BONY PELVIS
The bony pelvis is a rigid, basin-shaped ring of bones connecting the vertebral column to the lower limbs. It functions primarily to bear the weight of the upper body, protect pelvic viscera (internal organs), and provide attachment points for muscles of the trunk and lower extremities.
1. Osteology - Bone Structure of the Pelvis
Component Bones
The pelvic girdle is formed by the fusion of three major bones: the two hip bones laterally and anteriorly, and the sacrum posteriorly. The coccyx forms the terminal segment.
Two Hip Bones (Os Coxae)
Also called innominate bones. Each is formed by the fusion of three embryological components that meet at the acetabulum:
- Ilium: The superior and largest portion.
- Ischium: The posterior-inferior portion.
- Pubis: The anterior-inferior portion.
Sacrum
A large, triangular bone formed by the fusion of five sacral vertebrae (S1-S5), wedged firmly between the two hip bones to transmit body weight.
Coccyx
The terminal segment of the vertebral column, typically formed by 3-5 fused rudimentary vertebrae.
The three components of each hip bone (ilium, ischium, pubis) fuse at the acetabulum by puberty. The acetabulum is the deep socket that receives the head of the femur, forming the hip joint.
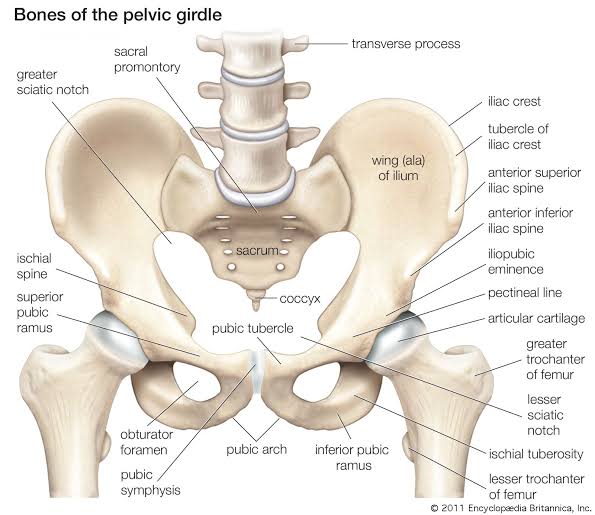
The Hip Bone (Os Coxae) - Detailed Landmarks
A. Ilium
The largest and most superior component of the hip bone. It forms the superior aspect of the acetabulum and extends superiorly to form the iliac fossa.
- Iliac crest: The superior curved border; serves as an attachment site for abdominal muscles and fascia.
- Anterior Superior Iliac Spine (ASIS): The anterior termination of the iliac crest; a palpable landmark and attachment for the inguinal ligament.
- Anterior Inferior Iliac Spine (AIIS): Located below the ASIS; origin of the rectus femoris muscle.
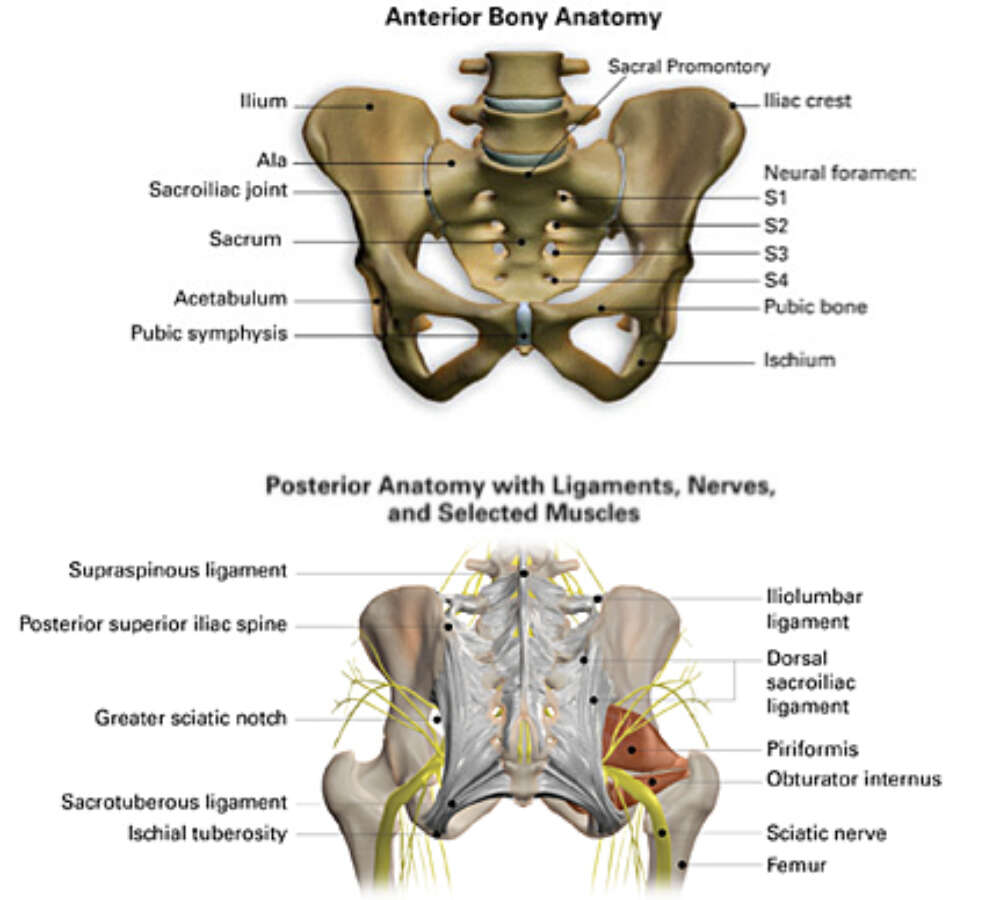
- Posterior Superior Iliac Spine (PSIS): Posterior termination of the iliac crest; attachment for posterior sacroiliac ligaments.
- Posterior Inferior Iliac Spine (PIIS): Located below the PSIS; forms the superior boundary of the greater sciatic notch.
- Greater sciatic notch: A large indentation on the posterior margin; converted into the greater sciatic foramen by pelvic ligaments.
- Iliac fossa: The large, smooth concavity on the internal surface; origin of the iliacus muscle.
B. Ischium
The posterior-inferior component of the hip bone, forming the posterior aspect of the acetabulum and the inferior body of the pelvis.
- Ischial spine: A pointed projection from the posterior margin; separates the greater and lesser sciatic notches.
