Autonomic Nervous System
Complete detailed notes covering the structural blueprint, visceral afferents, special pathways, pharmacology, and clinical anatomical correlations of the Autonomic Nervous System (ANS).
1. Structural Organization
The autonomic nervous system (ANS) controls the involuntary functions of visceral organs, smooth muscle, cardiac muscle, and glands. Unlike the somatic system, it operates through a two-neuron chain with a synapse located in a peripheral ganglion.
Somatic vs. Autonomic Motor Systems
The most fundamental distinction is the number of neurons between the Central Nervous System (CNS) and the effector organ.
| Feature | Somatic Motor | Autonomic Motor |
|---|---|---|
| Neurons in chain | ONE neuron (Upper Motor Neuron directly to skeletal muscle) | TWO neurons (preganglionic + postganglionic) |
| Neurotransmitter at effector | Acetylcholine (ACh) only | ACh (parasympathetic) or Norepinephrine (sympathetic) |
| Effector | Skeletal muscle | Smooth muscle, cardiac muscle, glands |
| Control | Voluntary | Involuntary |
| Myelination | Thickly myelinated (A-alpha fibers) | Thinly myelinated (preganglionic) or unmyelinated (postganglionic) |
The Two-Neuron Chain Explained
- Preganglionic neuron: The cell body is located in the CNS (brainstem, sacral spinal cord, or intermediolateral cell column). Its myelinated axon travels to a peripheral ganglion.
- Postganglionic neuron: The cell body is located in the peripheral ganglion. Its unmyelinated axon travels to the target organ.
- The ganglion: This is the synapse point between these two neurons. This arrangement allows for divergence — one preganglionic neuron can activate many postganglionic neurons, amplifying the autonomic response.
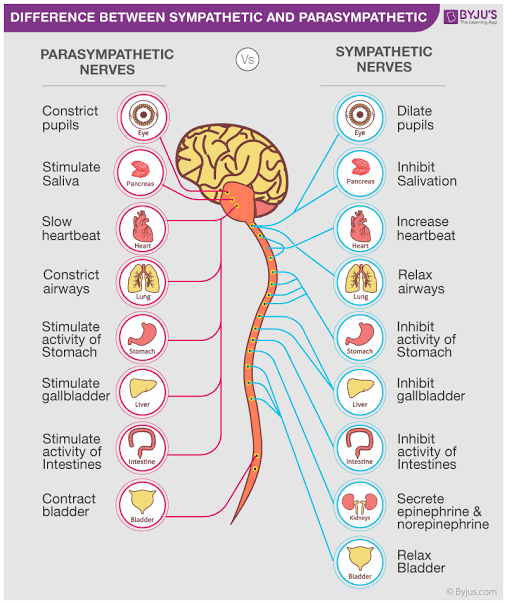
Sympathetic vs. Parasympathetic Divisions
The ANS has two anatomically and functionally distinct divisions:
| Feature | Sympathetic (Thoracolumbar) | Parasympathetic (Craniosacral) |
|---|---|---|
| Origin | Thoracolumbar outflow: T1-L2 intermediolateral cell column | Craniosacral outflow: CN III, VII, IX, X and S2-S4 |
| Ganglion location | Close to CNS — paravertebral chain or prevertebral | Close to target organ — terminal or intramural |
| Preganglionic fiber length | Short | Long |
| Postganglionic fiber length | Long | Short |
| General function | "Fight or flight" — mobilizes energy, prepares for action | "Rest and digest" — conserves energy, promotes digestion |
| Pupil | Dilates (mydriasis) | Constricts (miosis) |
| Heart | Increases rate and contractility | Decreases rate and contractility |
| Bronchi | Dilates | Constricts |
| GI tract | Decreases motility and secretion | Increases motility and secretion |
| Bladder | Relaxes detrusor, constricts sphincter | Contracts detrusor, relaxes sphincter |
| Blood vessels | Constricts (most vessels) | Dilates (few vessels only) |
Sympathetic = SYMPATHY for your body in danger (dilates pupils, speeds heart, opens airways).
Parasympathetic = PARA-dise rest (constricts pupils, slows heart, digests food).
The Sympathetic Pathway
Understanding the precise anatomical path of sympathetic fibers is essential for localizing lesions and predicting deficits.
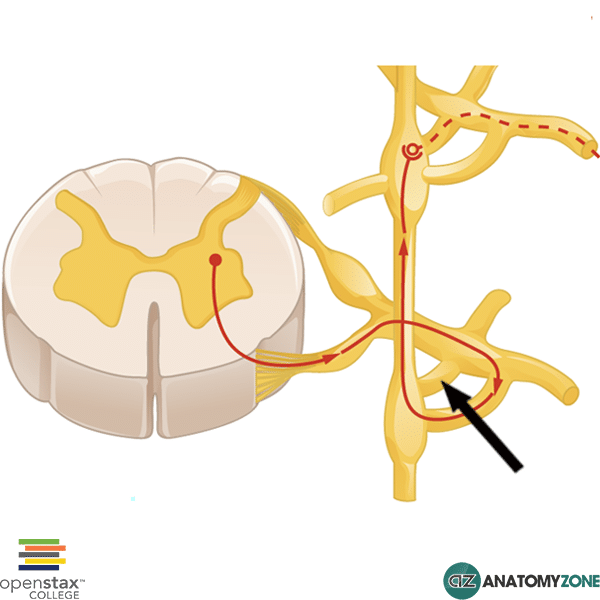
- Step 1 — Preganglionic Cell Body: Located in the intermediolateral cell column (IML) of the spinal cord gray matter, specifically at levels T1 through L2. These are the only spinal segments that give rise to sympathetic preganglionic fibers.
