The Reticular Formation: Master Control Center
A comprehensive guide detailing the core anatomy, ascending and descending pathways, vital centers, neurotransmitter factories, and advanced clinical concepts of the Reticular Formation (RF).
Section I: Core Anatomy and Location
What is the Reticular Formation?
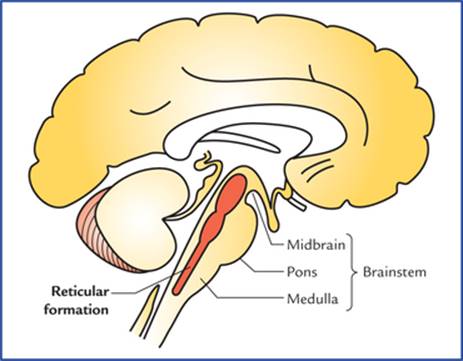
The Reticular Formation (RF) is a diffuse, net-like network of nerve cells (neurons) scattered throughout the core of the brainstem. The name comes from the Latin word "reticulum" meaning "little net", perfectly describing its web-like appearance.
- It is NOT a discrete, well-defined nucleus like the cranial nerve nuclei.
- It is a polysynaptic network — signals pass through many neuron-to-neuron connections.
- It contains a mixture of small and large neurons with diverse functions.
- It receives collateral branches from virtually ALL ascending sensory pathways.
Where is it Located?
The Reticular Formation spans the entire length of the brainstem, occupying the central core (tegmentum). It surrounds the central canal and fourth ventricle, flanked medially by the raphe nuclei and laterally by sensory and motor pathways.
| Region | Location Within Brainstem |
|---|---|
| Medulla | Lower (caudal) portion of RF |
| Pons | Middle portion of RF |
| Midbrain | Upper (rostral) portion of RF |
Anatomical Boundaries
- Dorsally: Fourth ventricle (in pons/medulla) and cerebral aqueduct (in midbrain).
- Ventrally: Pyramidal tracts and corticospinal fibers.
- Laterally: Sensory nuclei and ascending tracts.
Memory Tip: The RF is like the "internet backbone" of the brainstem — everything connects through it!
The Three Zones of the Reticular Formation
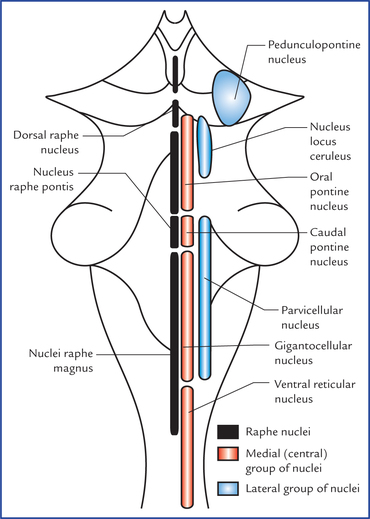
The Reticular Formation is organized into three vertical columns running from inside to outside (Median, Medial, and Lateral).
- Position: Exactly at the midline.
- Neurons: Small to medium-sized.
- Key Structure: Raphe Nuclei — the serotonin-producing factories.
- Function: Sleep regulation, mood control, pain modulation.
- Position: Inner column, just lateral to the median zone.
- Neurons: Large multipolar neurons (magnocellular = large-celled).
- Function: Major projection neurons sending long axons to the Thalamus (ascending), Spinal cord (descending), and Cerebellum.
- Role: The "output" zone of the RF.
- Position: Outer column, most lateral part of RF.
- Neurons: Small neurons (parvicellular = small-celled).
- Function: Receives collateral inputs from all sensory pathways. Acts as interneurons and relay stations.
- Role: The "input" zone of the RF.
Memory Tip Think "In-Large-Out-Small" — the Inner zone has Large cells that send outputs; the Lateral zone has Small cells that receive inputs.
Section II: Ascending Pathways
The Ascending Reticular Activating System (ARAS)
The ARAS is the portion of the RF that sends signals upward to the thalamus and cerebral cortex. It acts as the brain's "alarm clock," responsible for maintaining wakefulness and alertness.
