Neuroanatomy: Pathways and Systems
Major Ascending & Descending Tracts of the Central Nervous System (CNS)
By the end of this exhaustive study guide, you will master:
- The Foundational Rules governing sensory (ascending) and motor (descending) pathways.
- The detailed, step-by-step neuronal chains of the Dorsal Column-Medial Lemniscus (DCML), Spinothalamic, and Spinocerebellar tracts.
- The precise routing of the Corticospinal (Pyramidal) tract from the motor cortex to the neuromuscular junction.
- The roles of extrapyramidal pathways, specifically the Rubrospinal, Vestibulospinal, and Reticulospinal tracts.
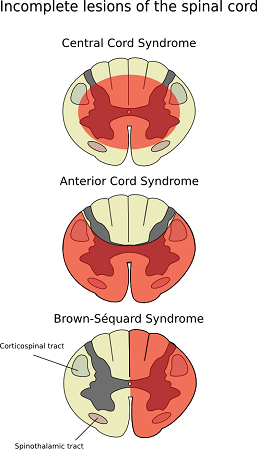
- How to confidently localize lesions using classic clinical syndromes like Brown-Séquard Syndrome, Anterior Cord Syndrome, and Syringomyelia.
- The critical decussation (crossing) points of every major tract to instantly predict ipsilateral versus contralateral deficits.
1. Core Principles of Neuroanatomy
Before memorizing the individual routes of specific tracts, you absolutely must master these four foundational rules. They will allow you to logically predict clinical deficits from any lesion location without blind memorization.
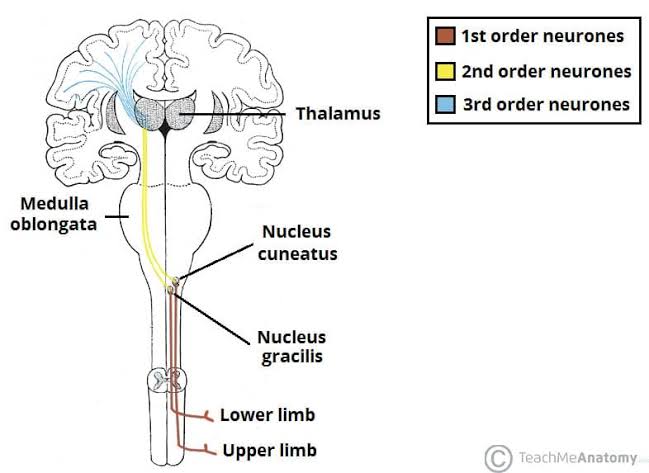
SENSORY = 3 NEURONS
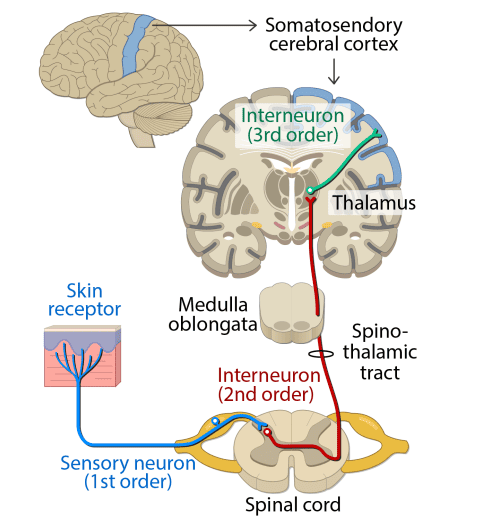
Information from the outside body reaches the conscious brain through a strict chain of three neurons:
- 1st Order Neuron: From the peripheral receptor to the spinal cord or brainstem.
- 2nd Order Neuron: From the spinal cord/brainstem up to the thalamus.
- 3rd Order Neuron: From the thalamus up to the cerebral cortex.
MOTOR = 2 NEURONS
Commands traveling from the brain down to the muscles run through a simple chain of two neurons:
- Upper Motor Neuron (UMN): Cell body resides in the motor cortex and descends into the spinal cord.
- Lower Motor Neuron (LMN): Cell body sits in the anterior horn of the spinal cord and projects out to the muscle.
