Cranial Nerves
Comprehensive Notes on Neuroanatomy.
This exhaustive master guide covers the neuroanatomy of the 12 Cranial Nerves, integrating their functional components, brainstem organization, exit points, and high-yield clinical pathophysiology. By the end of this guide, you will master:
- The 7 Functional Components (Modalities) of cranial nerves.
- The Brainstem Organization and the rule of the Sulcus Limitans.
- Detailed anatomical pathways and clinical lesions for Cranial Nerves I through XII.
- How to differentiate Upper Motor Neuron (UMN) vs. Lower Motor Neuron (LMN) cranial nerve lesions.
Part 1: Foundations of Cranial Nerve Anatomy
Before studying individual nerves, we must understand the overarching rules that govern how they are organized, what type of information they carry, and where they originate in the brainstem.
1.1 The 7 Functional Components (Modalities)
Every cranial nerve fiber acts as a specific type of wire, carrying a specific type of signal. We classify these fibers into one of seven functional categories:
| Abbreviation | Full Name | Direction | What It Carries | Example |
|---|---|---|---|---|
| GSA | General Somatic Afferent | Sensory (→ CNS) | Touch, pain, temperature, pressure from skin & mucosa. | Facial sensation (CN V). |
| SSA | Special Somatic Afferent | Sensory (→ CNS) | Special senses of vision, hearing, and balance. | Optic nerve (CN II), Vestibulocochlear (CN VIII). |
| GVA | General Visceral Afferent | Sensory (→ CNS) | Sensation from internal organs (stretch, chemoreception). | Carotid sinus baroreceptors (CN IX). |
| SVA | Special Visceral Afferent | Sensory (→ CNS) | Special chemical senses of taste & smell. | Taste from tongue (CN VII, IX, X). |
| GSE | General Somatic Efferent | Motor (← CNS) | Motor to skeletal muscles derived from embryonic somites. | Extraocular muscles (CN III, IV, VI), tongue (CN XII). |
| GVE | General Visceral Efferent | Motor (← CNS) | Parasympathetic (autonomic) fibers to glands & smooth muscle. | Pupil constriction (CN III), salivation (CN VII, IX). |
| SVE / BME | Special Visceral Efferent / Branchial Motor | Motor (← CNS) | Motor to skeletal muscles derived from pharyngeal (branchial) arches. | Facial expression (CN VII), mastication (CN V), pharynx/larynx (CN IX, X, XI). |
"Some Say Marry Money, But My Brother Says Big Brains Matter More"
This classic mnemonic helps you remember the primary function of Cranial Nerves I to XII in order:
- Some = Sensory (CN I, II, VIII)
- Say = Sensory + Motor (CN V, VII, IX, X)
- Marry = Motor (CN III, IV, VI, XI, XII)
- Money = Motor + Parasympathetic (CN III, VII, IX, X)
1.2 The Sulcus Limitans & Brainstem Organization
The sulcus limitans is a crucial anatomical groove found on the floor of the fourth ventricle. It serves as a strict dividing line that organizes the brainstem into two distinct functional zones during embryological development.
Key Rule: The "M-S RULE"
- Medial = Motor (Nuclei located medial to the sulcus limitans control motor functions).
- Lateral = Sensory (Nuclei located lateral to the sulcus limitans process sensory information).
Note: This is the exact same organization as the spinal cord (where anterior horn = motor, posterior horn = sensory), except the neural tube has been "unzipped" and rotated 90 degrees in the brainstem, laying it flat.
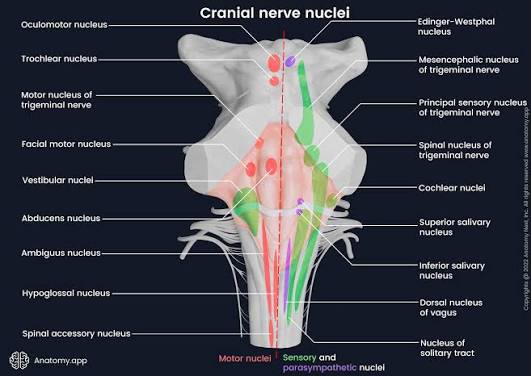
Columnar Organization of Nuclei (From Medial to Lateral)
The cranial nerve nuclei are perfectly organized in longitudinal columns:
- Most medial: GSE nuclei (somatic motor) — CN III, IV, VI, XII.
- Next: GVE nuclei (parasympathetic) — Edinger-Westphal, superior/inferior salivatory, dorsal motor nucleus of vagus.
- Next: SVE nuclei (branchial motor) — motor nucleus of V, facial motor nucleus, nucleus ambiguus, spinal accessory nucleus.
- At sulcus limitans: SVA (taste) and GVA (visceral sensory) — nucleus of the solitary tract.
- Lateral: GSA (general sensation) — main and spinal trigeminal nuclei.
- Most lateral: SSA (special sensation) — cochlear & vestibular nuclei.