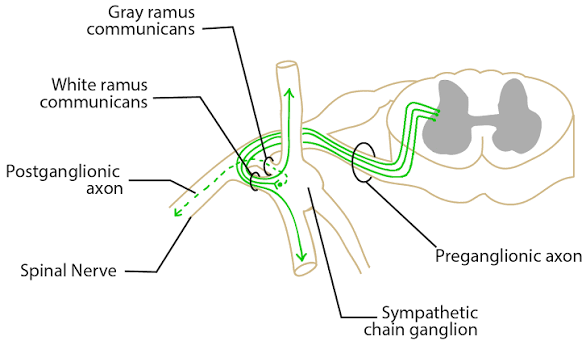
- Step 2 — Ventral Root Exit: The preganglionic axon exits the spinal cord through the ventral root alongside somatic motor fibers.
- Step 3 — White Ramus Communicans: The myelinated preganglionic axon enters the white ramus communicans (named for its white, myelinated appearance) and travels to the sympathetic trunk (paravertebral ganglia).
- Step 4 — Sympathetic Trunk Options: Once in the sympathetic trunk, the preganglionic axon has THREE possible fates:
- A. Synapse at the same level (most common for body wall targets).
- B. Ascend or descend within the sympathetic trunk to synapse at a different level (e.g., cervical ganglia for head targets, sacral ganglia for pelvic targets).
- C. Pass through without synapsing (splanchnic nerves) to reach prevertebral ganglia.
- Step 5 — Postganglionic Exit: The unmyelinated postganglionic axon exits the ganglion through the gray ramus communicans (named for its gray, unmyelinated appearance) and rejoins the spinal nerve to reach target organs.
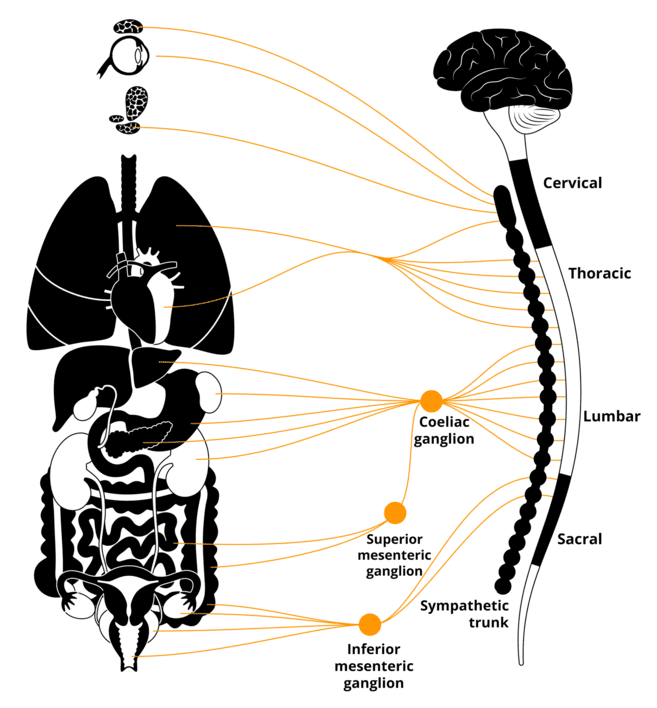
Paravertebral vs. Prevertebral Ganglia
- Paravertebral ganglia (sympathetic chain): A vertical chain of 22-23 ganglia running alongside the vertebral column from cervical to coccygeal levels. These ganglia receive preganglionic fibers for body wall structures (skin blood vessels, sweat glands, arrector pili muscles).
- Prevertebral ganglia (collateral ganglia): Located anterior to the aorta near major arterial branches. These include the celiac ganglion (foregut), superior mesenteric ganglion (midgut), and inferior mesenteric ganglion (hindgut). They receive preganglionic fibers via splanchnic nerves for visceral organs.
All spinal nerves from T1 to L2 carry white rami (preganglionic sympathetic fibers) to the sympathetic chain. ALL spinal nerves (C1 to S5) carry gray rami (postganglionic sympathetic fibers) back from the sympathetic chain. This means sympathetic postganglionic fibers reach every spinal nerve, distributing to the entire body surface.
The Parasympathetic Pathway
Parasympathetic fibers follow the craniosacral outflow — they emerge from the brainstem with cranial nerves and from the sacral spinal cord.
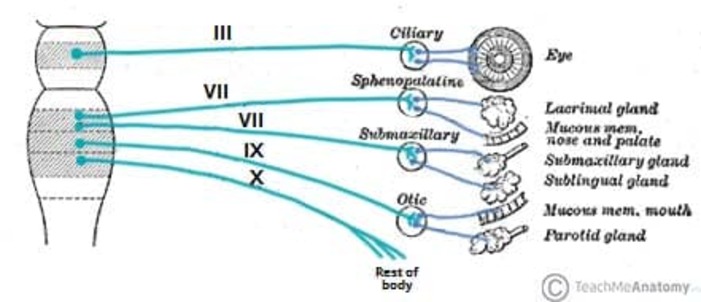
Cranial Outflow (CN III, VII, IX, X):
- CN III (Oculomotor): Preganglionic fibers arise from the Edinger-Westphal nucleus in the midbrain. They travel with CN III to the ciliary ganglion in the orbit. Postganglionic fibers innervate the ciliary muscle (accommodation) and sphincter pupillae (pupil constriction).