DECUSSATION (CROSSING)
Most neural pathways cross over (decussate) to the opposite side of the body at some specific point. You MUST know exactly where each tract crosses. This single piece of information determines whether a patient's symptoms will appear on the left or the right side following a stroke or spinal injury.
IPSILATERAL vs. CONTRALATERAL
This is the ultimate secret to clinical neurology:
- If a lesion occurs BEFORE the pathway decussates, the deficits appear on the SAME side (ipsilateral).
- If a lesion occurs AFTER the pathway has already decussated, the deficits appear on the OPPOSITE side (contralateral).
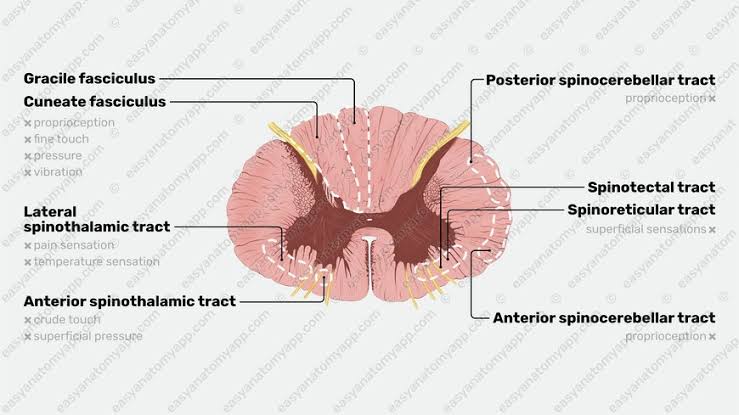
2. Spinal Cord Cross-Section Overview
The spinal cord is highly organized into outer white matter tracts (axons) surrounding an inner, butterfly-shaped core of central gray matter (cell bodies). Understanding this spatial arrangement is essential for visualizing how injuries destroy specific pathways.
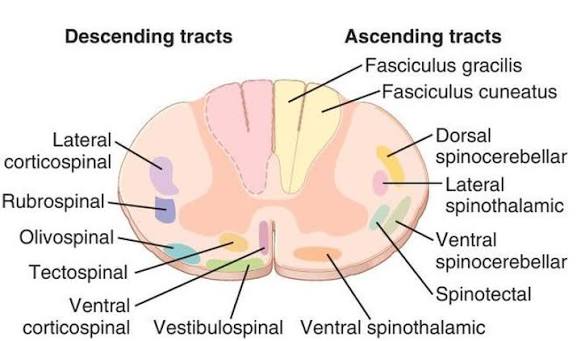
White Matter Organization (from outside inward):
The white matter is divided into columns called funiculi.
- Posterior (Dorsal) Funiculus: Contains the Fasciculus gracilis (medial) and Fasciculus cuneatus (lateral). This is the DCML sensory pathway.
- Lateral Funiculus: Contains the Lateral corticospinal tract (motor), Lateral spinothalamic tract (pain/temperature), and the Spinocerebellar tracts (unconscious proprioception).
- Anterior Funiculus: Contains the Anterior corticospinal tract (motor), Anterior spinothalamic tract (crude touch), and the Vestibulospinal/Reticulospinal tracts.
Gray Matter Organization:
- Dorsal Horn: Dedicated to sensory input. Contains the substantia gelatinosa, a critical site for pain modulation.
- Ventral Horn: Dedicated to motor output. Houses the Lower Motor Neurons (LMNs).
- Intermediate Zone: Contains Clarke's nucleus (specifically between levels T1-L2), which is the origin point for the spinocerebellar tracts.
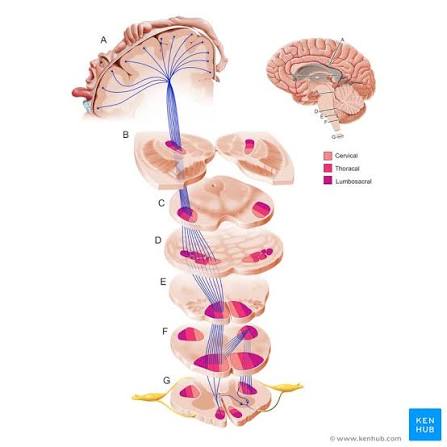
Somatotopic Arrangement (The Body Map)
In all tracts, the nerve fibers are highly organized according to the body region they supply (somatotopy):
- For the Corticospinal tract: Cervical (arm) fibers are located most medially, while lumbosacral (leg) fibers are most lateral.