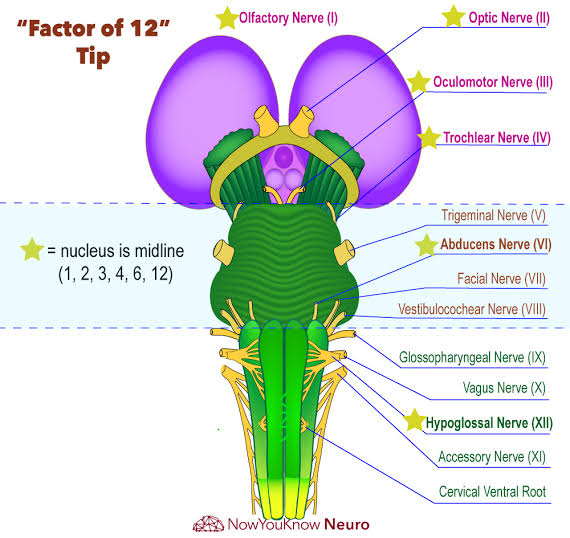
1.3 Exit Points from the Brainstem — "Factor in 4's"
A simple way to memorize where the cranial nerves exit the brainstem is the "Factor in 4's" rule:
- Above the Pons (Supratentorial/Midbrain): CN I–IV (Olfactory, Optic, Oculomotor, Trochlear).
- At the Pons: CN V–VIII (Trigeminal, Abducens, Facial, Vestibulocochlear).
- Below the Pons (Medulla): CN IX–XII (Glossopharyngeal, Vagus, Accessory, Hypoglossal).
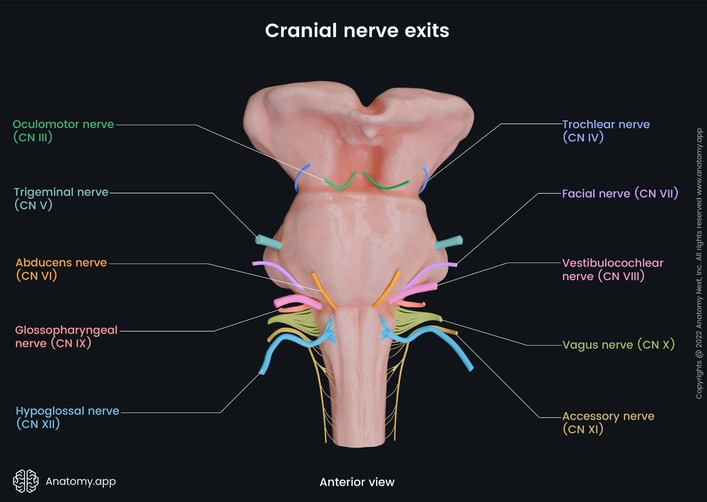
1.4 Brainstem Exits and Skull Foramina
| Cranial Nerve | Brainstem Exit | Skull Foramen | Brainstem Level |
|---|---|---|---|
| CN I Olfactory | Forebrain (not true brainstem) | Cribriform plate of ethmoid | Supratentorial |
| CN II Optic | Diencephalon | Optic canal | Supratentorial |
| CN III Oculomotor | Interpeduncular fossa of midbrain | Superior orbital fissure | Midbrain |
| CN IV Trochlear | Dorsal midbrain (posterior!) | Superior orbital fissure | Midbrain |
| CN V Trigeminal | Lateral pons | Sup. orbital fissure (V1), For. rotundum (V2), For. ovale (V3) | Pons |
| CN VI Abducens | Pontomedullary junction | Superior orbital fissure | Pons |
| CN VII Facial | Cerebellopontine angle | Internal acoustic meatus → stylomastoid foramen | Pons |
| CN VIII Vestibulocochlear | Cerebellopontine angle | Internal acoustic meatus | Pons |
| CN IX Glossopharyngeal | Post-olivary sulcus of medulla | Jugular foramen | Medulla |
| CN X Vagus | Post-olivary sulcus of medulla | Jugular foramen | Medulla |
| CN XI Accessory | Post-olivary sulcus + C1–C5 spinal cord | Jugular foramen | Medulla/Spinal |
| CN XII Hypoglossal | Pre-olivary sulcus of medulla | Hypoglossal canal | Medulla |
1.5 Parasympathetic Fibers in Cranial Nerves (GVE)
It is vital to remember that only 4 cranial nerves carry parasympathetic (GVE) fibers. They dictate rest, digestion, and glandular secretion in the head, neck, and viscera.
| Nerve | Preganglionic Nucleus | Ganglion | Target | Effect |
|---|---|---|---|---|
| CN III Oculomotor | Edinger-Westphal nucleus (midbrain) | Ciliary ganglion | Sphincter pupillae + Ciliary muscle | Pupil constriction + Lens accommodation |
| CN VII Facial | Superior salivatory nucleus (pons) | Pterygopalatine + Submandibular ganglia | Lacrimal, submandibular & sublingual glands | Tearing + Salivation |
| CN IX Glossopharyngeal | Inferior salivatory nucleus (medulla) | Otic ganglion | Parotid gland | Salivation |
| CN X Vagus | Dorsal motor nucleus of vagus (medulla) | Terminal ganglia in/near target organs | Thoracic & abdominal viscera | "Rest & digest" functions (decreased HR, increased digestion) |
1.6 UMN vs LMN Lesions: The Clinical Divide
Determining whether a nerve lesion is "Upper" (in the brain) or "Lower" (at or after the nucleus) is a fundamental clinical skill.