- Lesser sciatic notch: Located below the ischial spine; converted to the lesser sciatic foramen by the sacrospinous and sacrotuberous ligaments.
- Ischial tuberosity: The rough, weight-bearing prominence; this is the primary point of contact when sitting (the "sitting bone").
- Ischial ramus: The anterior extension that fuses with the inferior pubic ramus to form the ischiopubic ramus.
C. Pubis
The anterior component of the hip bone, forming the anterior aspect of the acetabulum and the anterior body of the pelvis.
- Superior pubic ramus: Extends from the body of the pubis to the acetabulum; contains the pectineal line.
- Inferior pubic ramus: Extends from the pubic body to fuse with the ischial ramus.
- Pubic crest: The superior border of the pubic body; attachment for the rectus abdominis muscle.
- Pubic tubercle: A small prominence on the pubic crest; medial attachment point of the inguinal ligament.
- Pectineal line: A sharp ridge on the superior pubic ramus; forms part of the pelvic brim.
Major Openings & Landmarks
- Obturator Foramen: A large opening formed by the ischium and pubis, almost completely covered by the obturator membrane in life. The obturator nerve and vessels pass through a small gap called the obturator canal (superior part of the foramen).
- Acetabulum: The deep, cup-shaped socket on the lateral aspect of the hip bone.
- The ilium forms the superior roof.
- The ischium forms the posterior-inferior portion.
- The pubis forms the anterior portion.
- The acetabular fossa is the non-articular depression at the center.
- The lunate surface is the articular (cartilage-covered) crescent-shaped rim that contacts the femoral head.
Sacrum & Coccyx Details
| Structure | Description | Clinical Significance |
|---|---|---|
| Sacral Promontory | Anterior projection of the S1 vertebral body; the posterior boundary of the pelvic inlet. | Key landmark for measuring the obstetric conjugate. |
| Sacral Foramina | Anterior and posterior openings on the sacrum for the passage of sacral spinal nerves. | Site for sacral nerve block anesthesia. |
| Auricular Surface | The ear-shaped articular surface on the lateral aspect of the sacrum for the sacroiliac joint. | Subject to degenerative changes and lower back pain. |
| Coccyx | 3-5 fused rudimentary vertebrae; articulates with the apex of the sacrum. | Fractures can occur during childbirth or falls. |
2. Pelvic Divisions & Spaces
The pelvis is divided into functional spaces by the pelvic brim (pelvic inlet), creating the greater (false) pelvis above and the lesser (true) pelvis below. Understanding these divisions is critical for both anatomical study and clinical practice, especially in obstetrics.