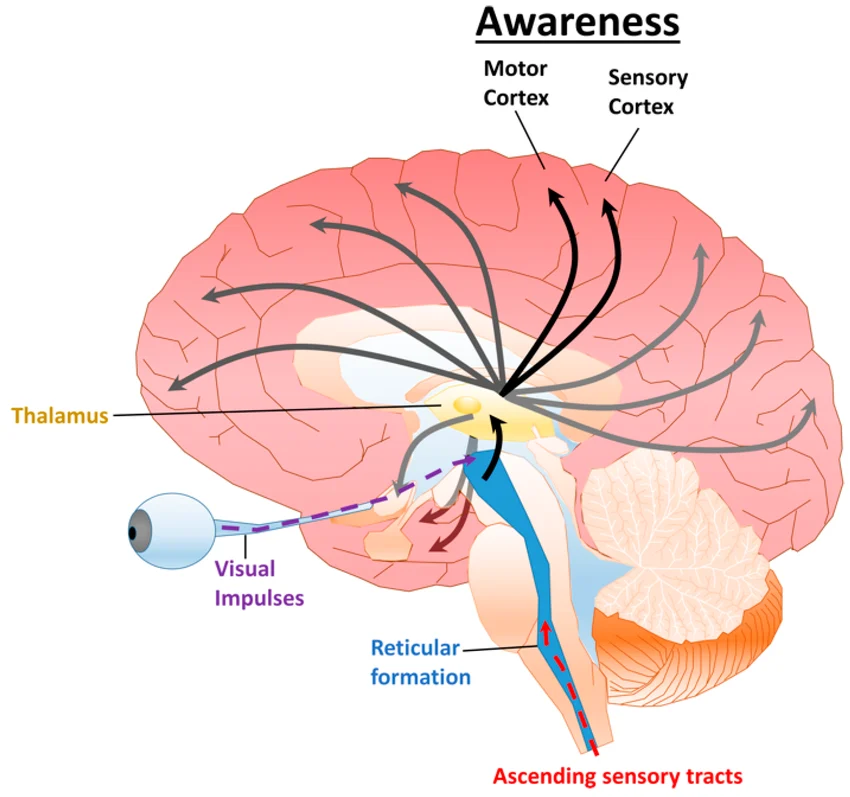
How It Works (The Pathway)
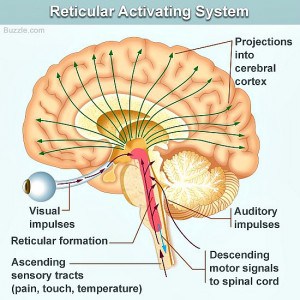
- Sensory inputs from all modalities (touch, pain, hearing, vision) send collateral branches to the RF.
- The lateral zone of RF receives these signals.
- Medial zone neurons relay signals upward.
- Signals pass through the thalamus (specifically intralaminar nuclei).
- Diffuse projections spread across the entire cerebral cortex.
- Result: Cortical activation and conscious awareness.
The Sleep-Wake Cycle & ARAS States
| ARAS State | Effect on Body |
|---|---|
| ARAS "ON" | Awake, alert, conscious |
| ARAS "DIM" | Drowsy, relaxed |
| ARAS "OFF" | Deep sleep (NREM) |
| ARAS DAMAGED | Coma, loss of consciousness |
The ARAS does NOT carry specific sensory information (like "this is pain" or "this is red"). Instead, it provides non-specific activation that keeps the cortex "awake" enough to process specific incoming information from other pathways.
Neurotransmitters of the ARAS
| Neurotransmitter | Source | Role |
|---|---|---|
| Acetylcholine | PPN, Basal Forebrain | Cortical activation |
| Norepinephrine | Locus Coeruleus | Arousal, vigilance |
| Serotonin | Raphe Nuclei | Mood, wakefulness |
| Histamine | Tuberomammillary Nucleus | Wake promotion |
| Orexin/Hypocretin | Lateral Hypothalamus | Stabilizes wakefulness |
Clinical Correlation: RAS Damage & Coma
Why does injury to the Reticular Formation cause a loss of consciousness?
- Normal Function: The cortex receives continuous activating signals from the ARAS. This maintains a tonic level of excitation. Even without specific sensory input, the brain remains "online".
- After RAS Damage: The cortex receives NO activating signals. Cortical neurons fall silent, and consciousness is immediately lost.
