Follows the sacral curve; not straight despite its name ("rectum" = "straight" in Latin).
Three Lateral Curvatures (Valves of Houston)
The rectum has three lateral flexures with corresponding internal mucosal folds:
- Superior flexure - Convex to the right (at the level of S3).
- Middle flexure - Convex to the left (at the level of the sacral promontory).
- Inferior flexure - Convex to the right (at the level of the tip of the coccyx).
The rectum lacks the characteristic features of the colon:
- No taeniae coli (three longitudinal muscle bands).
- No haustra (sacculations between taeniae).
- No omental appendices (fatty tags on the serosal surface).
Instead, the rectum has a relatively uniform outer longitudinal muscle layer.
Anal Canal
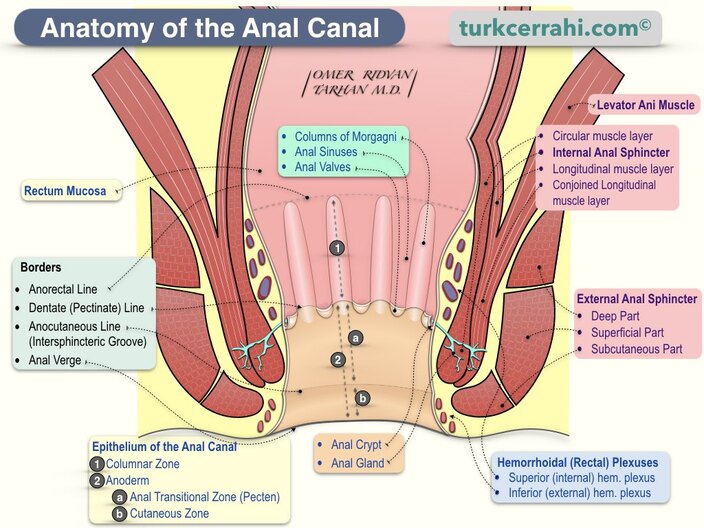
The Pectinate (Dentate) Line
The pectinate line marks the division between the upper visceral (endodermal) and lower somatic (ectodermal) origins of the anal canal. It is formed by the anal valves and represents the junction between the hindgut and proctodeum. This line is the most important anatomical landmark in the anal canal.
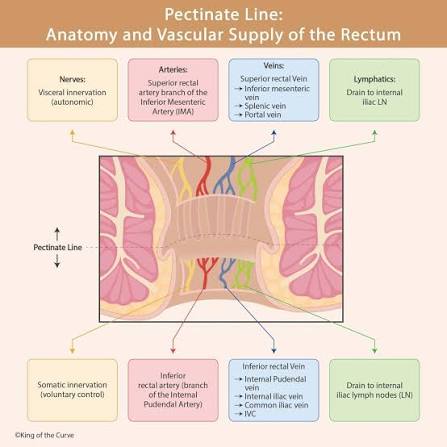
| Feature | Above Pectinate Line | Below Pectinate Line |
|---|---|---|
| Embryological Origin | Endoderm (hindgut) | Ectoderm (proctodeum) |
| Epithelium | Columnar (mucosa) | Squamous (skin) |
| Arterial Supply | Superior rectal artery (branch of IMA) | Inferior rectal artery (branch of internal pudendal) |
| Venous Drainage | Superior rectal vein → inferior mesenteric vein → portal system | Inferior rectal vein → internal pudendal vein → systemic (IVC) |
| Lymphatic Drainage | Internal iliac lymph nodes | Superficial inguinal lymph nodes |
| Innervation | Autonomic (visceral) - no pain sensation | Somatic (pudendal nerve) - pain sensitive |
| Hemorrhoids | Internal hemorrhoids (painless, bright red bleeding) | External hemorrhoids (painful, thrombosed) |
Mucosal Features
Above the Pectinate Line:
- Anal columns (of Morgagni) - 5-10 longitudinal mucosal folds.
- Anal valves - Semilunar mucosal folds connecting the lower ends of adjacent columns.
- Anal sinuses - Small pockets above the valves that receive anal glands.
- Anal glands - Open into the sinuses; can become infected (anal abscess, fistula).
Below the Pectinate Line:
- Anal pecten - A smooth, pale, hairless zone (transitional epithelium).
- Anocutaneous line (intersphincteric groove) - The boundary between the pecten and true skin.
- Anal verge - The true cutaneous margin of the anus. Contains sebaceous glands and hair follicles (true skin).
Muscular Architecture
| Sphincter | Type | Innervation | Function |
|---|---|---|---|
| Internal Anal Sphincter | Smooth muscle (thickened circular layer of rectum) | Autonomic (sympathetic: L1-L2; parasympathetic: S2-S4) | Involuntary tone; maintains continence at rest (~70% of resting pressure). |
| External Anal Sphincter | Skeletal muscle (three parts: deep, superficial, subcutaneous) | Pudendal nerve (S2-S4) | Voluntary control; provides additional squeeze pressure. |
SECTION 03: Male Reproductive System Viscera
The male reproductive viscera within the pelvis include the prostate gland, seminal vesicles, ejaculatory ducts, and the pelvic portion of the ductus deferens. These structures are intimately related to the urinary bladder and rectum.
