ADRENAL GLAND FUNCTIONS AND REGULATION
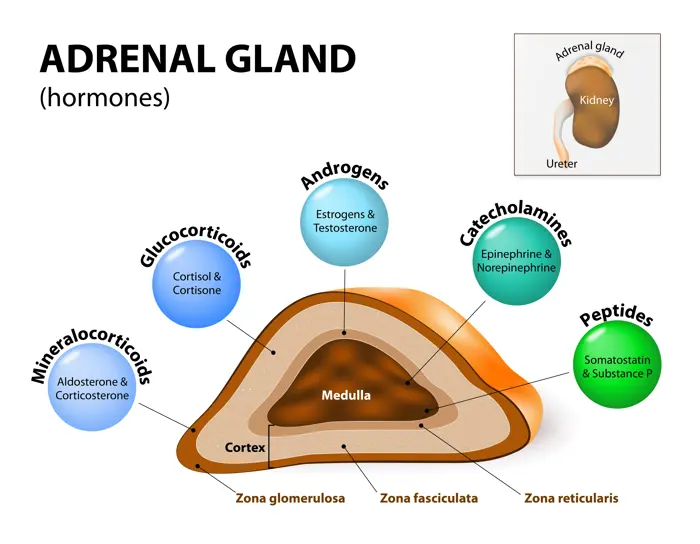
The adrenal glands, also known as suprarenal glands, are a pair of small, triangular-shaped endocrine glands located on top of each kidney (ad-renal, meaning "near the kidney"). Despite their small size, these glands are absolutely vital for life, playing a central role in managing stress, regulating metabolism, blood pressure, fluid balance, and even influencing immune function and sexual development.
The adrenal gland is not a single, homogenous organ but rather a composite of two distinct endocrine glands, each with unique origins, structures, and hormonal secretions. These two compartments are:
- The Adrenal Cortex (Outer Layer)
- The Adrenal Medulla (Inner Layer)
These two regions, though anatomically juxtaposed, function almost as separate organs, producing different classes of hormones that contribute synergistically to the body's complex physiological responses.
I. THE ADRENAL GLAND: TWO DISTINCT COMPARTMENTS
A. The Adrenal Cortex (Outer Layer)
The adrenal cortex is the outer, yellowish layer of the adrenal gland, accounting for approximately 80-90% of the gland's total mass. It is derived from embryonic mesoderm and is responsible for synthesizing and secreting a class of steroid hormones known as corticosteroids. These hormones are all synthesized from cholesterol and are lipid-soluble, allowing them to easily pass through cell membranes to exert their effects.
The adrenal cortex is further subdivided into three distinct layers or zones, each characterized by its unique cellular structure, enzymatic machinery, and primary hormonal products. These layers are arranged concentrically, starting from the outermost layer just beneath the capsule, and moving inward towards the medulla:
1. Zona Glomerulosa (15% of the Cortex)
- Location: Outermost layer, directly beneath the adrenal capsule. Cells arranged in small, spherical or arched clusters (glomeruli).
- Primary Hormones: Sole site of mineralocorticoid synthesis, with aldosterone being the most important.
- Function of Aldosterone: Regulates mineral balance (sodium and potassium). Main actions on kidneys:
- Sodium (Na+) reabsorption: Leads to water retention, maintaining blood volume/pressure.
- Potassium (K+) excretion: Essential for maintaining normal potassium levels.
- Hydrogen (H+) excretion: Contributing to acid-base balance.
- Regulation: Primarily regulated by the Renin-Angiotensin-Aldosterone System (RAAS) and plasma potassium concentration. ACTH has a permissive role.
2. Zona Fasciculata (75% of the Cortex)
- Location: Middle and largest layer. Cells arranged in long, straight cords or fascicles. Cells are often called "spongiocytes" due to vacuolated appearance from abundant lipid droplets (cholesterol esters).