- CN VII (Facial): Preganglionic fibers arise from the superior salivatory nucleus in the pons. They divide into two branches:
- Greater petrosal nerve → pterygopalatine ganglion → lacrimal gland, nasal and palatine glands.
- Chorda tympani → submandibular ganglion → submandibular and sublingual salivary glands.
- CN IX (Glossopharyngeal): Preganglionic fibers arise from the inferior salivatory nucleus in the medulla. They travel with CN IX to the otic ganglion → parotid gland.
- CN X (Vagus): The MOST IMPORTANT parasympathetic nerve. Preganglionic fibers arise from the dorsal motor nucleus of vagus and nucleus ambiguus in the medulla. The vagus nerve provides parasympathetic innervation to the thoracic and abdominal viscera (heart, lungs, esophagus, stomach, small intestine, proximal colon, liver, pancreas, kidneys).
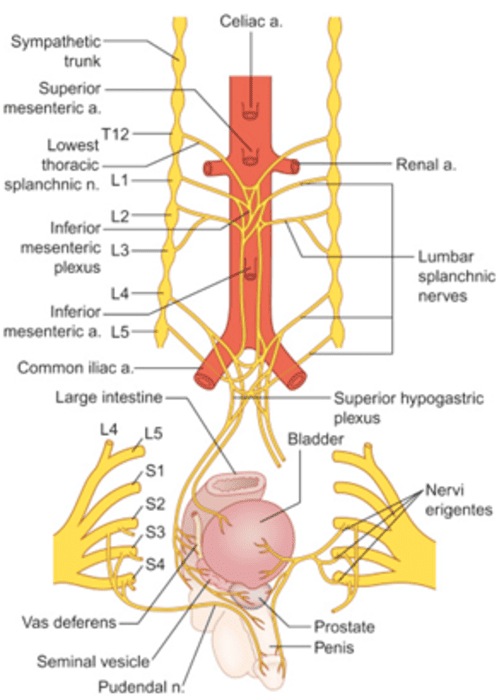
Sacral Outflow (S2-S4):
- Preganglionic cell bodies are in the intermediolateral cell column of sacral segments S2-S4.
- Axons exit through the ventral roots and form the pelvic splanchnic nerves (nervi erigentes).
- These nerves synapse in terminal ganglia (intramural ganglia within the organ walls) near or within the target organs.
- Targets: distal colon, rectum, bladder, reproductive organs.
Parasympathetic ganglia are terminal or intramural (close to or inside the target organ). This means parasympathetic postganglionic fibers are very short, while preganglionic fibers are long. The opposite is true for sympathetic fibers.
2. Visceral Afferents & Reflex Arcs (Sensory Pathways)
The ANS is not purely efferent (motor). It carries sensory information from viscera back to the CNS, enabling reflex control of autonomic functions.
Visceral Pain Pathway
Visceral pain is transmitted by visceral afferent fibers that travel alongside autonomic efferent fibers. The cell bodies of these sensory neurons are in the dorsal root ganglia, just like somatic sensory neurons.
The Pathway (Step by Step):
- Step 1 — Receptor: Nociceptors in visceral organs detect stretching, ischemia, inflammation, or chemical irritation. Visceral nociceptors are polymodal — they respond to multiple types of stimuli.
- Step 2 — Peripheral Process: The peripheral process of the pseudounipolar neuron travels with autonomic fibers to the target organ. For the heart and lungs, it travels with the vagus nerve. For abdominal organs, it travels with splanchnic nerves.
- Step 3 — Central Process: The central process enters the spinal cord through the dorsal root and synapses in the dorsal horn (laminae I and V), specifically in the same segments that receive somatic input from the corresponding dermatome.
- Step 4 — Ascent to Brain: Second-order neurons cross the midline and ascend in the spinothalamic tract (anterolateral system) to the thalamus, then to the somatosensory cortex.
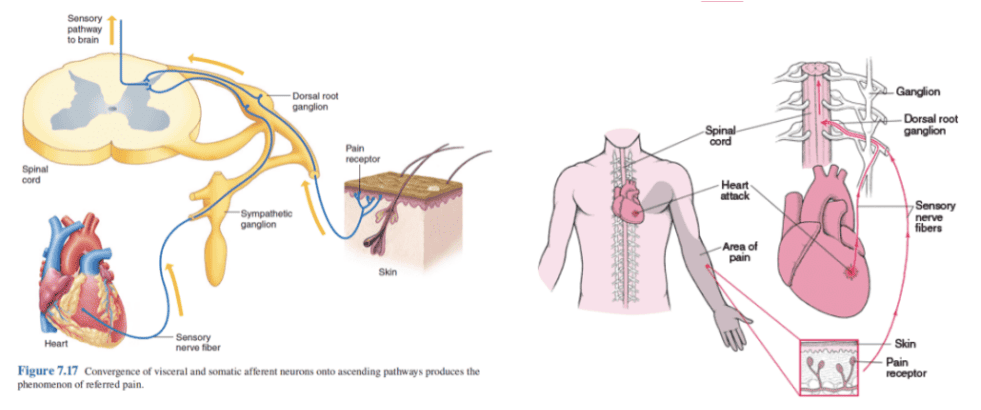
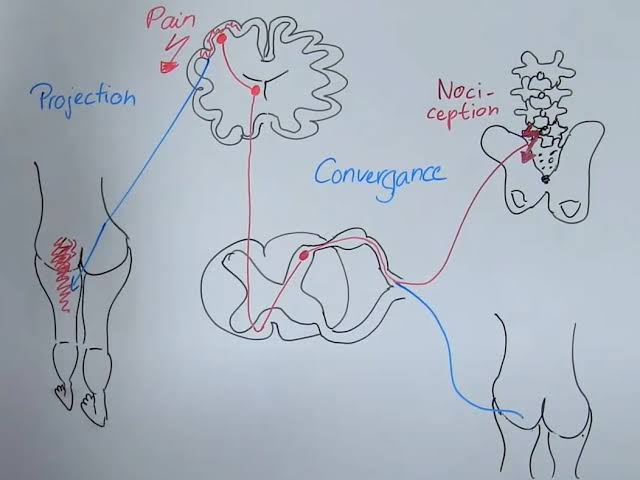
Referred Pain — The Convergence Theory
Referred pain is the phenomenon where visceral pain is perceived as originating from a somatic structure (usually the body wall). This occurs because visceral and somatic sensory fibers converge on the same second-order neurons in the dorsal horn.
