The Spleen
The spleen is a vital secondary lymphoid organ located in the upper left quadrant of the abdomen, playing crucial roles in immune surveillance and blood filtration.
Anatomical Summary ("Odd Numbers Rule of 1,3,5,7,9,11"):
This mnemonic is a useful way to remember key splenic facts:
- 1 inch thick, 3 inches wide, 5 inches long.
- Weighs approximately 7 ounces (approx. 200 grams).
- Lies between the 9th and 11th ribs.
- Development: Of mesodermal origin, similar to blood components it processes.
- Shape: Often described as having the size and shape of a clenched fist.
- Borders: Typically has an anterior notched border.
Location and Relations:
- Location: Intraperitoneal organ situated in the left upper part of the abdomen, in the left hypochondrium.
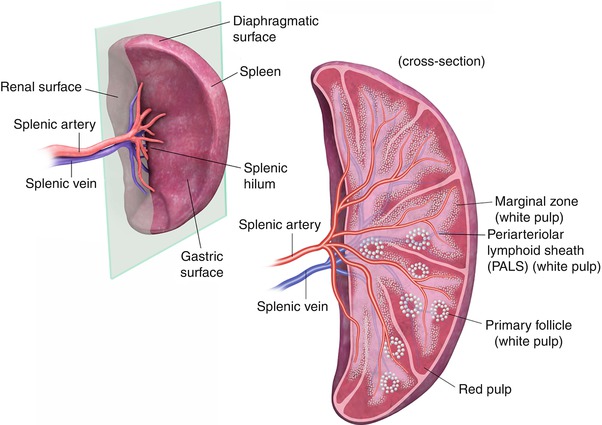
- Diaphragmatic Surface: Convex and smooth, molded to the concavity of the diaphragm.
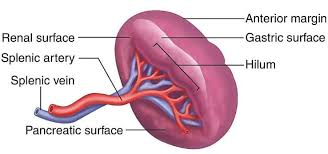
- Visceral Surface: Irregular, with impressions from adjacent organs.
- Hilum: Located on the visceral surface, usually between the stomach and the left kidney impressions.
- Long Axis: Lies along the line of the 10th rib.
- Lower Pole: Under normal circumstances, the lower pole does not extend beyond the midaxillary line, making it generally non-palpable in healthy adults.
Functions
The spleen is analogous to a lymph node in that it filters fluid and facilitates immune responses, but it filters blood, not lymph.
1. Immunological Responses
- Filter Blood-borne Antigens: Acts as a large filter for the blood, exposing blood-borne antigens to lymphocytes and macrophages.
- Production of Antibodies: Crucial site for initiating primary immune responses against encapsulated bacteria (e.g., Streptococcus pneumoniae, Haemophilus influenzae), producing IgM antibodies.
- Storage of Lymphocytes: Contains a large reserve of lymphocytes.
2. Filtration and Hemocatheresis (Removal of Aged/Defective Cells)
- Removes Particulate Matter: Phagocytoses bacteria, parasites, and cellular debris from the blood.
- Removes Aged/Defective Blood Cells: Primarily removes old, rigid, or damaged red blood cells (erythrocytes) and platelets. This process is crucial for maintaining a healthy circulation and preventing the accumulation of non-functional cells.
- Iron Recycling: Extracts iron from heme of senescent red blood cells for reuse in erythropoiesis.
3. Hematopoiesis (in Fetus and Disease States)
- Fetal Role: In the human fetus, the spleen is an important site of extramedullary hematopoiesis until the bone marrow takes over later in gestation.
- Adult Resumption: This function may be resumed in adults in certain pathological conditions, such as severe bone marrow failure (myelofibrosis).
4. Blood Reservoir
Can store a significant volume of blood, particularly red blood cells and platelets, which can be released into circulation when needed (e.g., hemorrhage, stress), though its role as a reservoir is less pronounced in humans compared to some other mammals.
Splenectomy (Surgical Removal of the Spleen)
Despite its important functions, the spleen is not essential for survival.