| Feature | Supranuclear (UMN) Lesion | Nuclear/Infranuclear (LMN) Lesion |
|---|---|---|
| Location | Above the cranial nerve nucleus (e.g., motor cortex, internal capsule, upper brainstem). | At or below the nucleus (the nerve root, the peripheral nerve itself, or the skull base). |
| Muscle Tone | Increased (spasticity). | Decreased (flaccidity). |
| Reflexes | Hyperreflexia. | Hyporeflexia / Areflexia. |
| Fasciculations | Absent. | May be prominently present (twitching). |
| Atrophy | Absent or very mild (disuse). | Present and severe (denervation atrophy). |
| Facial Nerve Specific | Forehead spared (because the upper face receives bilateral cortical innervation). | Entire half of face paralyzed (Bell's Palsy). |
Part 2: CN I to IV — Supratentorial & Midbrain
These nerves control our highest-order special senses (smell, sight) and the complex control of eye movements from the midbrain.
I. CN I — Olfactory Nerve
Nervus Olfactorius | SVA (SPECIAL VISCERAL AFFERENT)
Anatomy & Pathway
- Origin: Olfactory receptor neurons located in the olfactory epithelium of the nasal cavity (superior nasal concha & nasal septum).
- Passage: The delicate fibers pass upwards through the cribriform plate of the ethmoid bone (a thin, sieve-like bone that is easily fractured in head trauma).
- Termination: Olfactory bulb → Olfactory tract → Primary olfactory cortex (piriform cortex, uncus, amygdala).
Unique Feature: Bypassing the Thalamus!
Unlike all other sensory pathways (vision, hearing, touch), the sense of smell goes directly to the cortex without routing through a thalamic relay station. This direct connection to the limbic system (amygdala) is why smells can trigger incredibly powerful, instantaneous emotional memories.
Clinical Pearl: Anosmia (Loss of Smell)
- Common causes: Head trauma (specifically cribriform plate fracture), COVID-19, chronic rhinosinusitis, early neurodegenerative diseases (Parkinson's and Alzheimer's).
- Key Emergency Association: Anosmia combined with CSF rhinorrhea (clear, watery fluid dripping from the nose) following head trauma strongly indicates a cribriform plate fracture with a CSF leak. High risk of meningitis!
II. CN II — Optic Nerve
Nervus Opticus | SSA (SPECIAL SOMATIC AFFERENT)
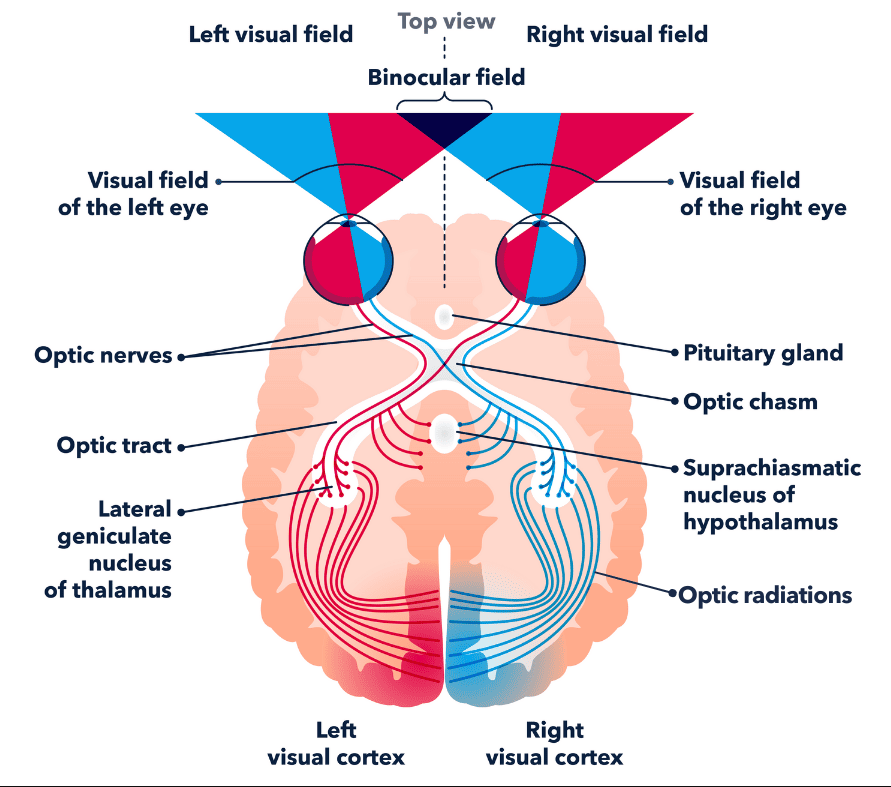
The Complete Visual Pathway
- Retina: Photoreceptors (rods and cones) → bipolar cells → retinal ganglion cells.