Prostate Gland
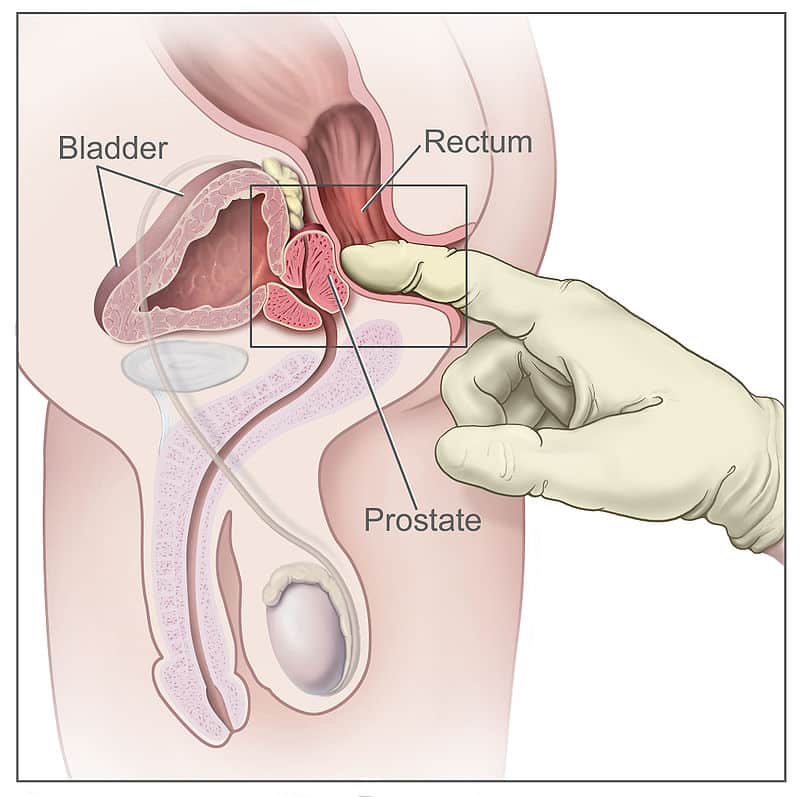
The prostate is a fibromuscular glandular organ situated inferior to the bladder neck and anterior to the rectum. This posterior location makes it palpable via digital rectal examination (DRE) — a critical diagnostic tool for prostate disease.
Prostate Dimensions & Relations
- Size: Approximately 3 cm (base-to-apex), 4 cm (width), 2 cm (anteroposterior).
- Weight: ~20 g in young adults.
- Anterior: Pubic symphysis (separated by retropubic space).
- Posterior: Rectum (separated by rectovesical fascia/Denonvilliers' fascia).
- Superior: Bladder neck and ureteric orifices.
- Inferior: Urogenital diaphragm and external urethral sphincter.
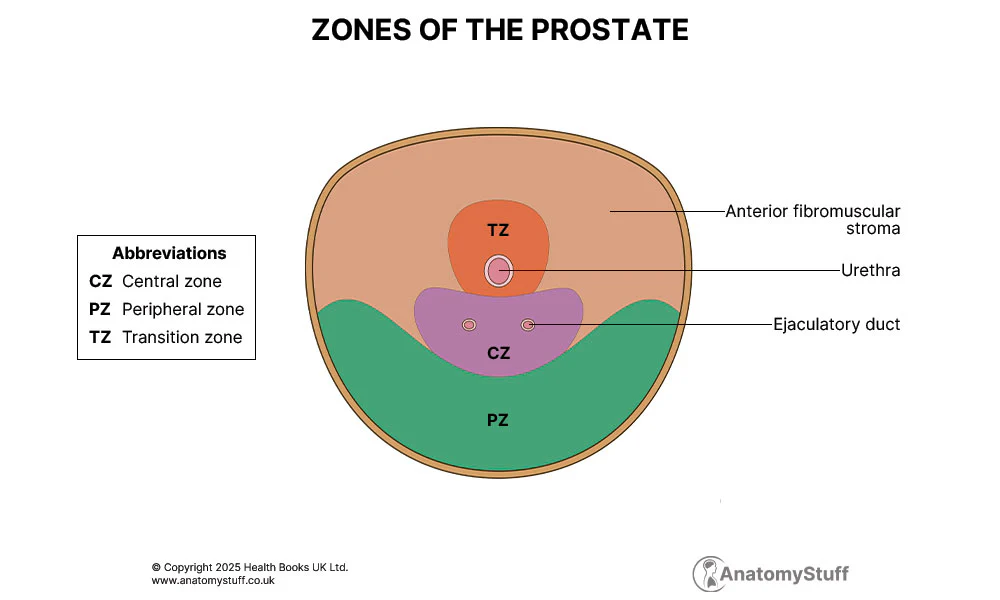
Prostate Zones (McNeal Classification)
| Zone | Description | Clinical Significance |
|---|---|---|
| Peripheral Zone (PZ) | ~70% of glandular tissue; Posterior and lateral. | Site of 70-80% of prostate cancers; Palpable on DRE. |
| Central Zone (CZ) | ~25% of glandular tissue; Surrounds ejaculatory ducts. | Rarely involved in cancer; Extends to base of prostate. |
| Transition Zone (TZ) | ~5% of glandular tissue; Surrounds proximal urethra. | Site of benign prostatic hyperplasia (BPH); Not palpable on DRE. |
| Anterior Fibromuscular Stroma | Non-glandular tissue; Smooth muscle and collagen. | Covers anterior surface; No secretory function. |
Prostate Lobes (Traditional Description)
| Lobe | Location | Clinical Correlation |
|---|---|---|
| Anterior | Anterior to urethra | Fibromuscular; site of benign prostatic hyperplasia (BPH). |
| Posterior | Posterior to urethra and ejaculatory ducts | Palpable on DRE; common site of carcinoma. |
| Median | Between ejaculatory ducts | Contains urethral crest and seminal colliculus. |
| Lateral | On either side of urethra | Contains most of the glandular tissue. |
Seminal Vesicles (Glands)
- Location: Posterior to the bladder fundus, superior to the prostate.