- Primary Hormones: Primary site of glucocorticoid synthesis, with cortisol (hydrocortisone) being the most important. Small amounts of adrenal androgens are also produced here.
- Function of Cortisol: Crucial "stress hormone".
- Glucose Metabolism: Promotes gluconeogenesis; decreases peripheral glucose utilization.
- Protein Metabolism: Increases protein catabolism (breakdown).
- Fat Metabolism: Promotes lipolysis.
- Anti-inflammatory/Immunosuppressive: Suppresses immune responses.
- Regulation: Primarily regulated by ACTH (from anterior pituitary), which is regulated by CRH (from hypothalamus). Forms the HPA axis.
3. Zona Reticularis (10% of the Cortex)
- Location: Innermost layer, adjacent to the medulla. Cells arranged in an irregular, anastomosing network (reticular).
- Primary Hormones: Primary site of adrenal androgen synthesis. Includes dehydroepiandrosterone (DHEA) and androstenedione (weak androgens). Some glucocorticoids produced here.
- Function of Androgens: Contribute to secondary sexual characteristics (pubic/axillary hair, libido). In males, masked by testicular androgens. In females, DHEA is a significant estrogen precursor.
- Regulation: Primarily regulated by ACTH.
B. The Adrenal Medulla (Inner Layer)
The adrenal medulla is the central, reddish-brown core of the adrenal gland, completely surrounded by the adrenal cortex. It comprises about 10-20% of the gland's total mass.
- Nature: Embryologically derived from neuroectoderm (neural crest cells), making it essentially a specialized sympathetic ganglion. Cells are called chromaffin cells (modified postganglionic sympathetic neurons).
- Innervation: Directly innervated by preganglionic sympathetic fibers (cholinergic). Allows rapid release of hormones in response to acute stress.
- Primary Hormones: Synthesizes and secretes catecholamines:
- Epinephrine (Adrenaline): ~80% of secretion.
- Norepinephrine (Noradrenaline): ~20% of secretion.
- Dopamine: Smaller amounts.
- Function: Central to the "fight-or-flight" response.
- Cardiovascular: Increased heart rate, contraction force, and blood pressure.
- Metabolic: Increased blood glucose (glycogenolysis/gluconeogenesis), lipolysis.
- Respiratory: Bronchodilation.
- Blood Flow: Shunting blood to muscles and brain.
- Regulation: Regulated by direct neural stimulation from the sympathetic nervous system in response to stress (pain, fear, hypoglycemia, etc.).
III. GLUCOCORTICOIDS: CORTISOL AND ITS ACTIONS
Glucocorticoids, with cortisol being the prime example, are powerful steroid hormones essential for life. Produced by the zona fasciculata and zona reticularis.
Regulation of Cortisol Secretion (HPA Axis):
- CRH (Corticotropin-Releasing Hormone): Secreted by the hypothalamus. Major regulator of ACTH secretion.
- ACTH (Adrenocorticotropic Hormone): Released from anterior pituitary. Stimulates cortisol synthesis/secretion.
- ADH (Vasopressin): A potent ACTH secretagogue, especially during stress.
- Pulsatile Secretion: Leads to diurnal (24-hour) variations. Peak activity is in the early morning (6-8 AM), diminishing to a nadir around midnight.
- Negative Feedback: Cortisol exerts negative feedback on both the hypothalamus (inhibiting CRH) and anterior pituitary (inhibiting ACTH).
Actions of Glucocorticoids (Cortisol):
1. Metabolic Response to Fasting (Anti-insulin Effects)
Cortisol promotes processes ensuring glucose availability during stress or fasting.
- Gluconeogenesis: Increases enzymes in the liver; mobilizes amino acids from muscle.