- Optic nerve (CN II): Exits the eyeball posteriorly at the optic disc (the blind spot).
- Optic chiasm: Located above the sella turcica (where the pituitary gland sits). Here, nasal retinal fibers cross to the opposite side, while temporal fibers stay ipsilateral.
- Optic tract: Contains fibers representing the contralateral visual field of BOTH eyes.
- Lateral Geniculate Nucleus (LGN): The primary thalamic relay station — 90% of visual fibers synapse here.
- Optic radiations: Fibers pass through the temporal lobe (Meyer's loop) and parietal lobes (superior bundle).
- Primary visual cortex (V1): Located in the calcarine sulcus of the occipital lobe.
Visual Field Deficits — Lesion Localization
| Lesion Location | Visual Field Deficit | Key Feature / Classic Cause |
|---|---|---|
| Retina / Optic nerve | Complete blindness in ONE eye | Ipsilateral anopsia. |
| Optic chiasm (center) | Bitemporal hemianopsia | Loss of both temporal visual fields (tunnel vision). Classic sign of a pituitary adenoma pressing upward. |
| Optic tract | Contralateral homonymous hemianopsia | Same visual field lost in both eyes. |
| Optic radiations (temporal / Meyer's loop) | Contralateral superior quadrantanopia | "Pie in the sky" deficit. Indicates a temporal lobe lesion. |
| Optic radiations (parietal) | Contralateral inferior quadrantanopia | "Pie on the floor" deficit. Indicates a parietal lobe lesion. |
| Visual cortex | Contralateral homonymous hemianopsia with macular sparing | Occipital lobe lesion (often a PCA stroke; the macula is spared due to dual blood supply from the MCA). |
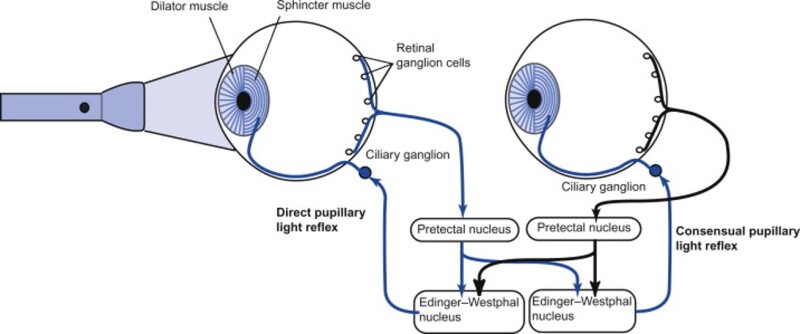
Pupillary Light Reflex (Afferent = CN II, Efferent = CN III)
The pathway involves "2 Neurons and 2 Synapses":
- Afferent (sensory): CN II → Pretectal nucleus (in the midbrain, near the superior colliculus).
- Efferent (motor): Pretectal nucleus → Bilateral Edinger-Westphal nuclei → CN III (parasympathetic) → Ciliary ganglion → Sphincter pupillae muscle.
Why do both pupils constrict when you shine a light in only one eye? The pretectal nucleus sends connecting fibers to both the left and right Edinger-Westphal nuclei simultaneously. This creates the consensual light reflex.
Marcus Gunn Pupil (RAPD)
RAPD = Relative Afferent Pupillary Defect.
When the doctor swings a flashlight from the normal eye to the affected eye, both pupils paradoxically appear to dilate instead of constrict.
Cause: Severe optic nerve damage on the affected side (e.g., optic neuritis in Multiple Sclerosis, or ischemic optic neuropathy). The brain registers a massive drop in light intensity when the beam moves to the damaged eye, causing a dilatory response.
III. CN III — Oculomotor Nerve
Nervus Oculomotorius | GSE (SOMATIC MOTOR) GVE (PARASYMPATHETIC)
Anatomy
- Nucleus: Oculomotor nucleus in the midbrain (at the level of the superior colliculus).
- Exit: Interpeduncular fossa of the midbrain (between the cerebral peduncles).
- Course: Passes forward through the cavernous sinus, then enters the orbit via the superior orbital fissure.
Muscles Innervated (GSE Component)
CN III innervates 4 of the 6 extraocular muscles, plus the eyelid lifter:
| Muscle | Action | Test Movement |
|---|---|---|
| Superior rectus | Elevation (upward gaze) | Look up and in |
| Inferior rectus | Depression (downward gaze) | Look down and in |
| Medial rectus | Adduction (inward gaze) | Look toward nose |
| Inferior oblique | Elevation, abduction, extorsion | Look up and out |
| Levator palpebrae superioris | Elevates upper eyelid | — |
Parasympathetic Component (GVE)
- Edinger-Westphal nucleus (parasympathetic origin in midbrain).
- Preganglionic fibers travel piggy-backed on the outside of CN III to the orbit.
- Synapse in the ciliary ganglion (located just behind the eye).