- Structure: Paired, coiled, tubular glands (~5 cm long, but highly convoluted).
- Function: Produce ~60% of seminal fluid volume; rich in fructose, prostaglandins, and fibrinogen.
- Duct: Each seminal vesicle joins the ductus deferens to form the ejaculatory duct.
Ejaculatory Ducts
Formed by the union of the ductus deferens (vas deferens) and the duct of the seminal vesicle. Each ejaculatory duct is approximately 2 cm long and passes through the prostate gland to terminate on the seminal colliculus (verumontanum) in the prostatic urethra. The ducts convey both sperm (from the testes via the ductus deferens) and seminal fluid (from the seminal vesicles).
Ductus (Vas) Deferens
Pelvic Course of the Ductus Deferens
- Enters the pelvis through the deep inguinal ring.
- Descends along the lateral pelvic wall, looping over the inferior epigastric vessels.
- Crosses the ureter anteriorly ("water under the bridge" relationship in reverse).
- Passes posterior to the bladder to reach the seminal vesicle.
- Joins the duct of the seminal vesicle to form the ejaculatory duct.
During vasectomy (male sterilization), the ductus deferens is ligated and divided in the scrotal portion (superficial to the scrotal skin). The pelvic portion remains intact. Sperm production continues but sperm are reabsorbed in the epididymis.
SECTION 04: Female Reproductive System Viscera
The female reproductive viscera within the pelvis include the uterus, ovaries, uterine (fallopian) tubes, and vagina. These structures are arranged in the midline and are intimately related to the urinary bladder anteriorly and the rectum posteriorly.
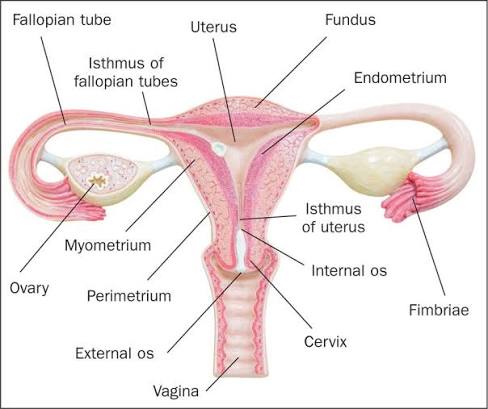
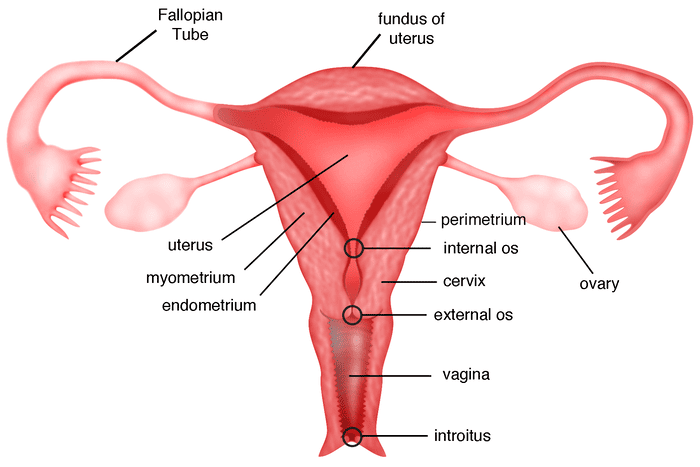
Uterus
Uterine Subdivisions
- Fundus - The rounded superior portion above the openings of the uterine tubes.
- Body - The main central portion between the fundus and isthmus.
- Isthmus - The narrow, constricted region between the body and cervix.
- Cervix - The inferior, cylindrical part projecting into the vagina:
- Internal os - Opening between uterine cavity and cervical canal.