Compensatory Mechanisms:
Its functions are largely taken over by other organs:
- Liver: Compensates for the filtration and removal of old red blood cells.
- Bone Marrow: Takes over hematopoietic functions.
- Lymph Nodes and other Lymphoid Tissues: Compensate for immune functions.
Blood Supply of the Spleen
Arterial Supply
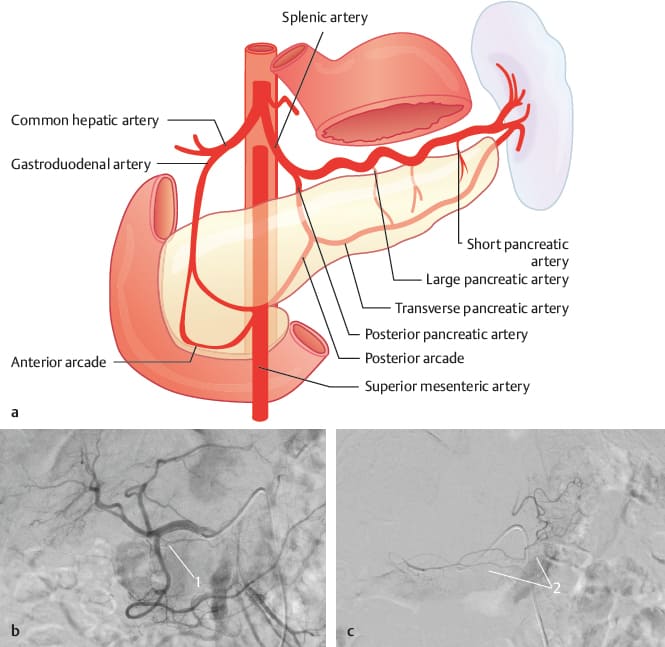
- Splenic Artery: A large and tortuous branch of the celiac trunk.
- Course: Runs along the superior border of the pancreas, posterior to the stomach, within the splenorenal ligament (which attaches the spleen to the posterior abdominal wall near the kidney).
- Branches: Gives off branches to the pancreas, short gastric arteries (supplying the fundus of the stomach), and the left gastro-omental (gastroepiploic) artery before reaching the splenic hilum. At the hilum, it typically divides into 4-5 (or more) segmental branches that enter the spleen.
Venous Drainage
- Splenic Vein: Formed by several tributaries from the splenic hilum.
- Course: Runs posterior to the tail and body of the pancreas.
- Confluence: Posterior to the neck of the pancreas, the splenic vein joins with the superior mesenteric vein (SMV) to form the hepatic portal vein. It also receives the inferior mesenteric vein (often).
Lymphatic Drainage:
- Lymphatic vessels typically follow the splenic artery back to the pancreaticosplenic lymph nodes located along the splenic artery.
- From there, lymph drains into the celiac lymph nodes.
Nerve Supply:
- Supplied by autonomic nerves originating from the celiac plexus.
- Primarily sympathetic innervation, which causes vasoconstriction and contraction of the splenic capsule (if present and muscular enough, as in some animals, to expel blood). Its role in humans is mainly to regulate blood flow.
- Parasympathetic innervation is less clearly defined or functionally significant.
Supports of the Spleen (Ligaments)
The spleen is supported and held in place by several peritoneal folds, or ligaments, derived from the embryonic dorsal mesentery.
Gastrosplenic Ligament
- Description: A double layer of peritoneum that extends from the greater curvature of the fundus of the stomach to the splenic hilum.
- Contents: Contains the short gastric arteries and veins (from the splenic artery/vein) and the left gastro-omental (gastroepiploic) artery and vein.
Splenorenal (Lienorenal) Ligament
- Description: A double layer of peritoneum that extends from the splenic hilum to the anterior aspect of the left kidney and posterior abdominal wall.
- Contents: Contains the splenic artery and vein and the tail of the pancreas. This is a key anatomical relationship; injury to the splenic vessels or damage to the pancreas during splenectomy is a concern.
Phrenicosplenic Ligament
Often considered a part of the splenorenal ligament or a separate fold connecting the superior aspect of the spleen to the diaphragm.