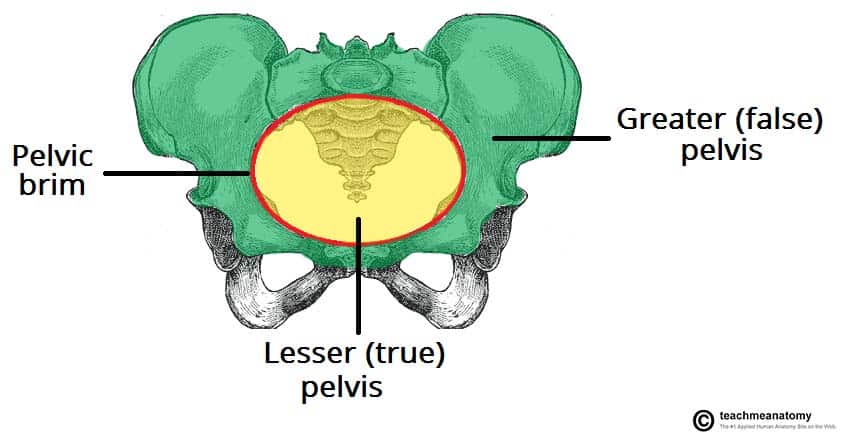
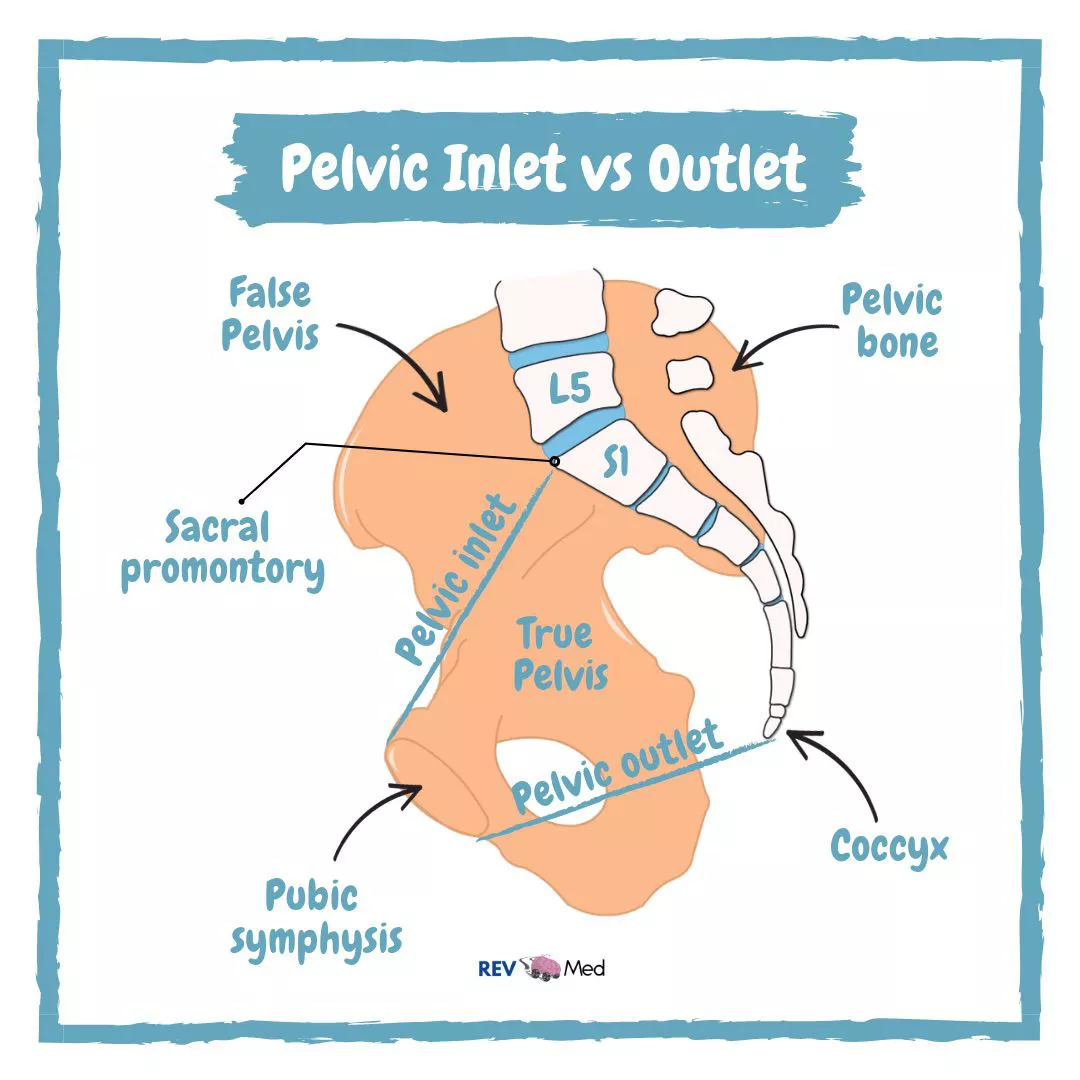
The Pelvic Inlet (Pelvic Brim)
The pelvic inlet is the superior opening of the true pelvis, bounded continuously by the following structures:
- Posterior: Sacral promontory and alae (wings) of the sacrum.