- Cervical canal - The passageway through the cervix.
- External os - Opening of cervical canal into the vagina.
Uterine Position
- Anteverted: The uterus is angled forward relative to the vagina (the long axis of the uterus forms an angle of ~90 degrees with the long axis of the vagina). This is the normal anatomical position in ~80% of women.
- Anteflexed: The uterus is bent forward at the isthmus (the body is flexed anteriorly on the cervix). This is the normal position and is important for sperm transport and early pregnancy implantation.
- Retroverted Uterus: In ~20% of women, the uterus is retroverted (tilted backward) and/or retroflexed (bent backward). This is usually asymptomatic but can be associated with deep dyspareunia (pain during intercourse), back pain during menstruation, difficulty conceiving (controversial), and increased risk of incarceration during early pregnancy.
Uterine Wall Layers
| Layer | Name | Description | Function |
|---|---|---|---|
| Outer | Perimetrium | Serous layer (visceral peritoneum) | Covers most of the uterus except the cervix and lateral portions. |
| Middle | Myometrium | Thick layer of smooth muscle; thickest in the fundus | Contracts during labor and menstruation; contains spiral arteries. |
| Inner | Endometrium | Mucosal lining; functional and basal layers | Site of implantation; shed during menstruation. |
Ovaries
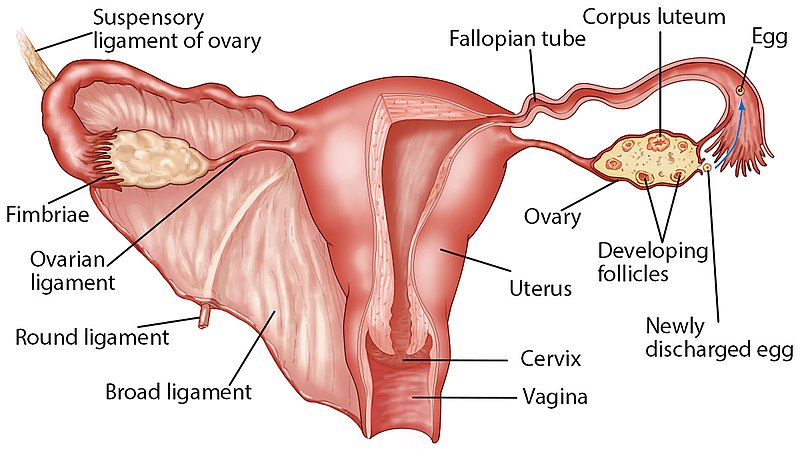
Ovarian Anatomy
- Location: In the ovarian fossa on the lateral pelvic wall (depression on the external iliac vessels, bounded by the ureter and obliterated umbilical artery).
- Shape: Almond-shaped; ~3-5 cm long, 2-3 cm wide, 1-2 cm thick.
- Function: Production of ova (oogenesis) and secretion of estrogen and progesterone.
Ovarian Ligaments
| Ligament | Origin | Insertion | Contents |
|---|---|---|---|
| Ligament of the Ovary | Uterine pole of ovary | Lateral angle of uterus (below uterine tube) | Ovarian branch of uterine artery. |
| Suspensory Ligament of the Ovary | Superior pole of ovary | Lateral pelvic wall | Ovarian vessels (artery, vein, lymphatics), ovarian plexus nerves. |
The suspensory ligament of the ovary is not a true ligament but a peritoneal fold containing the ovarian vessels. During oophorectomy (ovarian removal), this fold must be carefully ligated to prevent bleeding from the ovarian artery (a direct branch of the abdominal aorta).
Uterine (Fallopian) Tubes
The uterine tubes are paired muscular tubes that transport the ovum from the ovary to the uterine cavity. They are divided into four parts from lateral to medial:
| Part | Description | Clinical Significance |
|---|---|---|
| Infundibulum | Funnel-shaped lateral end with fimbriae (finger-like projections) that capture the ovum | Fimbriae must be mobile and patent for ovum capture; adhesions cause infertility. |
| Ampulla | Widest, longest, and most tortuous portion; ~2/3 of tube length | Primary site of fertilization; most common site of ectopic pregnancy. |
| Isthmus | Narrow, straight portion adjacent to the uterus | Common site for tubal ligation (sterilization). |
| Uterine/Intramural Part | Passes through the uterine wall; opens into uterine cavity | Site of tubal patency testing (hysterosalpingography). |
Implantation of the fertilized ovum outside the uterine cavity occurs in ~1-2% of pregnancies. The ampulla of the uterine tube is the most common site (~80%). Risk factors include: previous tubal surgery, pelvic inflammatory disease (PID), endometriosis, and assisted reproductive technology. Rupture can cause life-threatening hemorrhage into the peritoneal cavity.
Vagina
Vaginal Anatomy
- Definition: A fibromuscular canal extending from the cervix to the vestibule of the vagina.
- Length: ~7-10 cm along anterior wall; ~9-12 cm along posterior wall.