The Mechanism:
- Visceral afferent fibers and somatic afferent fibers from the same spinal segment (same dermatome) synapse on the same projection neurons in the dorsal horn.
- The brain cannot distinguish the source of the input. Because the brain is more accustomed to receiving pain signals from the body surface (somatic), it misinterprets visceral pain as somatic pain.
- The pain is typically referred to the dermatome that shares the same spinal segment as the visceral organ.
Classic Examples of Referred Pain:
| Visceral Organ | Spinal Segment | Referred to |
|---|---|---|
| Heart | T1-T5 | Left chest, left arm, left jaw (angina pectoris) |
| Stomach | T6-T9 | Epigastrium (upper central abdomen) |
| Gallbladder | T7-T9 | Right upper quadrant, right scapula (biliary colic) |
| Appendix | T10 | Periumbilical area (early appendicitis) |
| Ureter | T11-L2 | Groin, testicle/labium (renal colic) |
| Urinary bladder | S2-S4 | Perineum, suprapubic area |
Early appendicitis pain is felt around the umbilicus (T10 dermatome) because the appendix and umbilicus share the same spinal segment. Only when inflammation spreads to the parietal peritoneum (which has somatic innervation) does the pain localize to the right lower quadrant (McBurney's point).
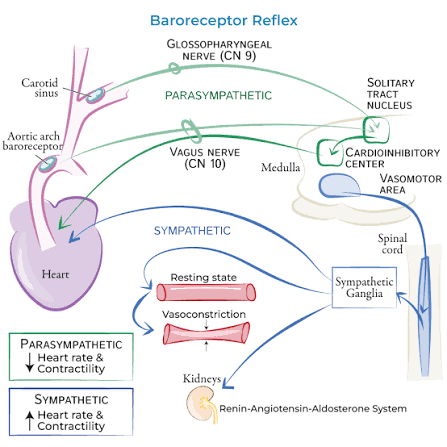
The Baroreceptor Reflex Arc
The baroreceptor reflex is the primary mechanism for short-term blood pressure regulation. It is a negative feedback loop that maintains arterial pressure within a narrow range.
- Step 1 — Sensory Receptors:
- Carotid sinus baroreceptors: Located at the bifurcation of the common carotid artery. They detect changes in arterial pressure in the carotid circulation.
- Aortic arch baroreceptors: Located in the wall of the aortic arch. They detect changes in systemic arterial pressure.
- Both are stretch receptors — they fire more action potentials when the vessel wall is stretched by high pressure, and fewer when pressure drops.
- Step 2 — Sensory Nerves:
- Carotid sinus → Glossopharyngeal nerve (CN IX) → inferior ganglion of CN IX → nucleus tractus solitarius (NTS) in the medulla.
- Aortic arch → Vagus nerve (CN X) → inferior (nodose) ganglion of CN X → nucleus tractus solitarius (NTS) in the medulla.
- Step 3 — Brainstem Integration (NTS):
- The nucleus tractus solitarius (NTS) is the primary cardiovascular control center in the medulla. It receives baroreceptor input and integrates it with other autonomic signals.
- The NTS has two output pathways:
— Cardioinhibitory center (dorsal motor nucleus of vagus + nucleus ambiguus) → increases parasympathetic output to the heart.
— Vasomotor center (rostral ventrolateral medulla, RVLM) → modulates sympathetic output to the heart and blood vessels.
- Step 4 — Motor Response (When Blood Pressure RISES):
- Increased baroreceptor firing → NTS activation → parasympathetic activation (vagus nerve) → decreases heart rate and contractility.
- Simultaneously, NTS inhibits the vasomotor center → decreased sympathetic tone → vasodilation and reduced cardiac output.
- Result: Blood pressure returns to normal.
- Step 4 — Motor Response (When Blood Pressure DROPS):
- Decreased baroreceptor firing → NTS is less activated → parasympathetic withdrawal → heart rate increases.
- Simultaneously, vasomotor center is disinhibited → increased sympathetic tone → vasoconstriction, increased heart rate, and increased contractility.
- Result: Blood pressure returns to normal.
Carotid Sinus Massage
Gentle pressure on the carotid sinus stimulates baroreceptors, increasing their firing rate. The NTS interprets this as high blood pressure and activates the parasympathetic response → bradycardia and hypotension. This is used therapeutically to terminate certain supraventricular tachycardias, but can be dangerous in patients with carotid artery disease.
3. Regional Anatomy & Special Pathways (The "Local" Networks)
This section covers the unique autonomic pathways that serve specific regions and organs. These pathways do not follow the general rules and require separate memorization.