Splenocolic Ligament
Description: Connects the inferior aspect of the spleen to the left colic (splenic) flexure of the colon.
Hilum of the Spleen
The hilum is the area on the visceral surface of the spleen where structures enter and leave the organ.
- Splenic Artery (dividing into segmental branches)
- Splenic Vein (formed by tributaries)
- Lymphatic Vessels
- Nerves (from the celiac plexus)
Histology of the Spleen
The spleen has a characteristic macroscopic and microscopic structure optimized for its functions.
Macroscopic Appearance:
When sectioned, the spleen consists of discrete, small (0.5-1 mm) white nodules called the white pulp, embedded in a larger, red matrix called the red pulp.
Microscopic Appearance:
- Capsule: Surrounded by a thin, fibroelastic outer capsule composed of dense irregular connective tissue, with some smooth muscle fibers (less prominent in humans than in some animals).
- Trabeculae: Short trabeculae (connective tissue septa) extend inwards from the capsule into the parenchyma, providing structural support and carrying blood vessels. The capsule is often thickened at the hilum and blends with the supporting tissues around the vessels.
White Pulp
- Consists of lymphoid aggregations, primarily periarteriolar lymphoid sheaths (PALS) surrounding central arterioles (branches of the splenic artery) and splenic nodules (lymphoid follicles with germinal centers).
- Contains T-lymphocytes (in PALS) and B-lymphocytes (in follicles), playing a key role in initiating immune responses.
Red Pulp
Makes up the bulk of the organ and is a highly vascular tissue. Composed of two main components:
- Splenic Cords (Cords of Billroth): A meshwork of reticular fibers and cells, including macrophages, lymphocytes, plasma cells, and blood cells. This is where old and damaged red blood cells are identified and removed.
- Splenic Sinuses (Sinusoids): Wide, tortuous, thin-walled vascular channels lined by specialized endothelial cells, through which blood flows slowly. The unique structure of these sinuses allows for efficient filtration.
Blood Flow within the Spleen:
- The splenic artery branches into trabecular arteries, which then give rise to central arterioles that enter the white pulp.
- From the white pulp, blood flows into the red pulp, where it can follow either an open circulation (blood leaves the capillaries and enters the splenic cords before re-entering sinuses) or a closed circulation (blood flows directly from capillaries into sinuses). The open circulation pathway is particularly important for the filtration function, as it forces red blood cells to squeeze through narrow spaces, allowing macrophages to detect and remove old/damaged cells.
- Blood from the sinuses then drains into pulp veins, which coalesce into trabecular veins, eventually forming the splenic vein.
The Pancreas
The pancreas is a vital organ with dual functions: it acts as both an exocrine gland (producing digestive enzymes) and an endocrine gland (producing hormones that regulate blood sugar).
General Characteristics:
- Location: A retroperitoneal organ (meaning it lies behind the peritoneum) situated deep in the upper abdomen.
- Color: Typically reddish-brown.
- Position: Lies transversely across the posterior abdominal wall, nestled in the concavity of the duodenum.
Mixed Gland:
Exocrine Component
Produces digestive enzymes (e.g., amylase, lipase, proteases) that are secreted into the duodenum to chemically break down food for absorption in the small intestines.
Endocrine Component
Produces hormones (e.g., insulin, glucagon, somatostatin) that are secreted directly into the bloodstream to regulate glucose metabolism.