- Orientation: Directed posterosuperiorly, forming an angle with the cervix.
- Walls: Normally in apposition (collapsed); highly distensible.
Vaginal Fornices (Recesses)
The vagina surrounds the cervix, creating recesses called fornices:
- Anterior fornix - Between anterior vaginal wall and cervix; related to bladder base.
- Posterior fornix - Between posterior vaginal wall and cervix; in close relation to the rectouterine pouch (Pouch of Douglas).
- Two lateral fornices - On either side of the cervix; related to ureters and uterine vessels.
The posterior vaginal fornix is the most dependent part of the female peritoneal cavity. It is directly accessible transvaginally and is used for:
- Culdocentesis - Aspiration of fluid (blood, pus) from the Pouch of Douglas.
- Transvaginal ultrasound - Optimal window for visualizing pelvic structures.
- Posterior colpotomy - Surgical access to the peritoneal cavity.
SECTION 05: Peritoneal Arrangements & Pelvic Pouches
The pelvic peritoneum reflects over the pelvic organs to form dynamic blind pouches (cul-de-sacs) that are clinically significant as sites of fluid accumulation, surgical access, and pathological spread. The arrangement differs between males and females due to the presence of the uterus.
Pelvic Pouches
Female Pelvic Pouches
- Vesicouterine Pouch: Between the bladder and uterus. Formed by the peritoneal reflection from the bladder dome onto the anterior uterine wall. It is shallow and has limited clinical significance.
- Rectouterine Pouch (Pouch of Douglas): Between the uterus and rectum. The lowest point of the female peritoneal cavity. Fluid, blood, or pus accumulates here due to gravity. Directly accessible via the posterior vaginal fornix.
Male Pelvic Pouch
- Rectovesical Pouch: Between the bladder and rectum. The lowest point of the male peritoneal cavity. In males, there is only one major pouch because the uterus is absent. The peritoneum reflects directly from the bladder to the rectum. This pouch is the site of fluid accumulation in males (e.g., ascites, hemoperitoneum). It is not directly accessible without surgical intervention, unlike the female Pouch of Douglas.
The Pouch of Douglas is the most dependent part of the peritoneal cavity in females. It is the first site to accumulate:
- Blood - Ruptured ectopic pregnancy, hemorrhagic ovarian cyst.
- Pus - Pelvic inflammatory disease (PID), ruptured appendicitis.
- Fluid - Ascites, ovarian cancer (pseudo-Meigs syndrome).
- Endometrial implants - Endometriosis commonly affects this pouch.
Culdocentesis (needle aspiration through the posterior vaginal fornix) can diagnose hemoperitoneum in suspected ectopic pregnancy with ~85% accuracy.
The Broad Ligament
Broad Ligament of the Uterus
A double fold of peritoneum that drapes over the uterus and uterine tubes like a mesentery. It extends from the lateral pelvic walls to the uterus and contains several important structures within its folds. Despite its name, it is not a true ligament (it does not provide mechanical support) but rather a peritoneal fold.
- Mesometrium - The largest part of the broad ligament; extends from the lateral pelvic wall to the body of the uterus. Contains the uterine vessels and the ureter as it passes under the uterine artery.
- Mesosalpinx - The upper free edge of the broad ligament that suspends the uterine tube. Contains the ovarian vessels and nerves as they course toward the ovary.
- Mesovarium - The posterior part of the broad ligament that suspends the ovary. Contains the ovarian vessels as they enter the suspensory ligament. The ovary is attached to the broad ligament by this peritoneal fold.
Contents of the Broad Ligament
The broad ligament contains several important structures in its folds:
- Uterine vessels (artery and vein) - In the base of the broad ligament.
- Ureter - Passes under the uterine artery ("water under the bridge").
- Ovarian vessels - In the suspensory ligament and mesovarium.
- Round ligament of the uterus - Runs from the uterine fundus to the labia majora.
- Ligament of the ovary - Connects ovary to uterus.
- Nerves and lymphatics - Autonomic and sensory fibers.
SECTION 06: Neurovascular Supply & Lymphatics
The pelvic viscera receive their blood supply from the internal iliac artery and its branches, with important contributions from the inferior mesenteric and ovarian arteries. Venous drainage occurs through extensive plexuses, while autonomic innervation governs visceral function. Lymphatic drainage follows arterial pathways to pelvic and para-aortic nodes.