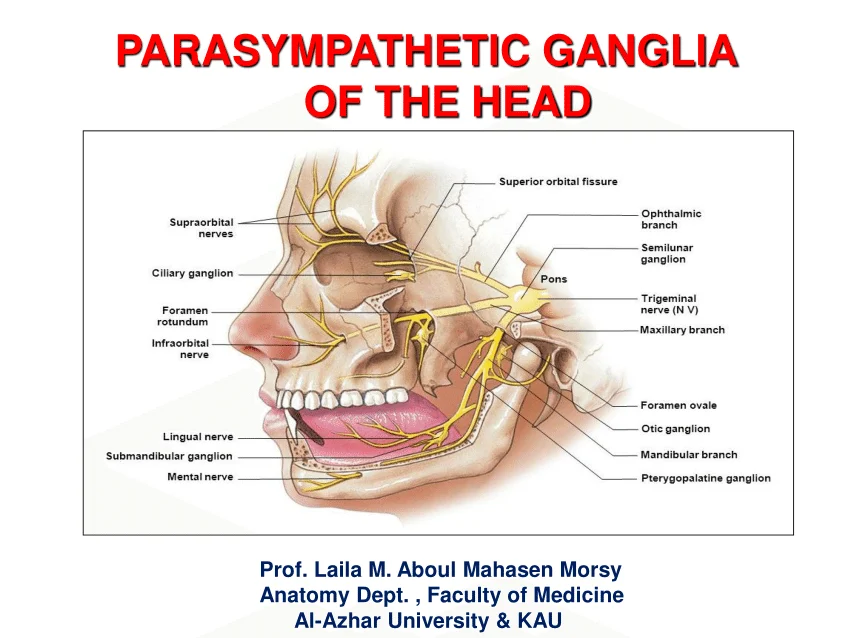
A. The Four Cranial Parasympathetic Ganglia
All four parasympathetic ganglia of the head are located near the foramina through which their associated cranial nerves exit the skull. Each has a specific preganglionic source, postganglionic branch, and target organ.
| Ganglion | Preganglionic Source | Postganglionic Branch | Target Organ |
|---|---|---|---|
| Ciliary | Edinger-Westphal nucleus (midbrain) via CN III | Short ciliary nerves | Ciliary muscle (accommodation) and sphincter pupillae (miosis) |
| Pterygopalatine (sphenopalatine) | Superior salivatory nucleus (pons) via CN VII → greater petrosal nerve | Branches of maxillary nerve (V2) | Lacrimal gland, nasal glands, palatine glands |
| Submandibular | Superior salivatory nucleus (pons) via CN VII → chorda tympani | Lingual nerve (branch of V3) | Submandibular and sublingual salivary glands |
| Otic | Inferior salivatory nucleus (medulla) via CN IX → lesser petrosal nerve | Auriculotemporal nerve (branch of V3) | Parotid gland |
- "III is for Ciliary (C = 3rd letter) — both start with C sounds"
- "VII is for Pterygopalatine and Submandibular — two ganglia, two branches"
- "IX is for Otic — both have one syllable, one ganglion"
- "X is for Viscera — the vagus serves everything else!"
All four ganglia receive sensory fibers from the trigeminal nerve (V) and sympathetic postganglionic fibers from the superior cervical ganglion. These fibers simply pass through the ganglia without synapsing. Only parasympathetic fibers synapse in these ganglia.
B. Splanchnic Nerves
Splanchnic nerves are the sympathetic pathways to the thoracic and abdominal viscera. They carry preganglionic fibers that bypass the sympathetic chain to reach prevertebral ganglia.
Cardiopulmonary Splanchnic Nerves:
- These arise from the upper thoracic sympathetic ganglia (T1-T5).
- They carry postganglionic sympathetic fibers (already synapsed in the sympathetic chain) directly to the heart and lungs.
- The cardiac plexus receives fibers from both sympathetic (T1-T5) and parasympathetic (vagus) sources.
- Sympathetic stimulation increases heart rate and contractility; parasympathetic (vagal) stimulation decreases them.
Abdominopelvic Splanchnic Nerves:
These carry preganglionic sympathetic fibers that pass through the sympathetic chain WITHOUT synapsing, then travel to prevertebral ganglia.
| Nerve | Origin | Prevertebral Ganglion | Target Organs |
|---|---|---|---|
| Greater splanchnic | T5-T9 (or T5-T10) | Celiac ganglion | Stomach, liver, gallbladder, spleen, proximal duodenum, pancreas (foregut organs) |
| Lesser splanchnic | T10-T11 | Aorticorenal ganglion (superior mesenteric) | Small intestine, ascending colon, proximal transverse colon (midgut organs) |
| Least splanchnic | T12 | Renal plexus / aorticorenal ganglion | Kidneys, ureters, gonads |
| Lumbar splanchnic | L1-L2 | Inferior mesenteric ganglion | Distal colon, rectum, bladder, reproductive organs (hindgut/pelvic organs) |
- "Greater = Gut (stomach, liver) — T5-T9"
- "Lesser = Lower gut (small intestine) — T10-T11"
- "Least = Leftovers (kidneys, gonads) — T12"
- "Lumbar = Lower everything (colon, bladder, pelvis) — L1-L2"
C. Unique Innervation of the Adrenal Medulla
The adrenal medulla is a unique structure that functions as a modified sympathetic ganglion. It is the only autonomic target organ that receives direct preganglionic sympathetic innervation without an intervening postganglionic neuron.
Why No Postganglionic Neuron?
- During embryonic development, neural crest cells migrate to the adrenal gland and differentiate into chromaffin cells.
- These chromaffin cells are essentially postganglionic sympathetic neurons that have lost their axons and dendrites.
- Instead of releasing neurotransmitter at a synapse, they release hormones (epinephrine and norepinephrine) directly into the bloodstream.