- Postganglionic fibers travel to the Sphincter pupillae (causing pupil constriction/miosis) and the Ciliary muscle (causing lens accommodation for near vision).
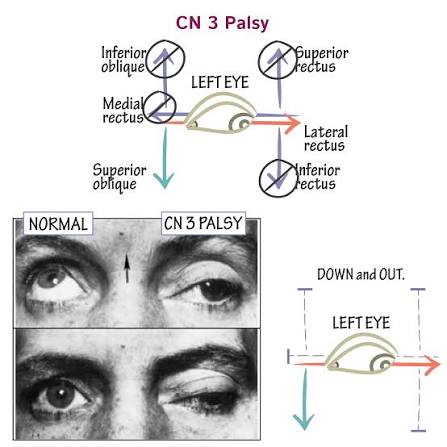
Complete CN III Palsy — The Classic Triad
- "Down and out" eye: The eye deviates downward and laterally. Why? Because the muscles innervated by CN IV (superior oblique pulling down) and CN VI (lateral rectus pulling out) are completely unopposed!
- Severe ptosis: The levator palpebrae superioris is paralyzed, so the eyelid drops shut.
- Dilated, unreactive pupil: The parasympathetic constrictor fibers are lost.
Important Distinction: Surgical vs. Medical CN III Palsy
The parasympathetic fibers run on the superficial outside of the nerve, while the motor fibers are deep inside.
- "Surgical" CN III palsy (Pupil involved): External compression (like a posterior communicating artery aneurysm or uncal herniation) crushes the outside of the nerve first. The pupil dilates. This is a neurosurgical EMERGENCY.
- "Medical" CN III palsy (Pupil spared): Microvascular ischemia (common in severe diabetes or hypertension) kills the core of the nerve, but the outer blood supply keeps the superficial parasympathetic fibers alive. Eye is down and out, but the pupil remains normal.
IV. CN IV — Trochlear Nerve
Nervus Trochlearis | GSE (SOMATIC MOTOR)
Unique Anatomical Features (The Two "Onlys")
CN IV is the anatomical oddball of the cranial nerves. It is the ONLY cranial nerve that:
- Exits dorsally: It emerges from the posterior aspect of the brainstem, wrapping entirely around the midbrain to reach the front.
- Fully decussates: It crosses over completely before exiting. The left nucleus controls the right eye!
Muscle Innervated
CN IV innervates only ONE muscle: the Superior Oblique.
- Action: Primarily causes intorsion (internal rotation), as well as depression and abduction.
- Clinical Test: Ask the patient to look down and in (e.g., as if reading a book or walking down stairs). The superior oblique is the primary depressor when the eye is adducted.
CN IV Palsy — Vertical Diplopia
- Symptoms: The patient complains of vertical double vision (images stacked on top of each other), which gets dramatically worse when looking down and in.
- Signs: The affected eye drifts upward (hypertropia) because the inferior oblique is unopposed.
- Compensation: The patient will adopt a characteristic head tilt toward the opposite shoulder to compensate for the lost intorsion. (Bielschowsky head tilt test is positive).
- Cause: Due to its incredibly long and thin intracranial course, it is highly susceptible to stretching from head trauma.
Part 3: CN V to VIII — The Pons Group
This group manages facial sensation, facial expression, eye abduction, hearing, and balance.
V. CN V — Trigeminal Nerve
Nervus Trigeminus | GSA (GENERAL SENSATION) SVE (BRANCHIAL MOTOR)
Known as the "Great Sensory Nerve" and the First Arch Motor nerve, CN V is the largest cranial nerve. It carries sensation from the entire face and provides motor supply to the muscles of mastication.
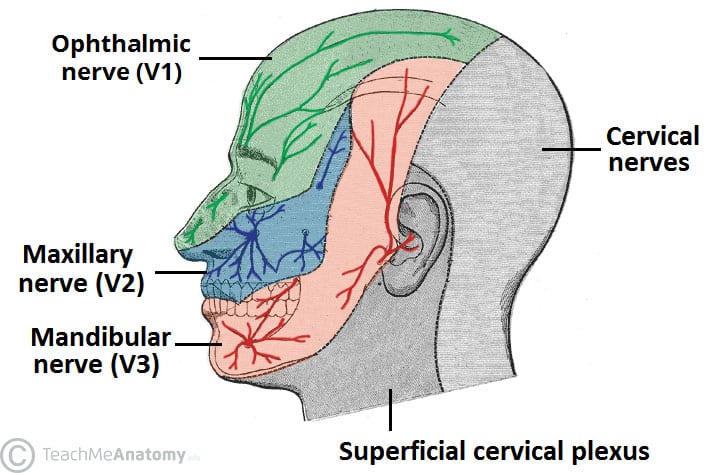
Three Sensory Divisions (GSA)
| Division | Foramen | Territory (Skin) | Key Branches |
|---|---|---|---|
| V1: Ophthalmic | Superior orbital fissure | Top strip: Forehead, upper eyelid, cornea, dorsum of nose, scalp to vertex. | Frontal, lacrimal, nasociliary. |
| V2: Maxillary | Foramen rotundum | Middle strip: Lower eyelid, cheek, upper lip, upper teeth, palate, nasal cavity. | Zygomatic, infraorbital, superior alveolar. |
| V3: Mandibular | Foramen ovale | Bottom strip: Lower lip, chin, lower teeth, temporal region, anterior 2/3 of tongue (sensation only, NOT taste). | Auriculotemporal, buccal, lingual, inferior alveolar, mental. |
Four Trigeminal Nuclei in the Brainstem
- Mesencephalic nucleus (Midbrain): Proprioception from muscles of mastication, TMJ, teeth. (Unique: The primary sensory cell bodies are actually IN the CNS, not in a peripheral ganglion!).