The ARAS is bilateral. Damage to BOTH sides is required to cause a coma. Unilateral damage causes hemi-inattention or neglect, but NOT loss of consciousness. The thalamus is also critical — thalamic injury can mimic RAS coma.
Common Causes of RAS Damage
| Cause | Mechanism |
|---|---|
| Traumatic Brain Injury | Direct impact, shearing forces on brainstem |
| Brainstem Stroke | Ischemia in pontine or midbrain arteries |
| Increased Intracranial Pressure | Herniation (tonsillar, central) compressing brainstem |
| Toxic/Metabolic | Drug overdose, hypoglycemia, hypoxia |
| Infection | Encephalitis, meningitis involving brainstem |
Any patient with altered consciousness + brainstem signs (abnormal pupils, abnormal respiratory pattern, decerebrate posturing) should have immediate brain imaging to rule out brainstem compression or stroke.
Section III: Descending Pathways (Reticulospinal Tracts)
The RF sends two major motor pathways down to the spinal cord for Motor Control of Posture & Muscle Tone.
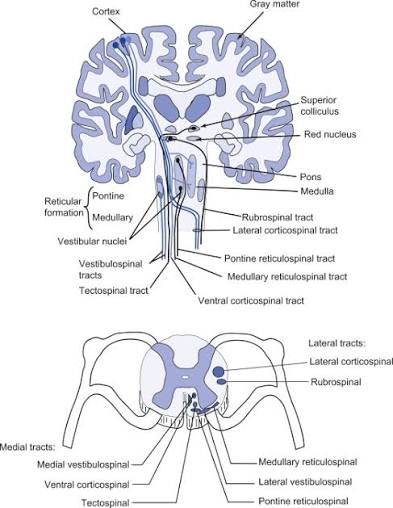
- Origin: Pontine reticular formation (nucleus reticularis pontis caudalis & oralis).
- Path: Anterior funiculus of spinal cord.
- Termination: Anterior horn cells (motor neurons).
- Neurotransmitter: Glutamate (excitatory).
- Function: EXCITES extensor (anti-gravity) muscles.
- Effect: Increases muscle tone, maintains posture.
- Origin: Medullary reticular formation (nucleus reticularis gigantocellularis).
- Path: Lateral funiculus of spinal cord.
- Termination: Anterior horn cells.
- Neurotransmitter: Glycine, GABA (inhibitory).
- Function: INHIBITS extensor muscles.
- Effect: Decreases muscle tone, allows movement (relaxes posture).
The Push-Pull Balance
These two tracts work as an antagonistic pair:
Pontine Tract (+) ↔ Medullary Tract (-)
(Excite) (Inhibit)
Extensor Muscles Extensor Muscles
Normal state: Both are active, creating balanced muscle tone.
Memory Tip Pontine = Posture + Power = Positive (excitatory). Medullary = Mellow = Minus (inhibitory).
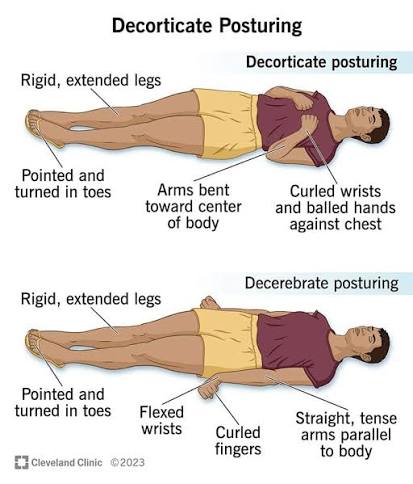
Decerebrate Posturing
Decerebrate posturing is a sign of severe brainstem injury below the level of the midbrain. It represents the uncontrolled, overactive firing of the pontine reticulospinal tract when freed from higher cortical inhibition.
The Mechanism (Step by Step)
- Damage Below the Midbrain: Lesion between the midbrain and pons, or lower. Causes: severe TBI, brainstem stroke, or herniation.
- Loss of Cortical Input: The cerebral cortex normally sends inhibitory fibers to the pontine RF. These fibers are severed. The pontine tract is no longer inhibited.
- Pontine Tract Over-Activity: Without inhibition, the pontine reticulospinal tract fires excessively. It over-excites extensor motor neurons in the spinal cord.