- Lateral: Arcuate line of the ilium.
- Anterolateral: Pectineal line of the pubis.
- Anterior: Pubic crest and superior border of the pubic symphysis.
The Pelvic Outlet
The pelvic outlet is the inferior opening of the true pelvis, bounded by:
- Anterior: Pubic arch (subpubic angle).
- Lateral: Ischial tuberosities.
- Posterolateral: Sacrotuberous ligaments.
- Posterior: Tip of the coccyx.
True vs. False Pelvis
- Bounded by the iliac fossae laterally.
- Located above the pelvic brim.
- Houses lower abdominal viscera (ileum, sigmoid colon).
- Technically part of the abdominal cavity, not the true pelvis.
- Has little obstetric significance.
- Situated between the pelvic inlet and outlet.
- Contains reproductive organs, urinary bladder, and rectum.
- Has the shape of a curved canal.
- Critical for childbirth (acts as the birth canal).
- Subject to detailed obstetric measurement (pelvimetry).
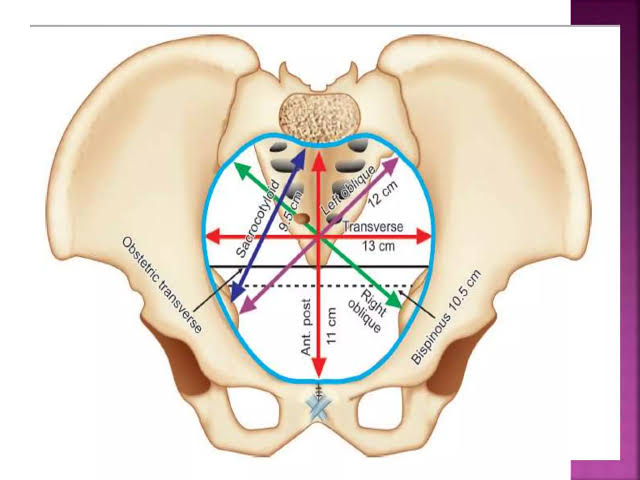
Pelvic Cavity - Dimensions & Axis
The Pelvic Axis is an imaginary curved line passing through the center of the pelvic cavity from the sacral promontory to the pubic symphysis. The fetal head must align with this axis during normal labor. The axis is not straight - it curves posteriorly at the inlet and anteriorly at the outlet.
| Parameter | Description | Typical Value |
|---|---|---|
| Pelvic Inclination | Angle between the plane of the pelvic inlet and the horizontal plane. | 55-60 degrees in standing posture. |
| Anteroposterior Diameter | Distance from sacral promontory to pubic symphysis. | ~11 cm (true conjugate). |
| Transverse Diameter | Widest distance between the lateral walls of the pelvic inlet. | ~13 cm. |
| Oblique Diameter | From sacroiliac joint to the opposite iliopubic eminence. | ~12 cm. |
3. Joints & Ligamentous Support
The stability of the pelvic ring depends on a combination of strong ligaments and specialized joints designed primarily for weight transfer rather than mobility. Understanding these structures is essential for comprehending pelvic fracture mechanics and stability.