Arterial Supply
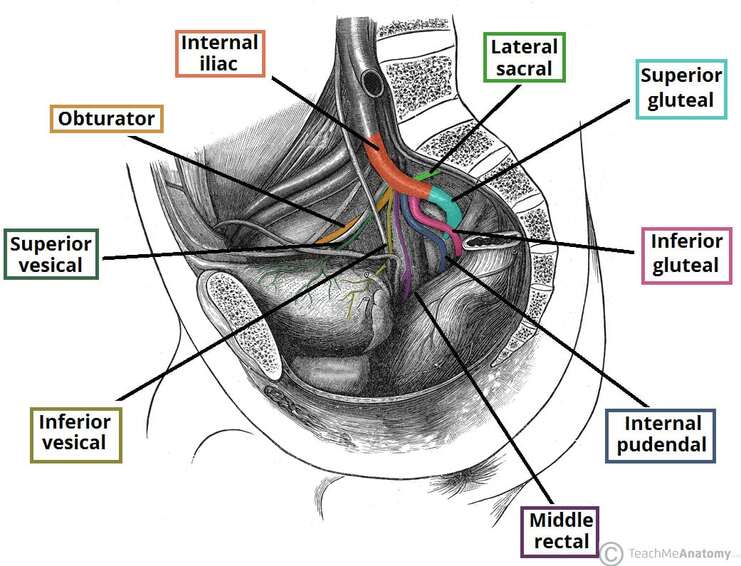
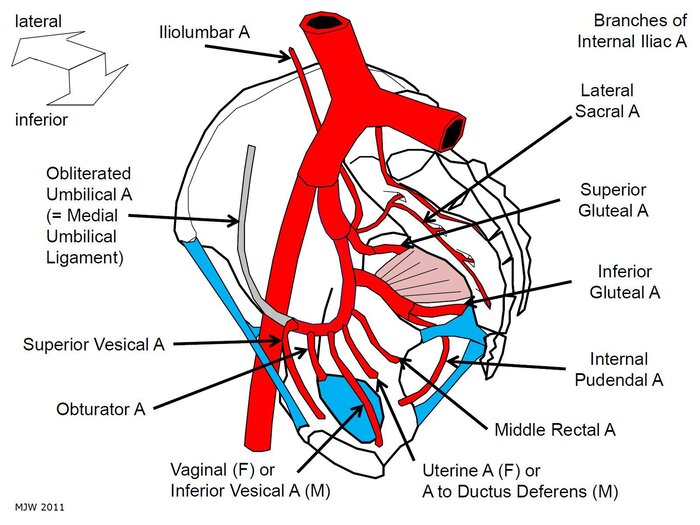
Visceral Branches of the Internal Iliac Artery
| Branch | Origin | Distribution | Clinical Note |
|---|---|---|---|
| Superior Vesical Artery | Anterior division (often from umbilical) | Superior bladder, ureteric orifices, ductus deferens | Supplies bladder dome; may arise from umbilical artery. |
| Inferior Vesical Artery (male) | Anterior division | Bladder base, prostate, seminal vesicle | Enlarged in BPH; embolization target for prostate hemorrhage. |
| Vaginal Artery (female) | Anterior division | Vagina, bladder base, rectum | Homologous to inferior vesical artery. |
| Uterine Artery | Anterior division | Uterus, cervix, vagina, uterine tube, medial ovary | Crosses ureter superiorly ("water under the bridge"). |
| Middle Rectal Artery | Anterior division | Middle and lower rectum, seminal vesicle, prostate | Supplies rectum above pectinate line; anastomoses with superior and inferior rectal arteries. |
| Internal Pudendal Artery | Anterior division | Perineum, external genitalia, erectile tissues, anal canal | Exits via greater sciatic foramen; enters Alcock's canal. |
Extra-Pelvic Arterial Sources
- Superior Rectal Artery: Branch of the inferior mesenteric artery (IMA). Descends into the pelvis to supply the upper rectum and anal canal above the pectinate line. It is the terminal branch of the IMA and anastomoses with the middle and inferior rectal arteries.
- Ovarian Artery: Arises directly from the abdominal aorta (below the renal arteries). Descends in the suspensory ligament of the ovary to supply the ovary, uterine tube, and fundus of the uterus. It anastomoses with the uterine artery in the broad ligament.
Venous Drainage
The pelvic viscera drain through extensive venous plexuses that form a rich anastomotic network:
| Plexus | Location | Drainage | Clinical Significance |
|---|---|---|---|
| Vesical Plexus | Around bladder base and neck | Internal iliac veins | Can be a source of hemorrhage during bladder surgery. |
| Prostatic Plexus (male) | Between prostatic capsule and fascia | Internal iliac veins | Site of significant bleeding during prostatectomy. |
| Uterine/Vaginal Plexus | Along uterine and vaginal walls | Internal iliac veins | Enlarged during pregnancy; varices can develop. |
| Rectal Plexus | Surrounding rectum | Superior rectal vein (portal) + middle/inferior rectal veins (systemic) | Portocaval anastomosis — portal hypertension causes hemorrhoids. |
Portocaval Anastomosis at the Rectum
The rectal venous plexus is a critical portocaval anastomosis:
- Above pectinate line: Superior rectal vein → inferior mesenteric vein → portal vein.
- Below pectinate line: Inferior rectal vein → internal pudendal vein → internal iliac vein → IVC (systemic).
In portal hypertension (e.g., cirrhosis), blood is shunted into systemic veins, causing dilation of the rectal veins — internal hemorrhoids. These are typically painless (visceral innervation) but can cause significant bleeding.