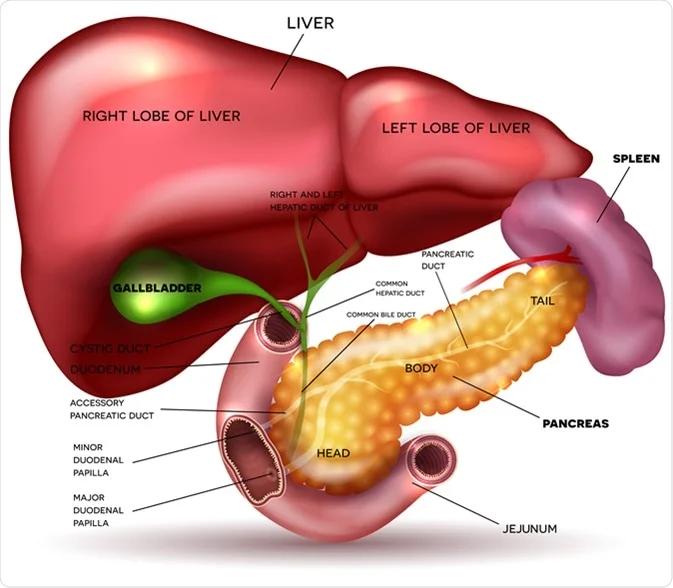
Structure
The pancreas is divided into four main parts: head, neck, body, and tail.
- Head:
- The broadest part of the pancreas.
- Located on the far right, firmly nestled within the C-shaped concavity of the duodenum.
- Uncinate Process: A small, hook-like projection from the lower-posterior part of the head that extends to the left, posterior to the superior mesenteric artery and vein. This is embryologically distinct.
- Neck:
- A slightly constricted portion that connects the head to the body.
- Lies anterior to the superior mesenteric artery and vein, and the formation of the portal vein (where the superior mesenteric and splenic veins merge).
- Body:
- The main, central part of the pancreas.
- Extends from the neck to the tail, typically lying anterior to the aorta and superior mesenteric artery.
- Tail:
- The narrowest and most mobile part of the pancreas.
- Extends to the left, often reaching the hilum of the spleen.
- Significantly, the tail of the pancreas lies within the splenorenal ligament, a peritoneal fold that connects the spleen to the posterior abdominal wall (near the left kidney). This anatomical proximity makes the tail of the pancreas vulnerable to injury during splenic surgery (e.g., splenectomy).
Relations of the Pancreas
The deep, central location of the pancreas means it has numerous vital relations.
Anteriorly:
- Stomach: The posterior wall of the stomach is directly anterior to the body of the pancreas.
- Lesser Sac (Omental Bursa): The lesser sac separates the stomach from the pancreas.
- Transverse Colon: Lies inferior to the body of the pancreas.
- Transverse Mesocolon: The attachment of the transverse mesocolon crosses the anterior surface of the pancreas.
Posteriorly:
- Inferior Vena Cava (IVC): Lies posterior to the head of the pancreas.
- Aorta: Lies posterior to the body of the pancreas.
- Common Bile Duct: Descends in a groove on the posterior surface of the head of the pancreas, sometimes even tunneling through it.
- Superior Mesenteric Artery and Vein: Pass posterior to the neck and anterior to the uncinate process.
- Left Kidney and Left Suprarenal Gland: The body and tail of the pancreas are anterior to these structures.
- Spleen: The tail of the pancreas extends to the hilum of the spleen.
- Renal Vessels, Splenic Vein, Left Crus of Diaphragm: Also posterior to various parts.
Blood Supply
The pancreas has a rich blood supply, primarily from branches of the celiac trunk and superior mesenteric artery.
Arterial Supply:
- Head and Uncinate Process: Supplied by the superior pancreaticoduodenal arteries (anterior and posterior branches from the gastroduodenal artery, a branch of the common hepatic artery) and inferior pancreaticoduodenal arteries (anterior and posterior branches from the superior mesenteric artery). These arteries form anastomotic arches.
- Body and Tail: Supplied by numerous branches from the splenic artery (a branch of the celiac trunk) as it courses along the superior border of the pancreas.
Venous Drainage:
- Veins generally follow the arteries.
- The pancreaticoduodenal veins drain into the superior mesenteric vein or portal vein.
- Veins from the body and tail drain into the splenic vein.
- Ultimately, all pancreatic venous blood drains into the hepatic portal system.
Lymphatic Drainage:
- Lymphatic vessels follow the arteries and drain into pancreaticosplenic, pyloric, and superior mesenteric lymph nodes, and ultimately to the celiac lymph nodes.
Innervation:
- Autonomic Nerves: Receive both sympathetic and parasympathetic innervation via the celiac and superior mesenteric plexuses.