- Clinical Appearance:
- Arms: Stiffly extended, adducted, internally rotated, pronated.
- Wrists: Flexed.
- Legs: Stiffly extended.
- Feet: Plantar flexed.
- Jaw: Clenched.
- Prognosis: Sign of SEVERE brainstem dysfunction. Generally indicates poor prognosis.
Decerebrate vs. Decorticate Posturing
| Feature | Decorticate | Decerebrate |
|---|---|---|
| Lesion Level | Above midbrain (cortex, internal capsule) | Below midbrain (pons, upper medulla) |
| Arm Position | Flexed (bent inward) | Extended (stiff straight out) |
| Leg Position | Extended | Extended |
| Which tract affected | Corticospinal damage | Ponticospinal unopposed |
Section IV: Autonomic Vital Centers
The lower brainstem (medulla oblongata) acts as your body's life support system, containing automatic survival centers that control essential life functions.
1. Cardiovascular Center
Located in the dorsal medulla (near the floor of the fourth ventricle). It has three sub-components:
- Cardioacceleratory Center: Sympathetic output. Increases heart rate via cardiac accelerator nerves. Releases norepinephrine.
- Cardioinhibitory Center: Parasympathetic output (vagus nerve). Decreases heart rate. Releases acetylcholine.
- Vasomotor Center: Controls blood vessel diameter. Causes vasoconstriction (sympathetic) and vasodilation (parasympathetic in some vessels).
Sensory Inputs: Baroreceptors in carotid sinus/aortic arch (detect BP) and Chemoreceptors in carotid/aortic bodies (detect O2, CO2, pH).
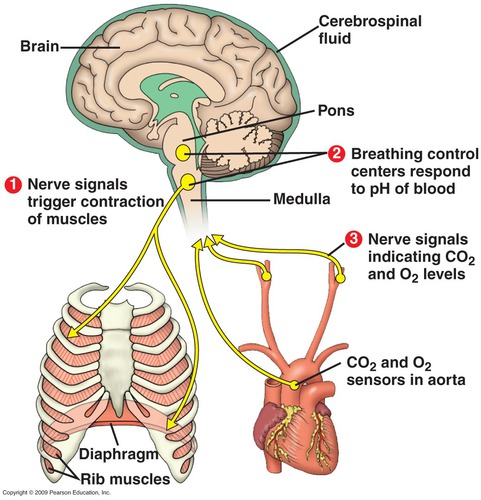
2. Respiratory Center
Located in the ventrolateral medulla. It has three sub-components:
- Dorsal Respiratory Group (DRG): Primary inspiration control. Contains inspiratory neurons. Receives input from the vagus nerve (lung stretch receptors).
- Ventral Respiratory Group (VRG): Active during forced expiration. Contains both inspiratory and expiratory neurons.
- Pneumotaxic Center (in pons): Limits inspiration duration and prevents over-inflation of lungs.
Sensory Inputs: Central chemoreceptors (medulla — detect CSF pH/CO2), Peripheral chemoreceptors (carotid/aortic bodies), and Lung stretch receptors (vagus nerve).
Why Medullary Damage is Fatal
The medulla controls the most primitive, essential functions (Heartbeat, Breathing rhythm, Blood pressure, Vomiting/coughing/swallowing reflexes). Even small lesions in the medulla can cause sudden cardiac arrest, respiratory failure, or death.
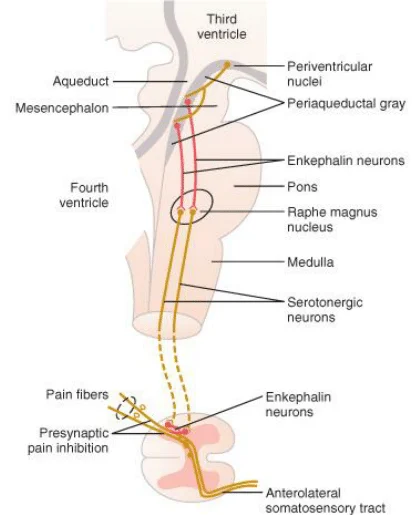
Section V: Pain Modulation
The Descending Analgesic Pathway (The "Pain Brake")
The Reticular Formation plays a crucial role in modulating pain signals. It can literally "turn down the volume" on pain perception.