A. Pubic Symphysis
Secondary Cartilaginous Joint (Amphiarthrosis): Unites the left and right pubic bones anteriorly via an interpubic fibrocartilage disc. It is a slightly movable joint that allows for limited movement during walking and, importantly, expansion during childbirth under hormonal influence. It is reinforced by superior and inferior pubic ligaments.
B. Sacroiliac (SI) Joints
The SI joints are among the strongest joints in the body, designed to transfer weight from the upper body to the lower limbs. They are synovial joints in their anterior portion but have extensive fibrous connections posteriorly.
- Type: Synovial (anterior) + Fibrous (posterior).
- Articular Surface: Auricular (ear-shaped) surfaces of the sacrum and ilium.
- Function: Weight transfer, minimal movement.
- Stability: Extremely stable due to interlocking surfaces and massive ligaments.
- Clinical: A common source of lower back pain (SI joint dysfunction).
C. Sacrococcygeal Joint
The articulation between the apex of the sacrum and the base of the coccyx. It is a symphysis type joint with an intervertebral disc that may undergo fusion with age. The coccyx is capable of limited backward movement during defecation and childbirth.
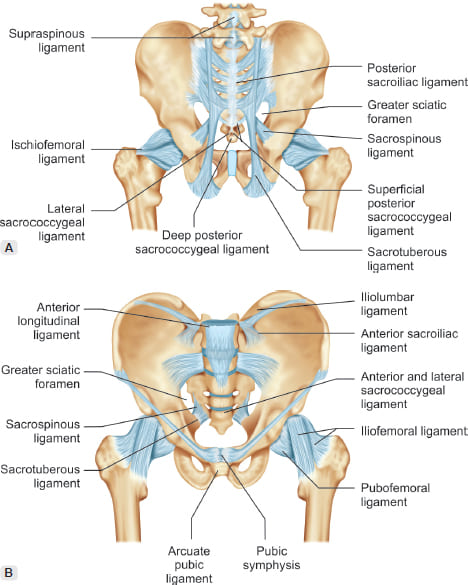
Key Pelvic Ligaments
- Sacroiliac Ligaments (Anterior, Posterior, Interosseous):
- The anterior ligaments are thin.
- The posterior sacroiliac ligaments are massive, multi-layered structures that are the primary stabilizers of the SI joint.
- The interosseous sacroiliac ligaments fill the space between the sacrum and ilium posteriorly, forming the strongest ligamentous structure in the body.
- Sacrotuberous Ligament: Extends from the posterior sacrum and posterior superior iliac spine to the ischial tuberosity. It is a broad, strong ligament that prevents upward tilting of the sacrum and converts the greater sciatic notch into the greater sciatic foramen.
- Sacrospinous Ligament: Extends from the lateral sacrum and coccyx to the ischial spine. It is thinner and more triangular. Together with the sacrotuberous ligament, it converts the lesser sciatic notch into the lesser sciatic foramen.
The sacrotuberous and sacrospinous ligaments are critical in converting the bony sciatic notches into functional foramina (passageways):
- Greater sciatic foramen: Located above the sacrospinous ligament; transmits the piriformis muscle, superior and inferior gluteal vessels, sciatic nerve, pudendal nerve, and internal pudendal vessels.
- Lesser sciatic foramen: Located below the sacrospinous ligament; transmits the tendon of obturator internus, pudendal nerve, and internal pudendal vessels (as they exit the pelvis to enter the perineum).
4. Pelvimetry & Sexual Dimorphism
The bony pelvis exhibits significant sexual dimorphism, with the female pelvis specifically adapted for childbirth. Pelvimetry is the measurement of pelvic dimensions, critical for assessing whether a vaginal delivery is feasible.