- For the DCML: Sacral (leg) fibers are added most medially (gracilis), while cervical (arm) fibers are added most laterally (cuneatus).
3. Ascending (Sensory) Tracts
Sensory information travels from peripheral receptors to the cerebral cortex through the mandatory three-neuron chains. Each unique pathway carries specific sensory modalities and decussates at a highly characteristic anatomical location.
A. Dorsal Column-Medial Lemniscus (DCML) Pathway
Modalities Carried: Fine touch, vibration, conscious proprioception (knowing exactly where your limbs are in space with your eyes closed), and deep pressure.
This is the pathway for discriminative sensation — the refined ability to tell exactly where you were touched, how hard you were touched, and what the texture of the object is.
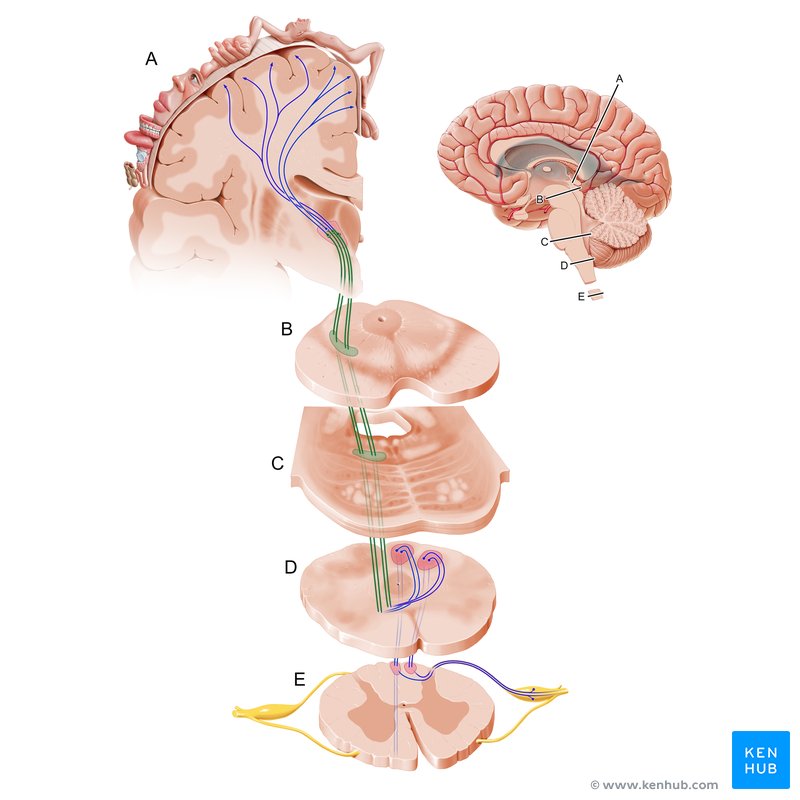
The 3-Neuron Chain (Step by Step):
- Step 1 — 1st Order Neuron: The cell body sits in the dorsal root ganglion (a swelling just outside the spinal cord). Its peripheral process detects stimuli from the skin, joints, and muscles. Its central process enters the spinal cord and immediately turns ipsilaterally upward directly into the dorsal columns.
- Step 2 — Dorsal Column Ascent: The 1st order axon ascends straight up the spinal cord without synapsing all the way to the medulla.
- Lower body fibers (legs, lower trunk) run in the fasciculus gracilis (medial).
- Upper body fibers (arms, upper trunk) run in the fasciculus cuneatus (lateral). The dividing line is approximately at the T6 spinal level.
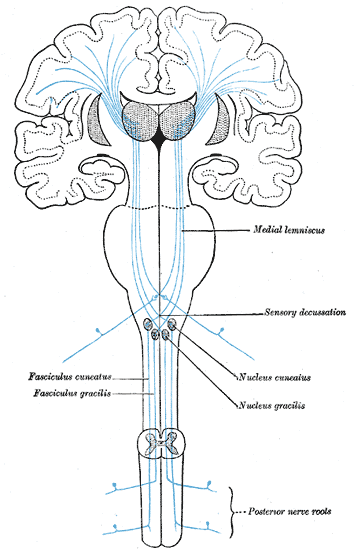
- Step 3 — First Synapse: In the caudal medulla of the brainstem, these 1st order axons finally synapse on 2nd order neurons located in the nucleus gracilis (lower body) and nucleus cuneatus (upper body).