The Pathway
Ascending (Pain Detection):
- Nociceptors in periphery detect tissue damage.
- Pain signals travel via the spinothalamic tract to the spinal cord.
- Collaterals branch to the Reticular Formation.
- RF alerts the brain: "Something is wrong!"
Descending (Pain Inhibition):
- Higher centers (cortex, hypothalamus, amygdala) evaluate the pain.
- Signals descend to the Periaqueductal Gray (PAG) in the midbrain.
- PAG activates Raphe Nuclei and other RF nuclei.
- RF sends descending inhibitory fibers to the spinal cord.
- These fibers block pain transmission at the dorsal horn.
Natural Painkiller Chemicals
| Chemical | Source | Mechanism |
|---|---|---|
| Endorphins | Pituitary, hypothalamus, PAG | Bind to opioid receptors, block pain |
| Serotonin | Raphe nuclei | Inhibits dorsal horn pain neurons |
| Enkephalins | Interneurons in spinal cord | Endogenous opioids, short-acting |
| GABA | Various inhibitory interneurons | General inhibition |
| Noradrenaline | Locus coeruleus | Inhibits pain transmission |
Gate Control Theory
The RF acts as a "gate" at the spinal cord level. If the gate is OPEN, pain signals pass freely and pain is felt. If the gate is CLOSED, pain signals are blocked, and pain is reduced or absent.
Factors that CLOSE the gate:
- Distraction, attention elsewhere
- Stress or danger (battlefield analgesia)
- Placebo effect
- Acupuncture
- Strong emotions
Section VI: Neurotransmitter Factories
The Reticular Formation contains specialized nuclei that produce specific chemical messengers that control mind and body.
Memory Tip Serotonin = GOLD, Norepinephrine = BLUE, Dopamine = RED, Acetylcholine = GREEN.
1. Raphe Nuclei (Serotonin Production)
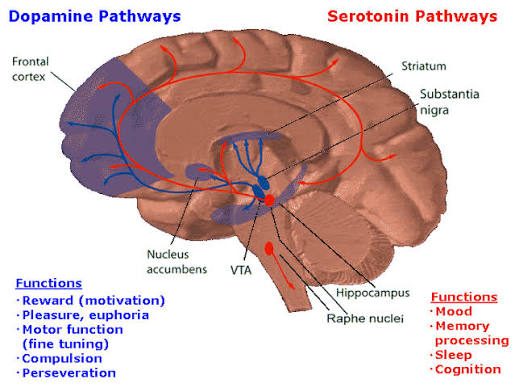
- Location: Median zone, forming a continuous column from the caudal medulla to the rostral midbrain.
- Key Nuclei: Dorsal raphe, median raphe, raphe magnus, raphe pallidus, raphe obscurus.
- Functions: Mood, sleep, pain inhibition, appetite, thermoregulation.
Synthesis Pathway:
Tryptophan (dietary amino acid) → Tryptophan hydroxylase → 5-HTP → Aromatic L-amino acid decarboxylase → SEROTONIN (5-HT)
Clinical Relevance:
- Depression: Low serotonin → SSRIs (Prozac, Zoloft) block reuptake.
- Migraine: Serotonin fluctuations trigger attacks → triptans activate 5-HT1B/D.
- Anxiety & Sleep Disorders: Serotonin imbalance.
2. Locus Coeruleus (Norepinephrine Center)
- Location: Dorsal pons, floor of fourth ventricle.
- Anatomy: "Blue Place" (contains neuromelanin giving a blue hue). Small nucleus (about 50,000 neurons) but projects everywhere.
- Functions: Panic, focus, stress response (fight-or-flight), arousal, vigilance. Silent during REM sleep.
Synthesis Pathway:
Tyrosine → Tyrosine hydroxylase → L-DOPA → DOPA decarboxylase → Dopamine → Dopamine beta-hydroxylase → NOREPINEPHRINE (NE)
Clinical Relevance:
- ADHD: Underactive LC → treated with stimulants.
- Anxiety/PTSD: Overactive/dysregulated LC → treated with beta-blockers, SNRIs.