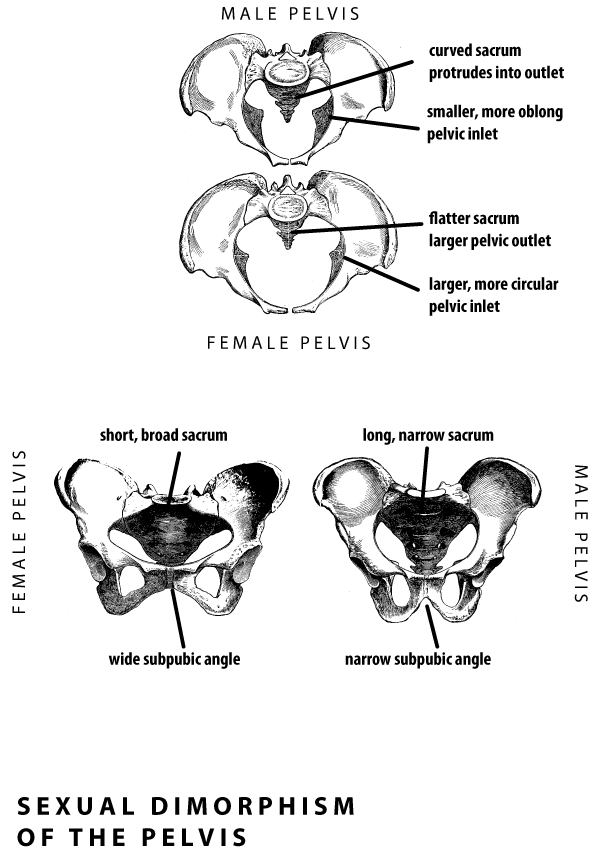
Anatomical Sex Differences
| Feature | Male Pelvis (Android) | Female Pelvis (Gynecoid) |
|---|---|---|
| General Architecture | Heavy, thick, narrow, and more massive. | Light, thin, wide, and more gracile. |
| Pelvic Inlet Shape | Heart-shaped. | Oval or rounded. |
| Subpubic Angle | Acute, less than 70 degrees. | Obtuse, greater than 80-90 degrees. |
| Ischial Spines | Inverted, closer together (prominent). | Everted, further apart (blunt). |
| Greater Sciatic Notch | Narrow, U-shaped. | Wide, almost 90 degrees. |
| Sacrum | Long, narrow, curved, projects more. | Short, wide, less curved. |
| Pelvic Outlet | Relatively small. | Relatively large. |
| Coccyx | Less movable, projects forward. | More movable, straighter. |
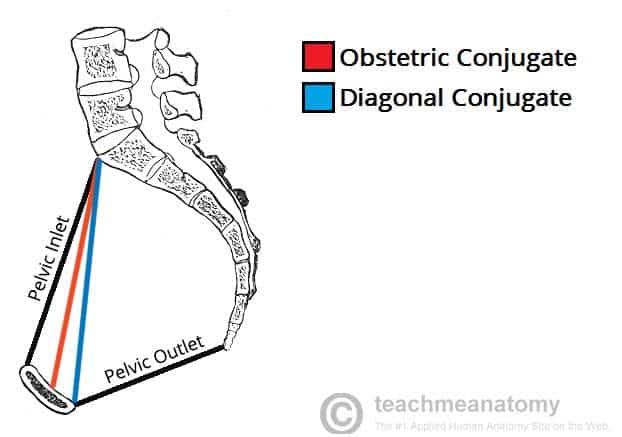
Obstetric Conjugates
These are anteroposterior (AP) measurements of the pelvic inlet.
- Anatomical (True) Conjugate: From the sacral promontory to the superior border of the pubic symphysis. This is the shortest AP diameter but cannot be measured clinically. (Normal: >= 11 cm).
- Obstetric Conjugate: The narrowest fixed distance over which the fetal head must pass. Measured from the sacral promontory to the posterior protrusion (most prominent point) of the pubic symphysis. This is the most critical measurement for assessing pelvic adequacy. (Normal: >= 10 cm).
- Diagonal Conjugate: The only conjugate that can be measured clinically via manual vaginal examination. It extends from the sacral promontory to the inferior border of the pubic symphysis. The obstetric conjugate is estimated by subtracting 1.5-2 cm from the diagonal conjugate. (Normal: >= 11.5 cm).
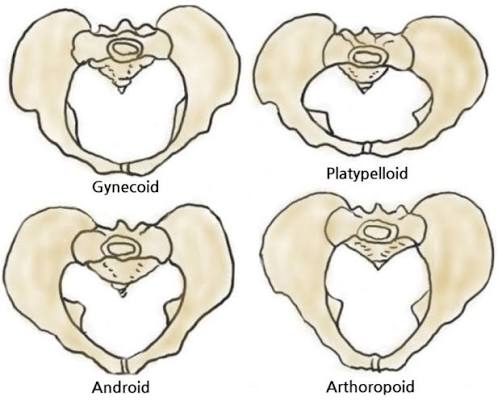
Caldwell-Moloy Classification
This system categorizes the female pelvis into four types based on the shape of the pelvic inlet:
- Round/oval inlet.