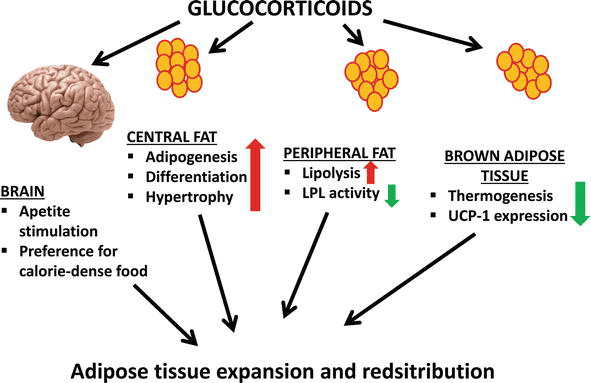
- Mobilization of Stored Fat: Promotes lipolysis, releasing free fatty acids (FFA) for energy and glycerol for gluconeogenesis.
- Muscle Cell: Promotes proteolysis (protein breakdown) releasing amino acids. Reduces protein synthesis.
- Fat Cell: Promotes lipolysis (releasing FFA and glycerol). Can promote lipogenesis in central areas.
- Liver Cell: Takes up amino acids/glycerol. Stimulates gluconeogenesis and glycogen synthesis.
- Overall Effect: Increase in circulating glucose (hyperglycemia) and free fatty acids (FFA).
2. Anti-inflammatory and Immunosuppressive Effects
Cortisol suppresses immune responses, inhibits pro-inflammatory cytokines, stabilizes lysosomal membranes, and decreases capillary permeability. Synthetic glucocorticoids are widely used as anti-inflammatory medications.
3. Other Important Actions
- Cardiovascular: Increases cardiac output; enhances vasoconstrictive effects of catecholamines (permissive action).
- Bone Metabolism: Chronic high levels inhibit bone formation, accelerate resorption (osteoporosis).
- Connective Tissue: Decreases collagen synthesis.
- CNS: Affects mood/behavior. High levels: insomnia, irritability, psychosis. Low levels: fatigue, depression.
- Gastrointestinal: Increases gastric acid secretion.
IV. ADRENAL FUNCTION ANOMALIES
A. CUSHING'S SYNDROME: EXCESSIVE GLUCOCORTICOIDS
Clinical condition resulting from prolonged exposure to excessively high levels of glucocorticoids (cortisol).
Causes of Cushing's Syndrome:
1. Pharmacologic (Exogenous)
- Most common cause. Results from therapeutic administration of exogenous glucocorticoids (e.g., prednisone) for autoimmune/inflammatory diseases.
2. Endogenous (Body's own overproduction)
- a. Cushing's Disease (Pituitary Adenoma): 75-90% of endogenous cases. Caused by a benign pituitary tumor secreting excessive ACTH. Leads to bilateral adrenal hyperplasia.
- Profile: High ACTH, High Cortisol.
- b. Adrenal Adenoma/Carcinoma (Primary Adrenal): Tumor within the adrenal gland autonomously secreting cortisol.
- Profile: Low ACTH (suppressed), High Cortisol.
- c. Ectopic ACTH Production: Non-pituitary tumor (e.g., small cell lung cancer) secreting ACTH.
- Profile: Very High ACTH, Very High Cortisol. Rapid onset.