- Therefore, the preganglionic sympathetic fiber (from T5-T11 via the greater splanchnic nerve) synapses directly on chromaffin cells — there is no separate postganglionic neuron.
The Pathway:
Preganglionic neuron (IML T5-T11) → white ramus → sympathetic chain (passes through without synapsing) → greater splanchnic nerve → celiac plexus → adrenal medulla → synapses on chromaffin cells.
Neurotransmitter: Preganglionic fibers release acetylcholine (ACh) onto nicotinic receptors on chromaffin cells — the same neurotransmitter used at ALL autonomic ganglia.
Hormone Release: Chromaffin cells release approximately 80% epinephrine (adrenaline) and 20% norepinephrine (noradrenaline) into the bloodstream. These hormones act on adrenergic receptors throughout the body, producing a systemic "fight or flight" response.
Pheochromocytoma
A pheochromocytoma is a tumor of chromaffin cells (usually in the adrenal medulla) that secretes excessive catecholamines. Patients present with episodic hypertension, tachycardia, sweating, and anxiety. The classic triad is headache, palpitations, and sweating. Diagnosis is confirmed by elevated urinary catecholamines or metanephrines.
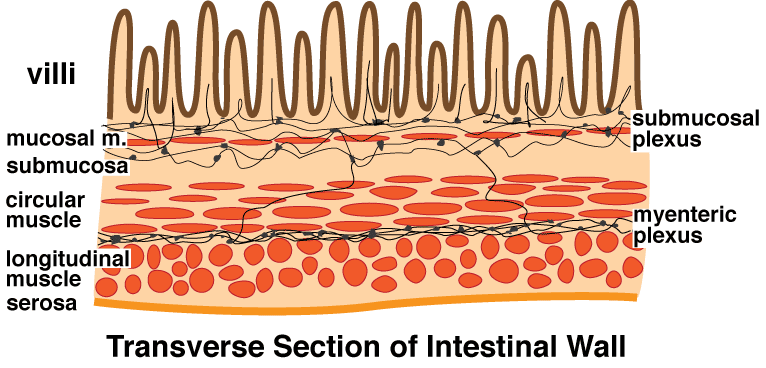
D. The Enteric Nervous System (The "Second Brain")
The enteric nervous system is an extensive network of neurons and glial cells within the wall of the gastrointestinal tract. It can function independently of the CNS, though it is modulated by sympathetic and parasympathetic input.
Structure of the Gut Wall (from lumen outward):
- Mucosa: Epithelium, lamina propria, muscularis mucosae
- Submucosa: Connective tissue, blood vessels, Meissner's plexus
- Muscularis externa: Inner circular layer, outer longitudinal layer, Auerbach's plexus
- Serosa/Adventitia: Outer connective tissue layer
The Two Enteric Plexuses:
- Myenteric (Auerbach's) plexus: Located between the inner circular and outer longitudinal muscle layers of the muscularis externa. It primarily controls GI motility (peristalsis, segmentation, sphincter tone). It contains excitatory motor neurons (release ACh, substance P) and inhibitory motor neurons (release nitric oxide, VIP).
- Submucosal (Meissner's) plexus: Located in the submucosa. It primarily controls GI secretion and absorption (glandular secretion, local blood flow, mucosal immune responses).
Extrinsic Innervation of the Gut:
- Parasympathetic (vagus and pelvic splanchnic): Increases GI motility and secretion. Preganglionic fibers synapse on enteric ganglion cells.
- Sympathetic (splanchnic nerves): Decreases GI motility and secretion. Postganglionic fibers primarily inhibit enteric neurons and constrict splanchnic blood vessels.
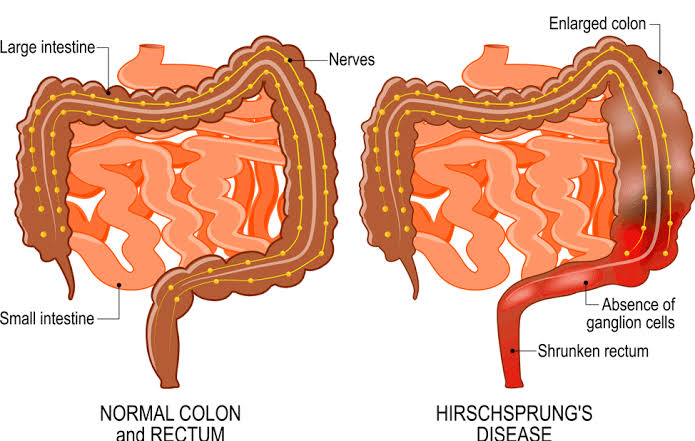
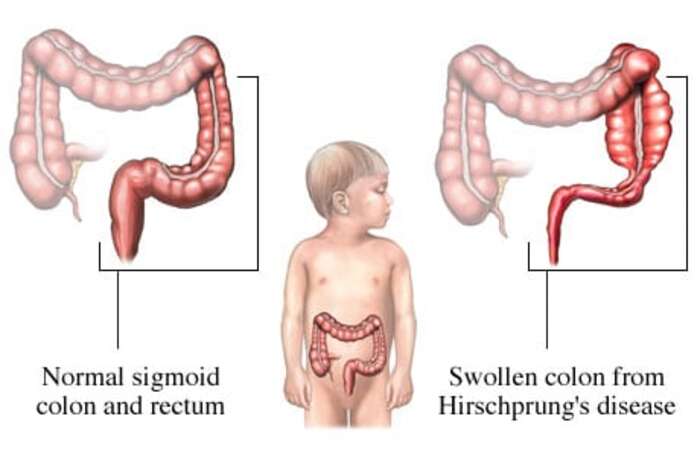
Hirschsprung Disease
Hirschsprung disease (congenital aganglionic megacolon) is caused by the failure of neural crest cells to migrate to the distal colon during embryonic development (weeks 5-12). The aganglionic segment (usually the rectosigmoid region) lacks both myenteric and submucosal plexuses.