- Step 4 — Sensory Decussation: The newly activated 2nd order axons curve ventrally as internal arcuate fibers and physically cross the midline in the caudal medulla. This exact crossing point is known as the sensory decussation.
- Step 5 — Medial Lemniscus: After crossing over, these axons bundle together to form a tract called the medial lemniscus. They ascend through the entire brainstem (pons, midbrain) to reach the VPL (Ventral Posterolateral) nucleus of the thalamus.
- Step 6 — Thalamus to Cortex: 3rd order neurons project from the VPL thalamus, passing through the posterior limb of the internal capsule, and ultimately terminate in the primary somatosensory cortex (the postcentral gyrus of the parietal lobe).
Key Points to Remember for DCML:
- Fasciculus gracilis = lower body (legs, lower trunk). Fibers from lower spinal levels are added medially. Mnemonic: "Gracilis = Graceful legs."
- Fasciculus cuneatus = upper body (arms, upper trunk). Fibers from upper spinal levels are added laterally. Mnemonic: "Cuneatus = Arms."
- Decussation happens in the CAUDAL MEDULLA — NOT in the spinal cord. This is critically important for accurate lesion localization.
- Damage before decussation (a lesion in the spinal cord) leads to ipsilateral loss of fine touch, vibration, and proprioception.
- Damage after decussation (a lesion in the medial lemniscus, thalamus, or internal capsule) leads to contralateral loss.
Tabes Dorsalis (Neurosyphilis): Late-stage Treponema pallidum infection causes selective degeneration of the dorsal columns and dorsal roots. Patients entirely lose proprioception and vibration sense. This leads to a characteristic "stamping gait" — they walk with heavy, slapping steps to try and feel the ground through crude touch and hearing. The Romberg test (standing with eyes closed) is markedly positive.
Vitamin B12 Deficiency (Subacute Combined Degeneration): B12 deficiency simultaneously damages BOTH the dorsal columns (causing proprioception and vibration loss) AND the lateral corticospinal tracts (causing UMN signs like spasticity and hyperreflexia). This exact combination is pathognomonic. Patients also often present with megaloblastic anemia and a beefy red tongue.
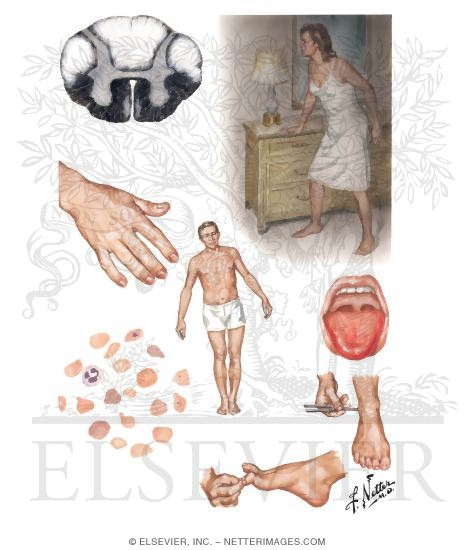
Figure 5: Subacute combined degeneration — Netter illustration showing dorsal column and lateral CST damage with clinical features
B. Spinothalamic Tract (Anterolateral System)
Modalities Carried: Pain, temperature, and crude (rough, non-discriminative) touch.
This is the essential pathway for nociception and thermoception — the body's ability to detect harmful stimuli and temperature changes. Unlike the highly precise DCML, this pathway provides much less precise localization of stimuli.
The 3-Neuron Chain (Step by Step):
- Step 1 — 1st Order Neuron: The cell body resides in the dorsal root ganglion. Peripheral processes detect pain (via nociceptors), temperature (via thermoreceptors), and crude touch. The central process enters the spinal cord via the dorsal root.
- Step 2 — Lissauer's Tract: Upon entering, 1st order axons travel 1 to 2 spinal segments up or down in Lissauer's tract (the dorsolateral fasciculus) before synapsing. This longitudinal spread allows pain signals to recruit adjacent segments for broader protective withdrawal reflexes.