- Alzheimer's: LC degenerates early → cognitive decline.
3. Ventral Tegmental Area (VTA - Dopamine Reward Center)
- Location: Midbrain, ventral to substantia nigra.
- Functions: Reward, motivation, pleasure, addiction, movement initiation.
- Major Pathways:
- Mesolimbic Pathway: VTA → Nucleus accumbens → Amygdala → Hippocampus. (The Reward Circuit).
- Mesocortical Pathway: VTA → Prefrontal cortex (Executive function).
Clinical Relevance:
- Addiction: Drugs of abuse HIJACK the mesolimbic pathway causing massive dopamine release.
- Schizophrenia: Mesolimbic overactivity (positive symptoms), Mesocortical underactivity (negative symptoms).
- Parkinson's: Associated substantia nigra degeneration.
4. Pedunculopontine Nuclei (PPN - Acetylcholine Center)
- Location: Pons-midbrain junction.
- Composition: ~90% Cholinergic (ACh), ~10% Glutamatergic.
- Functions:
- Movement Control: Activates spinal central pattern generators (works with basal ganglia).
- Sleep-Wake: CRITICAL for REM sleep generation (activates thalamus while LC and Raphe are silent).
- Attention & Learning: Sensory processing.
Clinical Relevance:
- REM Sleep Behavior Disorder (RBD): PPN dysfunction causes loss of REM atonia (violent dream enactment). Precedes Parkinson's by 10-15 years.
- Parkinson's Disease: PPN degeneration contributes to gait freezing and postural instability.
- Narcolepsy: Dysregulated REM mechanisms.
Section VII: Advanced Topics
1. Sleep-Wake Cycle Regulation
The Reticular Formation contains the master control system for sleep and wakefulness using a mutually inhibitory "Flip-Flop" Switch.
WAKE SYSTEM ↔ SLEEP SYSTEM
(LC, Raphe, PPN, Histamine, Orexin) ↔ (VLPO, MCH)
- Wakefulness System (ARAS "ON"): Norepinephrine (LC), Serotonin (Raphe), ACh (PPN), Histamine, Orexin (Stabilizer).
- Sleep System (ARAS "OFF"): Ventrolateral preoptic nucleus (VLPO) uses GABA to inhibit arousal systems. MCH promotes sleep.
2. RF & Cranial Nerves (Reflexes)
| Reflex / Function | Associated RF Structure |
|---|---|
| Horizontal Gaze | Paramedian pontine reticular formation (PPRF) |
| Vertical Gaze | Rostral interstitial nucleus of MLF (riMLF) |
| Torsional Eye Movements | Interstitial nucleus of Cajal |
| Vestibular Reflexes (VOR) | Vestibular nuclei (CN VIII) + RF |
| Vomiting / Coughing / Sneezing / Gagging | Medullary RF coordinates with various cranial nerves (IX, X) |
Clinical Pearl PPRF lesion causes inability to move eyes horizontally toward the lesion side (Internuclear ophthalmoplegia / INO when combined with MLF damage).
3. RF & Cerebellum (Motor Coordination)
The RF and Cerebellum create a feedback loop for real-time motor error correction and postural stability.
- Reticulocerebellar Tract: From Medullary/Pontine RF to Cerebellum (proprioception).
- Cerebelloreticular Tract: From Cerebellar nuclei back to RF (motor feedback).
4. Clinical Examination of the RF
- Level of Consciousness: Glasgow Coma Scale (GCS).
- Pupillary Responses: Intact pupils in coma suggest a metabolic cause; fixed dilated pupils suggest midbrain damage.
- Oculocephalic Reflex (Doll's Eyes): Intact RF = eyes move opposite direction of head turn.
- Oculovestibular Reflex: Caloric testing (Cold water = eyes deviate toward).
- Respiratory Patterns: Cheyne-Stokes (cortical dysfunction, RF intact), Central neurogenic hyperventilation (RF partially damaged), Ataxic breathing (Medullary damage - Ominous).
- Motor Response: Decorticate (flexion) vs Decerebrate (extension).