- Main sensory nucleus (Upper pons): Fine touch and pressure from the face.
- Spinal nucleus (Lower pons to upper cervical cord): Pain and temperature from the face.
- Motor nucleus (Upper pons): Motor output (SVE) to muscles of mastication.
Motor Component (V3 Only)
Motor fibers exit exclusively with the V3 division through the foramen ovale to supply:
- Muscles of mastication: Masseter, temporalis, medial and lateral pterygoids.
- Tensor tympani: Tenses the tympanic membrane to dampen loud sounds.
- Anterior belly of digastric and Mylohyoid.
Key Trigeminal Reflexes
- Corneal Reflex: Afferent = CN V1 (detects touch on the cornea). Efferent = CN VII (causes the orbicularis oculi to blink). Absent reflex suggests severe brainstem dysfunction.
- Jaw-Jerk Reflex: Afferent = CN V3 (teeth/ligaments). Efferent = CN V3 (masseter). Tapping the chin causes the jaw to jerk closed. An exaggerated jerk indicates an Upper Motor Neuron (supranuclear) lesion.
Trigeminal Neuralgia ("Tic Douloureux")
Characterized by sudden, severe, electric-shock-like facial pain, usually localized to the V2 or V3 territory. It is triggered by trivial stimuli like light touch, chewing, or a cold wind. It is most commonly caused by a vascular compression of the nerve root (often by the superior cerebellar artery). Treated first-line with Carbamazepine.
VI. CN VI — Abducens Nerve
Nervus Abducens | GSE (SOMATIC MOTOR)
- Nucleus: Located in the pons, near the floor of the fourth ventricle.
Unique relation: Motor fibers from the Facial nerve (CN VII) wrap internally around the CN VI nucleus before exiting, creating a visible bump on the ventricle floor called the facial colliculus. - Course: Has a very long intracranial course. It passes through the cavernous sinus before entering the orbit via the superior orbital fissure.
- Muscle Innervated: Solely the Lateral Rectus. Action = Abduction (pulls the eye laterally away from the nose).
CN VI Palsy & The "False Localizing Sign"
Presentation: The patient cannot abduct the affected eye, resulting in a medial deviation (esotropia) and horizontal diplopia that worsens when looking toward the affected side.
Clinical Pearl: Because CN VI has the longest intracranial course across the skull base, it is easily stretched. Therefore, a CN VI palsy can occur purely due to generalized increased Intracranial Pressure (ICP) from anywhere in the brain (like a distant tumor), acting as a "false localizing sign."
VII. CN VII — Facial Nerve
Nervus Facialis | SVE (BRANCHIAL MOTOR) GVE (PARASYMPATHETIC) SVA (TASTE) GSA (GENERAL SENSATION)
Anatomy and Course
- Nuclei: Facial motor nucleus (SVE) and Superior salivatory nucleus (GVE) in the pons.
- Exit: Leaves the brainstem at the cerebellopontine angle, enters the internal acoustic meatus (alongside CN VIII), and travels through the facial canal in the petrous temporal bone.
- Internal Branches: Gives off the Greater petrosal nerve (tears), Nerve to stapedius (dampens sound), and Chorda tympani (taste and saliva).
- Final Exit: Exits the skull via the stylomastoid foramen to fan out and supply the face.
| Component | Function | Details / Targets |
|---|---|---|
| SVE (Motor) | Facial Expression | Frontalis, orbicularis oculi, orbicularis oris, buccinator, platysma, stapedius, posterior belly of digastric. |
| GVE (Parasymp.) | Secretomotor | Lacrimal gland (tears), submandibular and sublingual glands (saliva) via chorda tympani. |
| SVA (Special Sensory) | Taste | Anterior 2/3 of the tongue (via chorda tympani). |
| GSA (General Sensory) | Touch | A tiny area of skin around the external auditory meatus. |
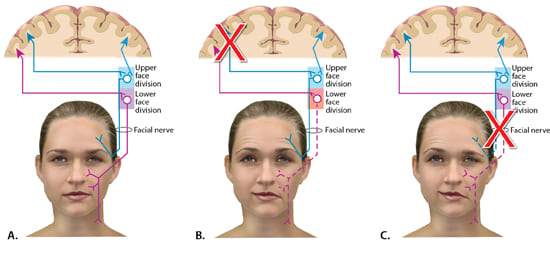
Central vs. Peripheral Facial Palsy: The Most Important Distinction!