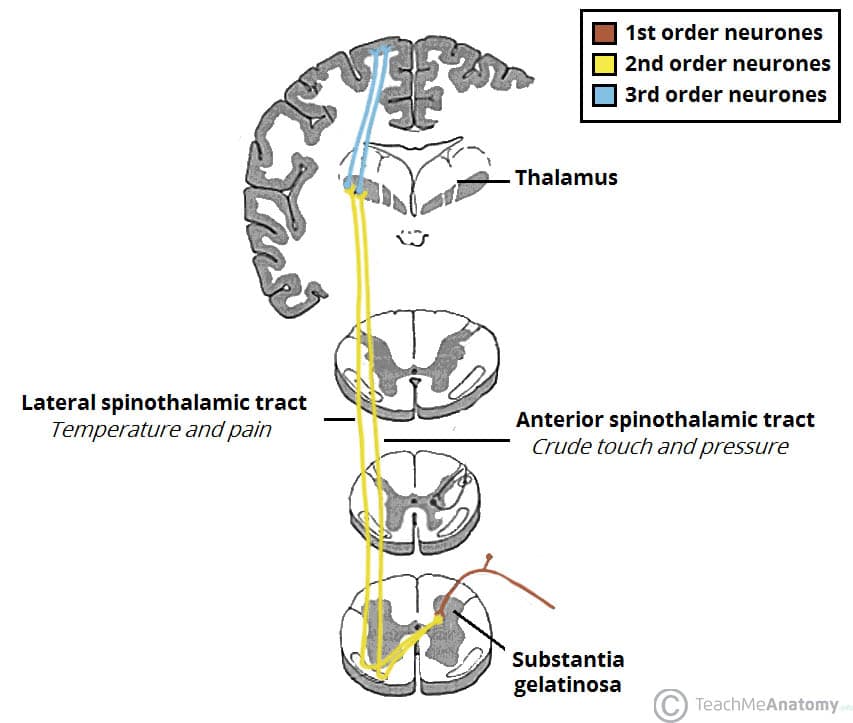
- Step 3 — First Synapse: Axons officially synapse on 2nd order neurons located in the substantia gelatinosa (Rexed laminae I and II) of the dorsal horn. This is the primary physiological site for pain modulation — this is exactly where endogenous opioids (endorphins/enkephalins) and opioid analgesic drugs act to block pain transmission.
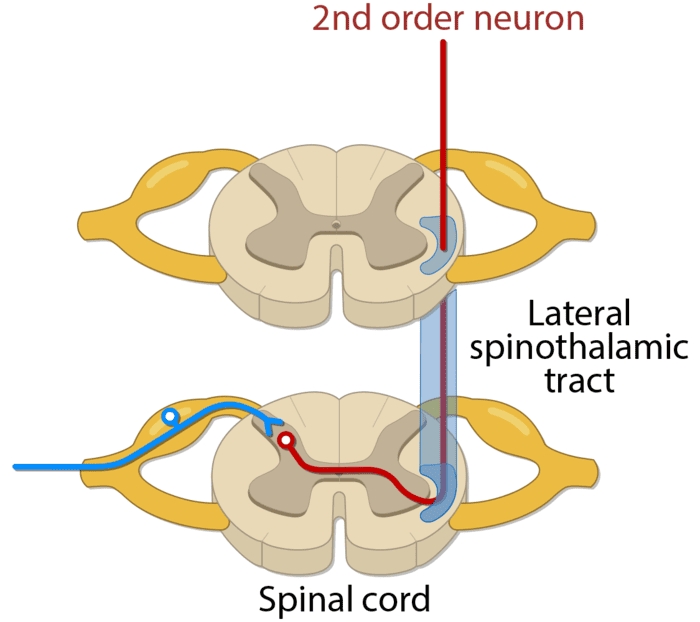
- Step 4 — Immediate Decussation: The 2nd order axons cross immediately through the anterior white commissure to the opposite side of the spinal cord. This crossing happens within 1-2 segments of their entry point.
- Step 5 — Ascent in Spinothalamic Tract: The crossed axons ascend in two divisions: the lateral spinothalamic tract (carrying pain and temperature) or the anterior spinothalamic tract (carrying crude touch and pressure). They travel through the brainstem, merging to reach the VPL nucleus of the thalamus.