5. Brain Death & The Reticular Formation
Brain death requires the permanent cessation of all brainstem function, including the RF. If the entire brainstem is dead, no recovery is possible.
| Criteria Test | Requirement |
|---|---|
| Coma | No response to painful stimuli |
| Absent brainstem reflexes | Pupils, corneal, oculocephalic, gag, cough reflexes absent |
| Apnea test | No breathing when CO2 rises (PCO2 > 60 mmHg) |
Clinical Pearl Brain death is NOT the same as a vegetative state. In a vegetative state, the RF may be partially functional (sleep-wake cycles present), but the cortex is damaged.
6. Comparative Anatomy & Development
- Evolution: Highly conserved. The medullary RF (vital functions) is the oldest part. The pontine/midbrain RF evolved with consciousness in higher mammals.
- Development: ARAS matures in childhood. Newborns spend 50% of sleep in REM (PPN highly active) because it promotes rapid synaptic plasticity and brain development.
- Aging: By age 80, there is ~30% LC neuron loss (reduced alertness), Raphe loss (sleep fragmentation), and PPN loss (gait problems).
7. Imaging the RF
The RF is diffuse and blends with tissue, making it difficult to visualize on standard CTs. Specialized techniques include:
- MRI (T2/FLAIR) & DWI: Detects lesions, pontine infarcts (Locked-in syndrome), or demyelination.
- fMRI / PET / SPECT: Used to visualize functional activation and metabolic/receptor activity.
Clinical Pearl In Locked-in syndrome, the RF is INTACT but the corticospinal/corticobulbar tracts are destroyed. The patient is fully conscious but paralyzed (except for eye blinks).
8. Pharmacology of the RF
| Drug Class | Mechanism & Effect on RF |
|---|---|
| Benzodiazepines / Barbiturates | Enhance GABA-A → Inhibit ARAS (sedation / anesthesia). |
| Propofol / Ketamine | GABA agonist / NMDA blocker → Rapid / Dissociative anesthesia. |
| Amphetamines / Methylphenidate | Increase NE/DA release / block reuptake → Activate ARAS (wakefulness). |
| SSRIs / SNRIs / TCAs / MAOIs | Block monoamine reuptake or breakdown → Target Raphe and LC. |
9. Consciousness, Learning, and Electrophysiology
- Consciousness Theories: The RF supports Integrated Information Theory (providing tonic activation) and the Global Workspace Theory (acting as the "spotlight" providing the arousal component, while the cortex provides the content).
- Memory: Emotional arousal (LC NE release) strengthens memory encoding. Sleep (REM and Slow-Wave) is crucial for memory replay and consolidation.
Memory Tip: Study before sleep! But don't cram under extreme stress — too much LC activation impairs memory. - Electrophysiology (EEG Correlates):
- Beta (13-30 Hz): Active ARAS (Alert).
- Alpha (8-12 Hz): Reduced ARAS (Relaxed).
- Theta (4-8 Hz): Drowsy ARAS.
- Delta (0.5-4 Hz): Minimal ARAS (Deep sleep).
- Gamma (30-100 Hz): Coordinated ARAS+cortex (Conscious perception / binding).
10. Surgical Considerations
- Anesthesia: The goal is to suppress the ARAS just enough for surgery, but not so much that the medullary vital centers are compromised.
- Brainstem Surgery: Extremely high risk. Requires continuous monitoring of cranial nerves, vitals, and intraoperative neurophysiology (MEPs, SSEPs).
- Deep Brain Stimulation (DBS): Experimental targeting of PPN (for Parkinson's gait), LC (cognitive disorders), and Raphe (depression).
Summary & Key Takeaways
| Function | Structure/Pathway | Key Point |
|---|---|---|
| Consciousness | ARAS | Damage → coma |
| Posture/Movement | Reticulospinal tracts | Pontine (+), Medullary (-) |
| Vital Functions | Medullary centers | Heart, breathing, BP |
| Pain Control | Descending analgesic pathway | Natural opioids, serotonin |
| Mood | Raphe nuclei | Serotonin |
| Alertness | Locus Coeruleus | Norepinephrine |
| Reward | VTA | Dopamine |
| Sleep/REM | PPN | Acetylcholine |
"The RF is the BRAINSTEM'S BRAIN —
It wakes you up, keeps you upright,
Controls your heart and lungs,
Numbs your pain,
And brews the chemicals that make you feel."