Without enteric ganglia, the affected bowel segment cannot relax. It remains in a state of tonic contraction, creating a functional obstruction. Proximal to the obstruction, the colon becomes massively dilated (megacolon).
Clinical Presentation: Newborns fail to pass meconium within 48 hours. Older infants present with chronic constipation, abdominal distension, and failure to thrive. The rectal examination reveals a tight anal sphincter and an empty rectal ampulla (because stool is trapped proximal to the obstruction).
4. Pharmacology & Chemical Mapping (Neurotransmitters & Receptors)
Understanding the chemical coding of the ANS is essential for pharmacology, anesthesia, and clinical medicine. Every drug that affects autonomic function works by mimicking or blocking these neurotransmitters and receptors.
Neurotransmitters in the ANS
There are only two primary neurotransmitters in the peripheral autonomic nervous system: acetylcholine (ACh) and norepinephrine (NE). Their distribution follows a simple but critical rule.
Acetylcholine (ACh) is released at:
- ALL preganglionic synapses — both sympathetic and parasympathetic ganglia.
- ALL parasympathetic postganglionic synapses — every parasympathetic target organ.
- SOME sympathetic postganglionic synapses — specifically sweat glands and arrector pili muscles (these are cholinergic sympathetic fibers, an exception to the rule).
- Neuromuscular junction — somatic motor to skeletal muscle (not autonomic, but same neurotransmitter).
Norepinephrine (NE) is released at:
- MOST sympathetic postganglionic synapses — all sympathetic target organs EXCEPT sweat glands and arrector pili.
- Adrenal medulla — chromaffin cells release NE and epinephrine into the bloodstream as hormones.
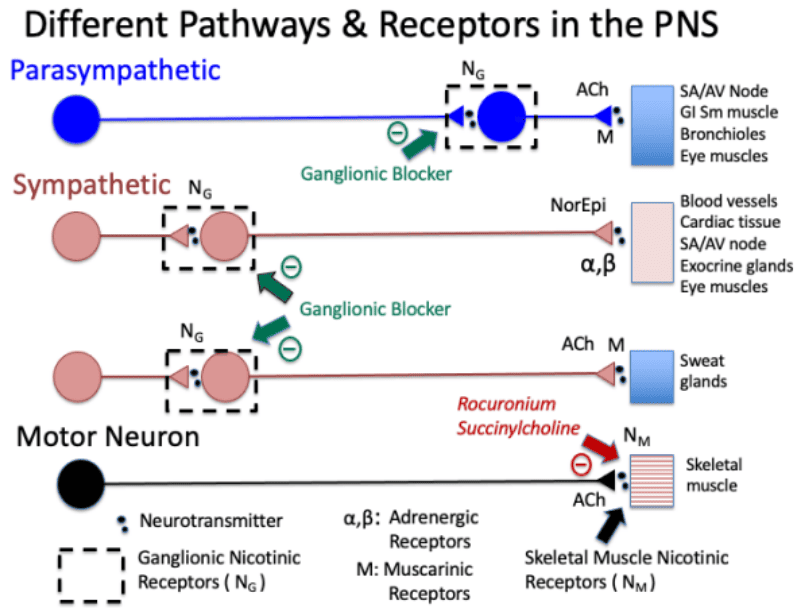
Receptor Types and Locations
Autonomic receptors are divided into two major classes: cholinergic (respond to ACh) and adrenergic (respond to NE and epinephrine).
Cholinergic Receptors:
- Nicotinic receptors (N): Ionotropic (ligand-gated ion channels). Found at:
- All autonomic ganglia (both sympathetic and parasympathetic) — these are Nn (neuronal nicotinic) receptors.
- Neuromuscular junction — these are Nm (muscle nicotinic) receptors.
- Adrenal medulla chromaffin cells.
- Muscarinic receptors (M): Metabotropic (G-protein coupled). Found at:
- All parasympathetic target organs (heart, smooth muscle, glands).
- Sweat glands (sympathetic cholinergic fibers).
- Five subtypes (M1-M5), but M2 (heart) and M3 (smooth muscle, glands) are most clinically relevant.
Adrenergic Receptors:
- Alpha-1 (α1): Gq-coupled. Causes vasoconstriction (arteries, veins), contraction of smooth muscle (iris dilator, bladder sphincter, prostate), and glycogenolysis (liver).
- Alpha-2 (α2): Gi-coupled. Found on presynaptic terminals (autoreceptors that inhibit further NE release) and on platelets (promotes aggregation) and pancreatic beta cells (inhibits insulin secretion).
- Beta-1 (β1): Gs-coupled. Found primarily in the heart (increases rate, contractility, conduction velocity) and kidney (promotes renin release).
- Beta-2 (β2): Gs-coupled. Found in bronchial smooth muscle (causes dilation), vascular smooth muscle (causes dilation in skeletal muscle vessels), and uterus (causes relaxation).
- Beta-3 (β3): Gs-coupled. Found in adipose tissue (promotes lipolysis) and bladder detrusor muscle (causes relaxation).