- Step 6 — Thalamus to Cortex: 3rd order neurons project through the internal capsule to terminate in the primary somatosensory cortex (postcentral gyrus).
Key Points to Remember for Spinothalamic:
- Lissauer's tract allows pain signals to spread to adjacent spinal segments before synapsing. This explains why a single pinprick can trigger a massive withdrawal reflex involving multiple muscle groups across multiple segments.
- Substantia gelatinosa is the first synapse site and the main location for pain modulation. Enkephalins and endorphins released here actively inhibit ascending pain transmission.
- Decussation happens IMMEDIATELY directly in the spinal cord via the anterior white commissure. This is fundamentally different from the DCML, which waits to decussate high up in the medulla.
- A spinal cord lesion will therefore cause contralateral loss of pain and temperature (because the fibers carrying that information have already crossed within 1-2 segments of entering).
- The spinothalamic tract carries crude touch (in its anterior division). This explains why patients with completely severed DCML pathways can still feel being touched — they just cannot localize it precisely.
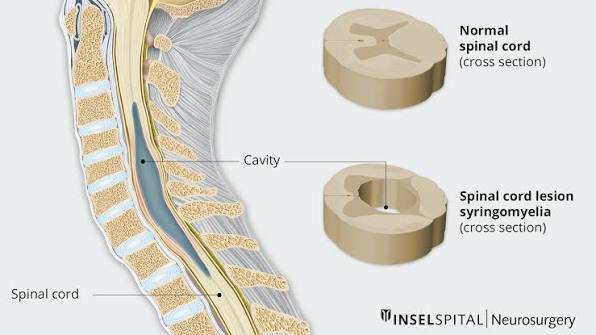
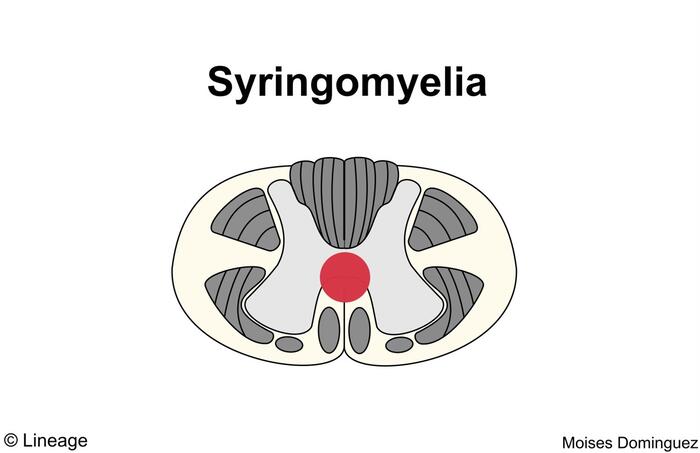
Syringomyelia
Syringomyelia is a fluid-filled cystic cavity (syrinx) that pathologically forms directly in the center of the spinal cord, typically in the cervical region. As this cavity gradually expands, it physically compresses and destroys the anterior white commissure — which is the exact crossing point of the spinothalamic fibers.
Because the crossing fibers from both the left and right arms are cut, this produces a highly characteristic bilateral, cape-like loss of pain and temperature draped over the shoulders and upper arms.
However, because the DCML runs safely far in the posterior columns (entirely unaffected by the central cavitation), fine touch and proprioception remain completely preserved. This finding of "dissociated sensory loss" is pathognomonic for syringomyelia.