Innervation
Inferior Hypogastric Plexus
The pelvic viscera receive autonomic innervation via the inferior hypogastric plexus, a network of sympathetic and parasympathetic fibers located on the lateral pelvic wall, lateral to the rectum and posterior to the bladder.
| Fiber Type | Origin | Pathway | Function |
|---|---|---|---|
| Sympathetic | L1-L2 spinal cord segments | Descends via lumbar splanchnic nerves → superior hypogastric plexus → hypogastric nerves → inferior hypogastric plexus | Inhibits bladder detrusor; contracts internal urethral sphincter; vasoconstriction; ejaculation. |
| Parasympathetic | S2-S4 spinal cord segments (pelvic splanchnic nerves) | Arises directly from sacral spinal nerves; joins inferior hypogastric plexus | Contracts bladder detrusor; relaxes internal urethral sphincter; erection (vasodilation); defecation. |
Pelvic Splanchnic Nerves (Nervi Erigentes)
The pelvic splanchnic nerves (S2-S4) are the primary parasympathetic supply to the pelvic viscera. They are critical for:
- Bladder contraction during micturition.
- Penile/clitoral erection (vasodilation of erectile tissues).
- Defecation (rectal contraction and internal sphincter relaxation).
Damage to these nerves (e.g., during radical prostatectomy, abdominoperineal resection, or spinal cord injury) can cause urinary retention, erectile dysfunction, and fecal incontinence.
Lymphatic Drainage
Lymphatic drainage of the pelvic viscera follows the arterial supply to regional lymph nodes:
| Organ | Primary Lymph Nodes | Secondary/Terminal Nodes |
|---|---|---|
| Bladder | External iliac, internal iliac | Common iliac → para-aortic |
| Prostate | Internal iliac, obturator | Common iliac → para-aortic |
| Uterus | Internal iliac, external iliac, obturator | Common iliac → para-aortic |
| Vagina (upper) | Internal iliac, external iliac | Common iliac |
| Vagina (lower) | Superficial inguinal | External iliac |
| Rectum (upper) | Internal iliac, superior rectal | Inferior mesenteric → para-aortic |
| Rectum (lower) | Internal iliac, superficial inguinal | Common iliac |
| Ovaries / Testes | Lumbar (aortic) nodes | Para-aortic |
The ovaries and testes have a unique lymphatic drainage pattern. They drain directly to the lumbar (para-aortic) lymph nodes at the level of L1-L2, following the gonadal vessels. This is because the gonads develop in the retroperitoneum and descend to their final positions, carrying their lymphatic drainage with them. This explains why ovarian and testicular cancers can present with retroperitoneal lymphadenopathy before pelvic node involvement.
SECTION 07: Clinical & Applied Anatomy
The anatomy of the pelvic viscera has profound clinical implications in diagnosis, surgery, and disease management. Understanding the spatial relationships, embryological origins, and vascular/lymphatic patterns is essential for clinical practice.
Digital Rectal Examination (DRE)
Digital rectal examination is a fundamental clinical skill that allows palpation of structures adjacent to the anterior rectal wall.
- In Males: Prostate & Seminal Vesicles.
- In Females: Cervix & Vaginal Wall.
- Both Sexes: Rectal Wall & Pelvic Masses.
Male DRE Findings:
- Prostate gland - Palpable through the anterior rectal wall; normal size ~20 g, smooth, rubbery consistency with a central sulcus.
- Prostate cancer - Hard, irregular, asymmetrical nodule (typically in the peripheral/posterior zone).
- Benign prostatic hyperplasia (BPH) - Smooth, symmetrical enlargement; median groove may be obliterated.
- Seminal vesicles - Normally not palpable; enlarged in seminal vesiculitis or obstruction.
Female DRE Findings:
- Cervix - Palpable through the anterior rectal wall; firm, round structure.
- Vaginal wall - Anterior to the rectum; can assess for rectocele.
- Uterus - May be palpable if retroverted.
- Adnexal masses - Ovarian cysts or tumors may be palpable laterally.
Pouch of Douglas Pathology & Culdocentesis
Culdocentesis: The Pouch of Douglas (rectouterine pouch) is the most dependent part of the female peritoneal cavity. It is directly accessible transvaginally via the posterior vaginal fornix.
- Indications: Suspected ruptured ectopic pregnancy, hemoperitoneum, pelvic abscess.
- Technique: A needle is inserted through the posterior vaginal fornix into the Pouch of Douglas.
- Findings: Non-clotting blood suggests hemoperitoneum; pus indicates pelvic infection; clear fluid is normal.
With the advent of high-resolution transvaginal ultrasound, culdocentesis is now less commonly performed, but it remains a valuable bedside diagnostic tool in resource-limited settings.
Benign Prostatic Hyperplasia (BPH) vs. Prostate Cancer
Benign Prostatic Hyperplasia (BPH)
- Origin: Arises from the transition zone (TZ) and periurethral glands.
- Pathophysiology: Nodular enlargement of glandular and stromal tissue around the urethra.