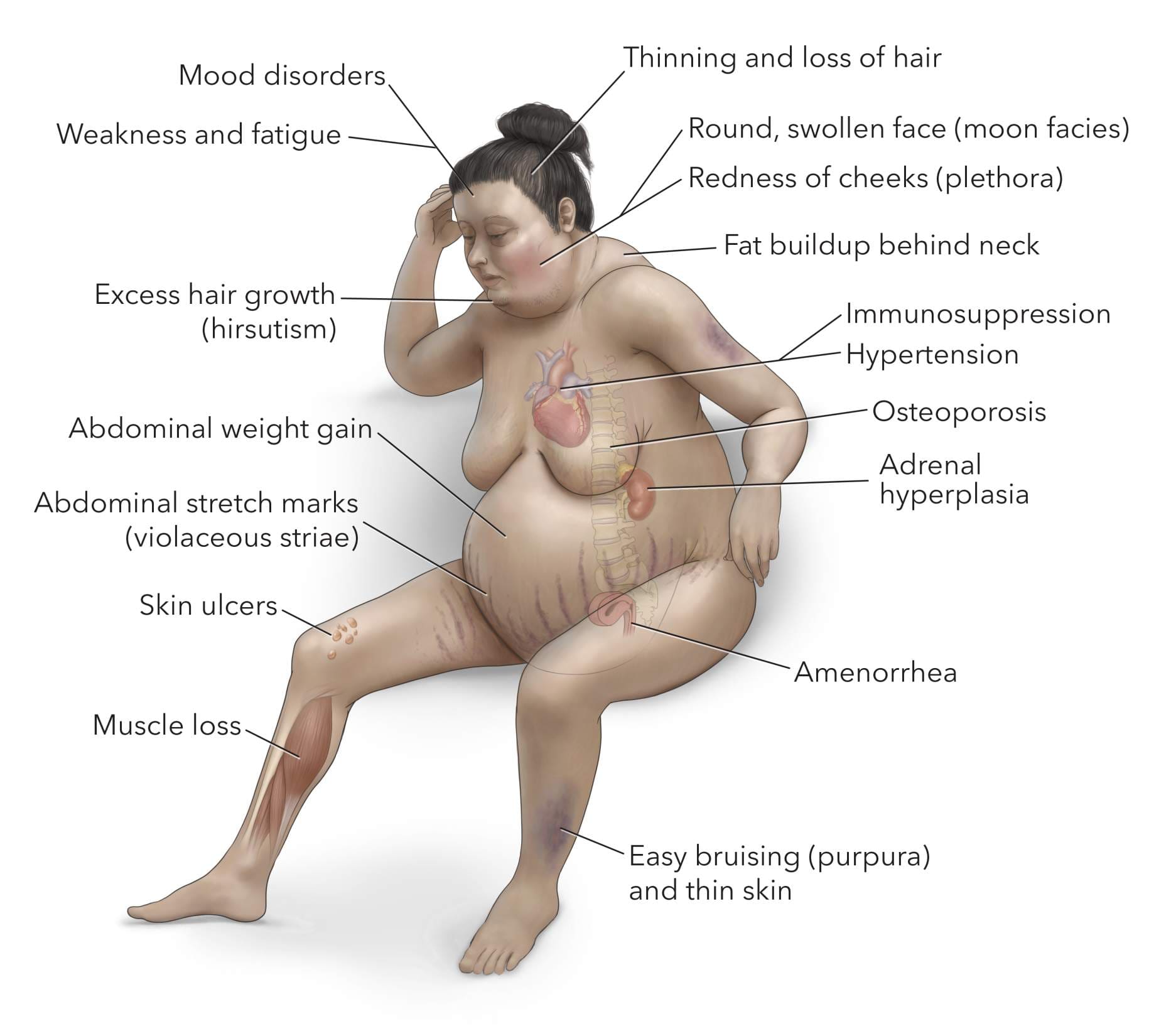
Clinical Signs and Symptoms:
Body Fat Redistribution
- Central Obesity: Fat in trunk, thin extremities.
- Buffalo Hump: Fat pad between shoulders/neck.
- Moon Facies: Rounded, plethoric face.
Skin Changes
- Purple Striae: Broad stretch marks (abdomen, thighs).
- Thin, Fragile Skin: Easy bruising.
- Hirsutism & Acne: Due to androgenic effects.
Metabolic Derangements
- Hyperglycemia: Adrenal diabetes.
- Muscle Wasting: Proximal muscle weakness (proteolysis).
- Osteoporosis: Increased fracture risk.
Cardiovascular & Other
- Hypertension: Fluid retention, catecholamine sensitivity.
- Psychiatric: Mood swings, psychosis.
- Immune Suppression: Infections.
- Reproductive: Menstrual irregularities, decreased libido.