- Parasympathetic (Vagus Nerve): Primarily stimulates exocrine secretion and promotes insulin release.
- Sympathetic (Splanchnic Nerves): Primarily inhibits exocrine secretion and modulates hormone release.
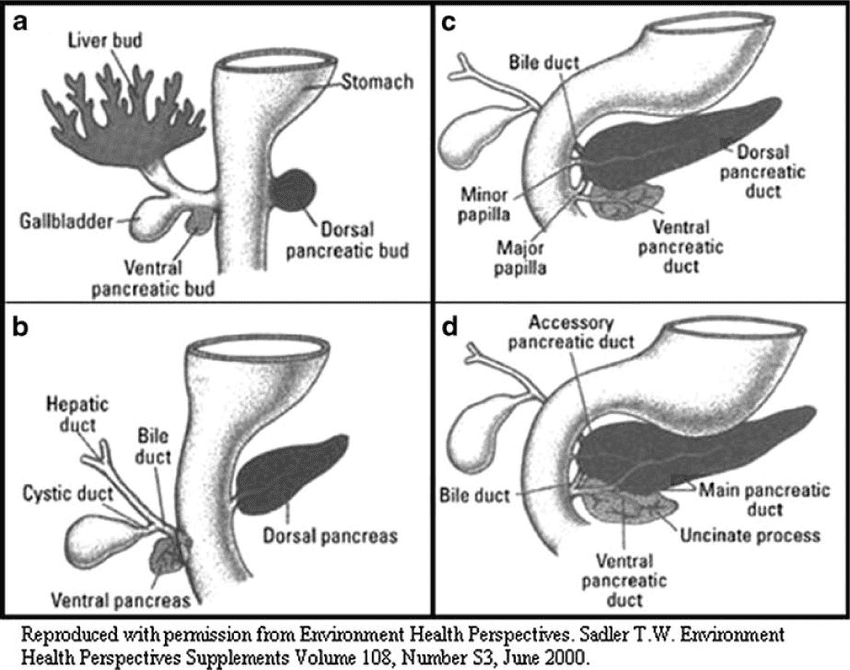
Embryology of the Pancreas
The pancreas develops from two endodermal outgrowths of the foregut.
- Origin: Develops from the endoderm of the primitive foregut.
- Dorsal and Ventral Buds:
- Dorsal Pancreatic Bud: Appears first, as an outgrowth from the dorsal wall of the duodenum. It forms most of the pancreas.
- Ventral Pancreatic Bud: Appears later, as an outgrowth from the ventral wall of the duodenum, in close association with the hepatic diverticulum (which forms the liver and gallbladder).
- Rotation and Fusion:
- As the duodenum rotates to the right, the ventral pancreatic bud moves posteriorly and to the left.
- It comes to lie inferior and posterior to the dorsal pancreatic bud.
- The two buds then fuse around the 6th-7th week of development.
- Contributions to the Adult Pancreas:
- Dorsal Bud: Forms the upper part of the head, body, and tail of the pancreas, and the accessory pancreatic duct (duct of Santorini).
- Ventral Bud: Forms the lower part of the head (including the uncinate process) and the main pancreatic duct (distal part of the duct of Wirsung).
- Pancreatic Duct System Formation:
- The main pancreatic duct (of Wirsung) is formed by the fusion of the distal part of the dorsal pancreatic duct and the entire ventral pancreatic duct. It usually drains into the major duodenal papilla along with the common bile duct.
- The proximal part of the dorsal pancreatic duct either obliterates or persists as a small channel, the accessory pancreatic duct (of Santorini), which (when present) drains into the minor duodenal papilla.
- Islets of Langerhans Development:
- The pancreatic islets (of Langerhans), which comprise the endocrine component, develop from the parenchymatous (exocrine) pancreatic tissue during the third month of fetal life.
- Insulin secretion begins around the 5th month of fetal life.
- Glucagon and somatostatin-secreting cells also differentiate from the parenchymal cells.