To distinguish between a stroke (Central/UMN) and Bell's Palsy (Peripheral/LMN), look at the forehead.
- Central (UMN) Palsy: Lesion is in the motor cortex or internal capsule. The forehead is SPARED. The upper face receives bilateral cortical input, so the healthy hemisphere takes over. Result: Only the lower half of the face on the contralateral side droops.
- Peripheral (LMN) Palsy (Bell's Palsy): Lesion is in the facial nerve itself. The forehead is AFFECTED. The entire nerve is dead, so the entire ipsilateral half of the face is paralyzed. Patient cannot close their eye or wrinkle their forehead. May also present with hyperacusis (loud sounds hurt, due to stapedius paralysis) and loss of taste.
Mnemonic: "Forehead is friends with both sides."
VIII. CN VIII — Vestibulocochlear Nerve
Nervus Vestibulocochlearis | SSA (SPECIAL SENSATION)
CN VIII is purely sensory and is divided into two distinct functional parts: Cochlear (hearing) and Vestibular (balance).
1. Cochlear Division (Hearing)
Organ of Corti (hair cells) → Cochlear nerve → Cochlear nuclei (pons-medulla junction) → Bilateral projections via lateral lemniscus → Inferior colliculus (midbrain) → Medial Geniculate Nucleus (thalamus) → Primary auditory cortex (Heschl's gyrus).
Key Point: Auditory pathways ascend bilaterally. Therefore, a unilateral brain lesion above the level of the cochlear nuclei will not cause total deafness in one ear.
2. Vestibular Division (Balance)
Semicircular canals (angular rotation) + Utricle/Saccule (linear acceleration) → Vestibular nerve → Vestibular nuclei (pons/medulla). Projects to the Cerebellum (flocculonodular lobe) for balance, the MLF (for the Vestibulo-Ocular Reflex to coordinate eye movements with head turning), and the spinal cord (postural adjustments).
Weber & Rinne Tests for Hearing Loss
Conductive Hearing Loss: (Issue in outer/middle ear like wax or otosclerosis).
Weber: Sound localizes to the AFFECTED ear (bone conduction takes over).
Rinne: Bone Conduction > Air Conduction (Negative Rinne).
Sensorineural Hearing Loss: (Issue in inner ear or nerve, like Acoustic Neuroma).
Weber: Sound localizes to the NORMAL ear.
Rinne: Air Conduction > Bone Conduction (Positive Rinne, but both are diminished compared to normal).
Part 4: CN IX to XII — The Medulla Group
These nerves manage swallowing, speech, visceral regulation, taste, and tongue movement.
IX. CN IX — Glossopharyngeal Nerve
Nervus Glossopharyngeus | Contains 5 modalities: SVE, GVE, SVA, GVA, GSA.
Shared Nuclei: CN IX shares several key nuclei in the medulla with the Vagus nerve (CN X), including the Nucleus Ambiguus (motor to pharynx/larynx) and the Nucleus of the Solitary Tract (taste and visceral sensation).
- Motor (SVE): Stylopharyngeus muscle (elevates the pharynx during swallowing).
- Parasympathetic (GVE): Originates in the Inferior salivatory nucleus → otic ganglion → Parotid gland (massive salivation).
- Taste (SVA) & Touch (GSA): Provides both to the Posterior 1/3 of the tongue.
- Visceral (GVA): Crucial for the Carotid sinus (detects blood pressure changes) and carotid body (chemoreceptors for O2/CO2). Clinical: Carotid sinus massage triggers this nerve to signal the medulla, increasing vagal tone to slow down the heart rate in certain arrhythmias.
X. CN X — Vagus Nerve
Nervus Vagus | "The Wanderer" — Contains 5 modalities.
The longest cranial nerve, traversing from the medulla all the way down to the colon.
- Motor (SVE): Pharyngeal constrictors (for swallowing) and all intrinsic laryngeal muscles (for voice production).
- Parasympathetic (GVE): The primary rest-and-digest nerve of the body. Controls thoracic and abdominal viscera (slows the heart, constricts bronchi, ramps up intestinal digestion).
| Important Branch | Origin / Course | Function |
|---|---|---|
| Superior Laryngeal Nerve | Upper neck | Internal branch: sensation above vocal cords. External branch: motor to cricothyroid muscle (tenses vocal cords for high pitch). |
| Recurrent Laryngeal Nerve | Loops under the subclavian artery (Right) or the Aortic Arch (Left). | Motor to ALL intrinsic laryngeal muscles (except cricothyroid). Sensation below the vocal cords. |
Vagus Clinical Pearls
- Left Recurrent Laryngeal Nerve Vulnerability: Because it loops deep into the chest under the aortic arch, it can be crushed by an aortic aneurysm, mediastinal tumors, or an enlarged left atrium (Ortner's syndrome). Damage causes severe hoarseness.
- Gag Reflex: Afferent sensory = CN IX. Efferent motor = CN X.
- Uvula Deviation: In a CN X lesion, when the patient says "Ahh," the uvula deviates AWAY from the side of the lesion (the strong, healthy side pulls it over).