- Wide subpubic angle.
- Most favorable for labor (Normal labor progression expected).
- Incidence: ~50%.
- Heart-shaped inlet (male type).
- Narrow subpubic angle.
- Deep transverse arrest risk (Fetal head may engage in posterior position; higher risk of obstructed labor and cesarean).
- Incidence: ~33%.
- AP-elongated oval inlet.
- Long sacrum.
- Fetal head often engages in occiput posterior position; prolonged second stage possible.
- Transversely wide, flat inlet.
- Short AP diameter.
- Fetal head may not engage at all; elective cesarean often recommended.
- Incidence: ~3%.
5. Clinical & Applied Anatomy
Understanding pelvic anatomy is essential for managing trauma, performing diagnostic procedures, predicting obstetric outcomes, and recognizing hormonally mediated changes during pregnancy.
Fracture Mechanics - The Pelvic Ring
The pelvis functions as a structural ring. A break in one location of the ring is almost always accompanied by a break (or dislocation) in another location. This principle guides both diagnosis and treatment.

Case Study: Open-Book Fracture
A 28-year-old male motorcyclist involved in a high-speed collision presents with severe pelvic pain and hemodynamic instability (BP: 85/50 mmHg, HR: 128 bpm). Mechanism: Anterior-Posterior (AP) Compression.
Pathophysiology: The "open-book" fracture results from AP compression forces. The pubic symphysis disrupts anteriorly, and the sacroiliac joints disrupt posteriorly, causing the hemipelvis to rotate externally like an opening book. This dramatically increases pelvic volume, allowing massive hemorrhage into the retroperitoneal space from the internal iliac vascular network.
| Fracture Type | Mechanism | Key Risk |
|---|---|---|
| Open-Book (APC) | Anterior-posterior compression. | Massive hemorrhage from internal iliac vessels; hemodynamic instability. |
| Lateral Compression (LC) | Lateral impact (e.g., T-bone motor vehicle collision). | Internal rotation of hemipelvis; severe bladder or urethral injury. |
| Vertical Shear (VS) | Fall from height; axial loading. | Most unstable; severe neurovascular injury. |
| Combined | Complex multi-directional forces. | Highest mortality; combination of all risks. |
Bone Marrow Aspiration
The posterior iliac crest is the preferred site for bone marrow biopsy and aspiration because:
- It is easily accessible and palpable.
- It contains abundant hematopoietic (red) marrow in adults.
- The risk of damaging major vessels or nerves is minimal.
- The bone is relatively superficial (covered only by skin, subcutaneous tissue, and gluteal muscles).
Procedure Note: The needle is inserted 2-3 cm posterior to the posterior superior iliac spine (PSIS) and advanced through the cortical bone into the marrow cavity.
Obstetric Complications: Obstructed Labor (Dystocia)
Pelvic outlet narrowing or contraction of the interspinous diameter can lead to cephalopelvic disproportion (CPD) - a mismatch between fetal head size and pelvic dimensions.
- Inlet contraction: Short obstetric conjugate (< 10 cm) leads to failure of fetal head engagement.
- Mid-pelvic contraction: Narrow interspinous diameter (< 10 cm) leads to deep transverse arrest.
- Outlet contraction: Narrow subpubic angle leads to difficulty with fetal head extension and delivery.
Hormonal Modifications During Pregnancy
A peptide hormone produced by the corpus luteum and later by the placenta. Its primary role in pregnancy is to increase the laxity of pelvic ligaments and the pubic symphysis, allowing temporary expansion of pelvic dimensions for parturition (birth).
- Anatomical Target: Sacroiliac ligaments, sacrotuberous ligaments, pubic symphysis interpubic disc.
- Functional Outcome: Greater SI joint mobility; increased pelvic outlet diameter. Symphyseal widening causes increased AP diameter of the outlet (up to 4-9 mm separation).
- Other Effects: Cervical ripening (softening/dilation) and inhibition of uterine contractions (prevents premature labor).
Excessive relaxin-mediated symphyseal separation (> 10 mm) can cause symphysis pubis dysfunction (SPD) or diastasis symphysis pubis. This condition is characterized by severe pelvic girdle pain, difficulty walking, and joint instability. Management includes pelvic binders, physical therapy, and in severe cases, surgical fixation.