- Connective Tissue: The connective tissue (stroma) of the pancreas is derived from the surrounding splanchnic mesoderm.
Histology of the Pancreas
The pancreas is distinguished histologically by its dual exocrine and endocrine components.
Exocrine Pancreas (Majority):
- Composed of serous acini (plural of acinus).
- Each acinus is a roughly spherical cluster of pyramid-shaped secretory cells (acinar cells). These cells are deeply basophilic at their base (due to abundant rough endoplasmic reticulum for protein synthesis) and contain zymogen granules (containing inactive digestive enzymes) in their apex.
- The apices of these cells surround a minute central lumen, which represents the terminal end of the duct system.
- Duct System:
- Centroacinar cells: Flattened cells located within the lumen of the acinus, marking the beginning of the duct system.
- Intercalated ducts: Smallest tributaries, lined by simple low cuboidal epithelium. They drain the acini.
- Intralobular ducts: Formed by the convergence of intercalated ducts.
- Interlobular ducts: Located in the septa between lobules, receiving drainage from intralobular ducts. These are lined by simple cuboidal to stratified cuboidal epithelium.
- Main Pancreatic Duct (Duct of Wirsung): The major collecting duct, with a progressively thicker layer of dense collagenous supporting tissue and smooth muscle in its wall.
- Supporting Tissue: Inconspicuous loose connective tissue separates adjacent acini, containing numerous capillaries that supply nutrients and remove waste.
Endocrine Pancreas (Minority):
- Composed of the Islets of Langerhans, which are spherical clusters of endocrine cells scattered throughout the exocrine tissue. They typically stain more poorly (lighter) than the surrounding acinar tissue in routine H&E stains.
- Each islet contains various cell types, each producing different hormones:
| Cell Type | Hormone | Function |
|---|---|---|
| Alpha (α) cells | Glucagon | Raises blood glucose |
| Beta (β) cells | Insulin | Lowers blood glucose (Most numerous) |
| Delta (δ) cells | Somatostatin | Regulates alpha and beta cells |
| PP cells (Gamma cells) | Pancreatic polypeptide | Regulates pancreatic secretion |
The islets are highly vascularized to facilitate rapid hormone diffusion into the bloodstream.
Pancreatic Disease
The deep, retroperitoneal location and critical functions of the pancreas make it susceptible to various diseases, often with severe consequences.
Location and Pain Referral:
- Because it is a retroperitoneal organ located deep in the abdomen, the pancreas is rarely affected by direct superficial abdominal injuries.
- Pain originating from the pancreas is often referred to the back or felt in the epigastric region, sometimes radiating to the back.
- This referred pain can be confused with pain from surrounding structures such as the stomach, duodenum, spleen, kidneys, or even cardiac pain.
Acute Pancreatitis
- Definition: Acute inflammation of the pancreas.
- Common Causes: The two most common causes are gallstones (obstructing the pancreatic duct or ampulla) and alcohol abuse.
- Pathophysiology: Premature activation of digestive enzymes within the pancreatic cells leads to autodigestion of the pancreas.
- Symptoms: Severe epigastric pain, often radiating to the back, nausea, vomiting, fever.
- Complications: Can range from mild to severe, including systemic inflammatory response syndrome (SIRS), organ failure, pseudocyst formation, and pancreatic necrosis.
Chronic Pancreatitis:
- Definition: Persistent inflammation of the pancreas that results in irreversible morphological changes and progressive loss of exocrine and/or endocrine function.
- Causes: Most commonly chronic alcohol abuse, but also genetic factors, autoimmune diseases, and idiopathic.
Pancreatic Cancer:
- Highly aggressive cancer, often diagnosed at late stages due to its deep location and non-specific early symptoms.
- Most common type: Adenocarcinoma, usually arising from the ducts.
- Due to its close proximity and location within the splenorenal ligament, the tail of the pancreas is particularly vulnerable to injury during splenectomy.
- Damage to the pancreatic tail can lead to leakage of pancreatic enzymes, causing local inflammation, abscess formation, or even a pancreatic fistula, which can be difficult to manage. This is a recognized complication.