B. ADRENOCORTICAL INSUFFICIENCY: DEFICIENT GLUCOCORTICOIDS
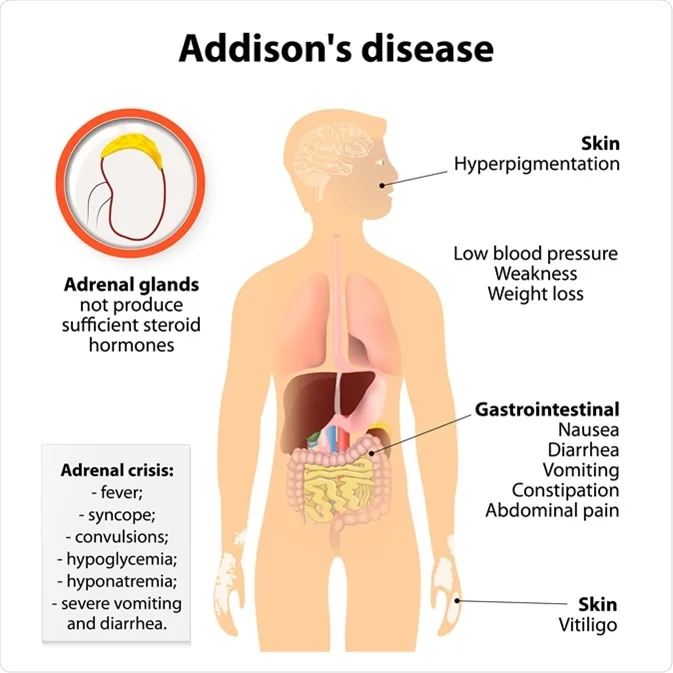
1. Primary Adrenocortical Insufficiency (Addison's Disease)
Disorder where the adrenal glands themselves are damaged and cannot produce hormones.
- Causes:
- Autoimmune Adrenalitis: Most common cause (80-90%).
- Infections: Tuberculosis, Fungal, HIV.
- Tumors: Metastatic cancer.
- Hemorrhage: Sepsis, trauma (Waterhouse-Friderichsen).
- Drugs (Ketoconazole) or Genetic defects.
- Hormonal Profile: Low Cortisol, Low Aldosterone, Very High ACTH (lack of negative feedback).
Clinical Signs & Symptoms (Addison's)
- Fatigue and Weakness: Profound/chronic.
- Weight Loss & Anorexia.
- Hyperpigmentation: Hallmark sign due to very high ACTH (stimulates melanocytes). Skin darkening in sun-exposed areas, scars, gums.
- Hypotension: Low BP, orthostatic (lack of aldosterone/cortisol).
- Electrolyte Abnormalities: Hyponatremia (low Na+), Hyperkalemia (high K+).
- Salt Craving.
- Hypoglycemia.
Adrenal Crisis (Addisonian Crisis)
A life-threatening acute exacerbation often triggered by stress (infection, trauma, surgery). Characterized by severe hypotension, shock, vomiting, abdominal pain, profound weakness, and altered mental status. Requires immediate IV glucocorticoid replacement.
2. Secondary Adrenocortical Insufficiency
Deficiency of ACTH secretion from the pituitary gland, leading to insufficient stimulation of the adrenal cortex. The adrenal glands are typically healthy.
- Causes:
- Hypopituitarism: Tumors, radiation, Sheehan's syndrome.
- Suppression by Exogenous Steroids: Most common cause. Long-term steroid therapy suppresses HPA axis. Sudden stopping leads to insufficiency. Steroids must be tapered slowly.
- Hormonal Profile: Low Cortisol, Low ACTH. Aldosterone is usually normal (regulated by RAAS).
- Key Distinction from Primary: Absence of hyperpigmentation (due to low ACTH) and less severe electrolyte disturbances (preserved aldosterone).
Source: https://doctorsrevisionuganda.com | Whatsapp: 0726113908