- Symptoms: Early urinary symptoms due to urethral compression — frequency, urgency, nocturia, weak stream, hesitancy, urinary retention.
- DRE: Smooth, symmetrical, rubbery enlargement; median groove preserved.
- PSA: Mildly elevated (usually < 10 ng/mL).
- Treatment: Alpha-blockers, 5-alpha-reductase inhibitors, surgery (TURP).
Prostate Adenocarcinoma
- Origin: Arises from the peripheral zone (PZ) — posterior and posterolateral.
- Pathophysiology: Malignant transformation of glandular epithelium; often multifocal.
- Symptoms: Typically asymptomatic in early stages because the tumor grows away from the urethra.
- DRE: Hard, irregular, asymmetrical nodule; loss of median groove; fixed to surrounding tissues.
- PSA: Significantly elevated (> 10 ng/mL, often much higher).
- Treatment: Radical prostatectomy, radiation, hormone therapy, chemotherapy.
BPH arises in the transition zone, which surrounds the prostatic urethra. Even small nodules compress the urethra, causing obstructive symptoms. Prostate cancer arises in the peripheral zone, which is posterior and away from the urethra. Tumors can grow large without causing urinary symptoms, which is why many prostate cancers are detected by elevated PSA or abnormal DRE before symptoms develop.
Spread of Rectal Malignancy
The pectinate line is the critical landmark that determines the pattern of metastatic spread in rectal cancer:
| Parameter | Above Pectinate Line | Below Pectinate Line |
|---|---|---|
| Lymphatic Spread | Internal iliac lymph nodes → common iliac → para-aortic | Superficial inguinal lymph nodes → external iliac |
| Venous Spread | Superior rectal vein → inferior mesenteric vein → portal vein → liver | Inferior rectal vein → internal pudendal → internal iliac → IVC → lungs |
| Primary Metastatic Site | Liver (via portal system) | Lungs (via systemic circulation) |
| Tumor Type | Adenocarcinoma (columnar epithelium) | Squamous cell carcinoma (squamous epithelium) |
Rectal cancers above the pectinate line (the vast majority) metastasize to the liver first because they drain via the portal system. This is why liver imaging (CT, MRI) is essential in staging rectal cancer. Cancers below the pectinate line (anal canal cancers) metastasize to the lungs first because they drain via the systemic circulation. This difference in metastatic pattern directly influences staging workup and surveillance protocols.
APPENDIX: Quick Reference Table
| Structure | Key Feature / Function | Clinical Relevance |
|---|---|---|
| Bladder Trigone | Smooth triangular area between ureteric and urethral orifices | Landmark for cystoscopy; no rugae. |
| Ureter (female) | Passes under uterine artery ("water under the bridge") | At risk during hysterectomy. |
| Pectinate Line | Divides visceral (endodermal) from somatic (ectodermal) anal canal | Determines vascular, neural, lymphatic supply. |
| Internal Hemorrhoids | Above pectinate line; visceral innervation (painless) | Bleed bright red; portal system drainage. |
| External Hemorrhoids | Below pectinate line; somatic innervation (painful) | Thrombosed; systemic drainage. |
| Prostate Peripheral Zone | 70% of gland; posterior location | Site of 70-80% prostate cancers; palpable on DRE. |
| Prostate Transition Zone | 5% of gland; surrounds urethra | Site of BPH; not palpable on DRE. |
| Uterine Tube Ampulla | Widest portion; 2/3 of tube length | Primary site of fertilization and ectopic pregnancy. |
| Pouch of Douglas | Lowest point of female peritoneal cavity | Fluid accumulation; culdocentesis access. |
| Broad Ligament | Peritoneal fold containing uterine vessels and ureter | "Water under the bridge" relationship. |
| Portocaval Anastomosis | Rectal plexus connects portal and systemic veins | Portal hypertension causes internal hemorrhoids. |
| Pelvic Splanchnic Nerves | S2-S4; parasympathetic to pelvic viscera | Bladder contraction, erection, defecation. |
| Ovarian Lymphatics | Drain to lumbar (para-aortic) nodes | Ovarian cancer spreads to retroperitoneum first. |
Key Concepts to Remember
- The pectinate line is the most important landmark in the anal canal.
- Above the line = visceral (autonomic, portal, internal iliac nodes).
- Below the line = somatic (pudendal nerve, systemic, inguinal nodes).
- The prostate is palpable on DRE because it lies anterior to the rectum.
- The Pouch of Douglas is the lowest point of the female peritoneal cavity.
- The ampulla of the uterine tube is the most common site of fertilization.
- BPH arises from the transition zone (around urethra) → early symptoms.
- Prostate cancer arises from the peripheral zone (posterior) → late symptoms.
- Rectal cancer above pectinate line metastasizes to liver (portal system).
- Rectal cancer below pectinate line metastasizes to lungs (systemic).
- Culdocentesis accesses the Pouch of Douglas via posterior vaginal fornix.
- Ovarian/testicular lymphatics drain to para-aortic nodes (not pelvic).