Organ-Specific Receptor Distribution:
| Organ/System | Receptor | Effect of Activation |
|---|---|---|
| Heart | β1 (dominant), M2 | β1: increases rate and contractility; M2: decreases rate and contractility |
| Blood vessels (most) | α1 | Vasoconstriction |
| Blood vessels (coronary, skeletal muscle) | β2 | Vasodilation |
| Bronchi | β2 (dilation), M3 (constriction) | β2: bronchodilation; M3: bronchoconstriction |
| GI tract smooth muscle | M3 (contraction), α2, β2 (relaxation) | M3: increases motility; α2/β2: decreases motility |
| GI tract sphincters | α1 (contraction), M3 (relaxation) | α1: closes sphincter; M3: opens sphincter |
| Bladder detrusor | M3 (contraction), β2/β3 (relaxation) | M3: promotes voiding; β: promotes storage |
| Bladder sphincter | α1 (contraction), M3 (relaxation) | α1: prevents voiding; M3: allows voiding |
| Pupil | α1 (dilator), M3 (sphincter) | α1: mydriasis; M3: miosis |
| Ciliary muscle | M3 | Accommodation for near vision |
- "Alpha-1 = ONE vessel constrictor (vascular smooth muscle)"
- "Beta-1 = ONE heart (one heart per person)"
- "Beta-2 = TWO lungs (two lungs) — bronchodilation"
- "Beta-3 = THREE fat cells (adipose tissue) — lipolysis"
5. Clinical Anatomical Correlations (Pathology & Lesions)
This section applies anatomical knowledge to predict clinical signs from specific autonomic lesions. This is the highest-yield material for exams and clinical practice.
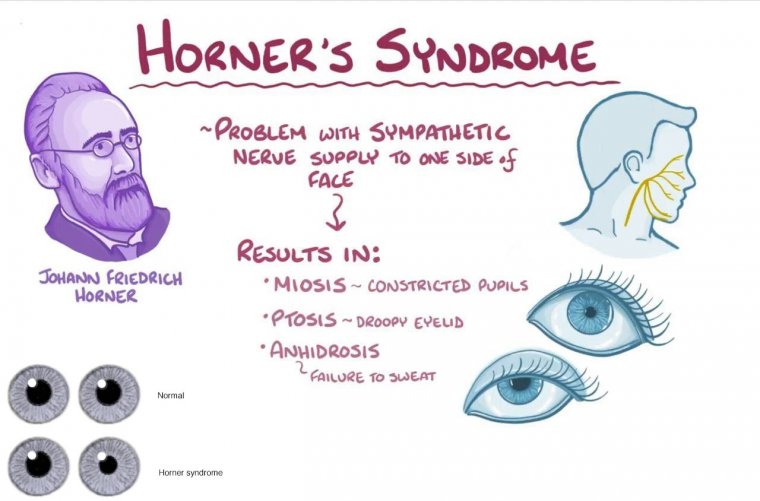
A. Horner's Syndrome
Horner's syndrome results from interruption of the cervical sympathetic pathway anywhere along its three-neuron chain. It produces a characteristic triad of ipsilateral signs.
The Cervical Sympathetic Pathway (Three Neurons):
- 1st order neuron (Central): Descends from the hypothalamus through the brainstem and lateral funiculus of the spinal cord to synapse in the IML at T1-T2.
- 2nd order neuron (Preganglionic): Cell body in IML T1-T2. Axon exits via ventral root → white ramus → sympathetic chain → ascends to superior cervical ganglion (C1-C2 level).
- 3rd order neuron (Postganglionic): Cell body in superior cervical ganglion. Axons travel with the internal carotid artery (to eye and forehead) and external carotid artery (to face and neck).
The Classic Triad:
- Ptosis (drooping of the upper eyelid): Due to loss of sympathetic innervation to Muller's muscle (superior tarsal muscle), which assists the levator palpebrae in elevating the eyelid. The ptosis is partial (not complete, unlike oculomotor nerve palsy).
- Miosis (constricted pupil): Due to loss of sympathetic innervation to the dilator pupillae muscle. The pupil cannot dilate properly. In dim light, the affected pupil remains smaller than the normal pupil (anisocoria is more pronounced in darkness).
- Anhidrosis (absence of sweating): Due to loss of sympathetic innervation to sweat glands on the ipsilateral face and neck. The distribution of anhidrosis depends on which part of the pathway is damaged — postganglionic lesions affect only the forehead, while preganglionic lesions affect the entire face.

Localization of the Lesion:
- Central (1st order) lesion: Caused by lateral medullary syndrome (Wallenberg), syringomyelia, or brainstem stroke. May have associated brainstem signs (vertigo, ataxia, dysphagia).
- Preganglionic (2nd order) lesion: Caused by Pancoast tumor (apical lung cancer), cervical rib, or brachial plexus injury. May have associated arm pain or weakness.
- Postganglionic (3rd order) lesion: Caused by internal carotid artery dissection, cavernous sinus thrombosis, or cluster headache. May have associated neck pain or headache. Anhidrosis is limited to the forehead because only the internal carotid plexus is affected.
Pharmacologic Testing for Horner's Syndrome
- Cocaine eye drops: In a normal eye, cocaine blocks NE reuptake and causes pupil dilation. In Horner's syndrome, there is no NE to reuptake, so the pupil does NOT dilate. This confirms the diagnosis.
- Hydroxyamphetamine eye drops: This drug releases NE from nerve terminals. If the lesion is preganglionic (2nd order), the postganglionic terminal is intact and releases NE → pupil dilates. If the lesion is postganglionic (3rd order), the terminal is damaged → pupil does NOT dilate. This distinguishes 2nd from 3rd order lesions.