XI. CN XI — Accessory Nerve
Nervus Accessorius | SVE (BRANCHIAL MOTOR)
CN XI has a unique, confusing anatomy consisting of two parts:
- Cranial Part (Minor): Arises from the medulla, joins the vagus nerve, and is functionally just a part of the vagus.
- Spinal Part (Major/Clinical): Arises from the anterior horns of the C1–C5 spinal cord. The fibers travel UP through the foramen magnum into the skull, join the cranial part, and then immediately exit back down through the jugular foramen.
- Muscles Innervated: Sternocleidomastoid (SCM) (turns head to the opposite side) and Trapezius (shrugs the shoulders).
Accessory Nerve Palsy
Commonly caused by iatrogenic injury during a lymph node biopsy in the posterior triangle of the neck (where the nerve runs very superficially).
Signs: Shoulder droop, inability to shrug against resistance, scapular winging, and weakness turning the head to the opposite side of the lesion.
XII. CN XII — Hypoglossal Nerve
Nervus Hypoglossus | GSE (SOMATIC MOTOR)
- Anatomy: Originates in the medulla, exits between the pyramid and the olive, and leaves the skull via the hypoglossal canal.
- Muscles Innervated: Supplies ALL intrinsic and extrinsic muscles of the tongue (except the palatoglossus, which is CN X).
- Key Muscle - Genioglossus: Protrudes the tongue straight out.
Tongue Deviation
- LMN Lesion: The tongue deviates TOWARD the side of the lesion upon protrusion (the healthy side pushes it over). Accompanied by severe atrophy and fasciculations (twitching).
- UMN Lesion: The tongue deviates AWAY from the brain lesion. No atrophy or twitching.
Part 5 & 6: Clinical Pearls & Quick Reference
Essential Mnemonics
- Extraocular Muscles: "LR6 - SO4 - AO3" (Lateral Rectus = VI, Superior Oblique = IV, All Others = III).
- Taste to the Tongue: Anterior 2/3 = CN VII. Posterior 1/3 = CN IX. Epiglottis = CN X.
- Tongue vs. Uvula Lesions: "Tongue points Toward (LMN), Uvula points Upposite (Opposite)."
- Weber Test for Conductive Loss: "Weber goes to the Worse ear in Conductive loss."
High-Yield Clinical Scenarios
"Down and out" eye + Dilated Pupil
Diagnosis: Complete CN III palsy (Surgical).
Action: Think Posterior Communicating Artery (PCoA) aneurysm. Needs urgent MR/CT angiography to prevent rupture.
Sudden Unilateral Facial Weakness — Forehead Spared
Diagnosis: Central (UMN) facial palsy.
Action: The patient is having a stroke. Initiate emergency stroke workup.
Sudden Unilateral Facial Weakness — Entire Face Affected
Diagnosis: Bell's Palsy (LMN facial nerve lesion).
Action: Oral corticosteroids. Eye protection is critical as they cannot blink to moisturize the cornea.
Bitemporal Hemianopsia
Diagnosis: Lesion at the optic chiasm.
Cause: Pituitary adenoma compressing from below.
Quick Reference: All 12 Cranial Nerves Summary
| # | Name | Type | Foramen | Key Function | Classic Lesion Sign |
|---|---|---|---|---|---|
| I | Olfactory | Sensory | Cribriform plate | Smell | Anosmia |
| II | Optic | Sensory | Optic canal | Vision | Visual field defect |
| III | Oculomotor | Motor + Parasymp | Sup. orbital fissure | 4 EOMs, pupil, eyelid | "Down and out" eye, ptosis, dilated pupil |
| IV | Trochlear | Motor | Sup. orbital fissure | Superior oblique | Vertical diplopia, head tilt |
| V | Trigeminal | Mixed | Sup. orbital fissure (V1), For. rotundum (V2), For. ovale (V3) | Face sensation, mastication | Facial numbness, trigeminal neuralgia |
| VI | Abducens | Motor | Sup. orbital fissure | Lateral rectus (abduction) | Esotropia, horizontal diplopia |
| VII | Facial | Mixed | Internal acoustic meatus → Stylomastoid foramen | Facial expression, taste, tears, saliva | Bell's palsy (LMN) or forehead-spared weakness (UMN) |
| VIII | Vestibulocochlear | Sensory | Internal acoustic meatus | Hearing and balance | Sensorineural hearing loss, vertigo, nystagmus |
| IX | Glossopharyngeal | Mixed | Jugular foramen | Taste (post. 1/3), parotid, carotid sinus | Loss of gag reflex (afferent), impaired taste |
| X | Vagus | Mixed | Jugular foramen | Pharynx/larynx, parasympathetic to viscera | Uvula deviates AWAY, hoarseness, dysphagia |
| XI | Accessory | Motor | Jugular foramen | SCM and Trapezius | Weak head turning, shoulder droop |
| XII | Hypoglossal | Motor | Hypoglossal canal | Tongue muscles | Tongue deviates TOWARD lesion, atrophy, fasciculations |