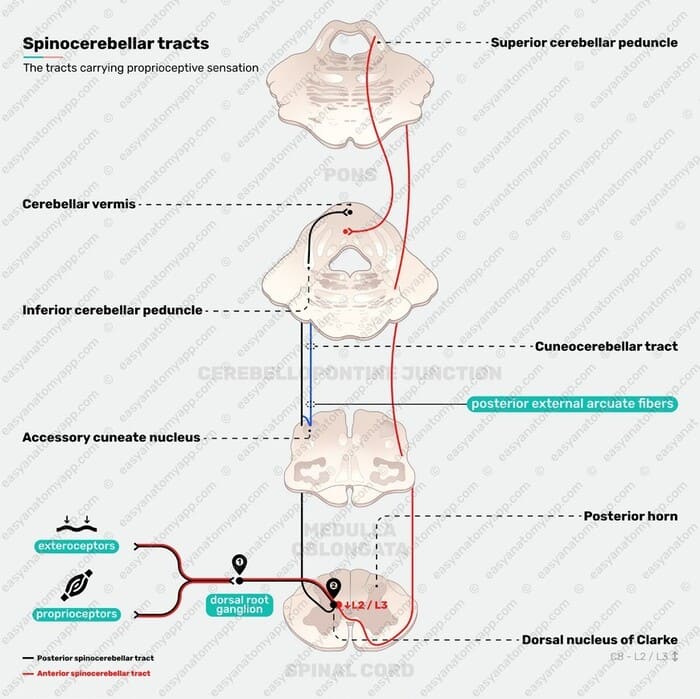
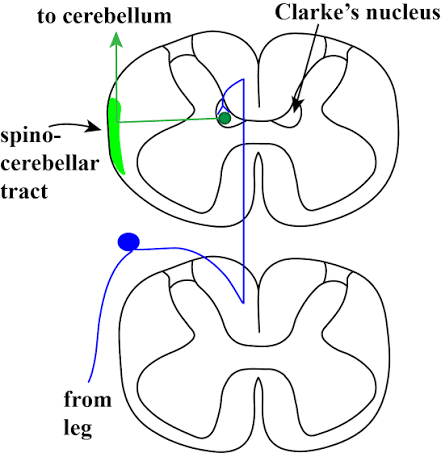
C. Spinocerebellar Tracts (Unconscious Proprioception)
These specific tracts carry vital information about muscle and joint position directly to the cerebellum without conscious awareness. They do not reach the cerebral cortex. They are essential for rapid coordination, balance, and smooth, fluid movement.
| Feature | Posterior (Dorsal) Spinocerebellar | Anterior (Ventral) Spinocerebellar |
|---|---|---|
| Origin | Clarke's nucleus (nucleus dorsalis) in intermediate zone | Intermediate zone of anterior horn |
| Spinal levels | T1–L2 only | All levels |
| 1st order neuron | Enters dorsal horn, synapses in Clarke's nucleus at SAME level | Enters dorsal horn, synapses in intermediate zone at SAME level |
| Decussation | None — remains completely ipsilateral | Decussates once in spinal cord (crosses to opposite side) |
| Path to cerebellum | Inferior cerebellar peduncle (ipsilateral) | Superior cerebellar peduncle (decussates AGAIN inside the cerebellum) |
| Function | Precise proprioception from the individual muscles of the trunk and lower limb | Coordination of the whole limb movement |
Why both tracts end up ipsilateral to the cerebellum:
The cerebellum controls the same side of the body (unlike the cerebral cortex). Therefore, all cerebellar tracts must ultimately end up on the ipsilateral side.
- Posterior spinocerebellar tract: Never crosses at any point. The 1st order neuron synapses in Clarke's nucleus, and the 2nd order neuron enters the cerebellum via the inferior cerebellar peduncle on the SAME side. It is a simple, direct path.
- Anterior spinocerebellar tract: Much more complex. The 1st order neuron synapses in the intermediate zone. The 2nd order neuron crosses the midline in the spinal cord and ascends in the opposite lateral funiculus. It then enters the cerebellum via the superior cerebellar peduncle, where it dramatically crosses back again (a double decussation). Because it crosses twice, the two crossings mathematically cancel each other out, so the information successfully reaches the correct ipsilateral cerebellum.
Clinical Note: Friedreich's Ataxia
Damage specifically targeting the spinocerebellar tracts (e.g., in Friedreich's ataxia, a hereditary degenerative disease) causes a profound loss of coordination, ataxic gait, and dysmetria (the inability to correctly judge distance during movement, leading to past-pointing). Because these are strictly unconscious pathways, patients absolutely cannot compensate for this voluntarily, no matter how hard they try.
4. Descending (Motor) Tracts
Motor commands travel from the cerebral cortex and brainstem down to the spinal cord lower motor neurons through simple two-neuron chains. These powerful pathways control voluntary movement, adjust posture, and modulate reflexes.
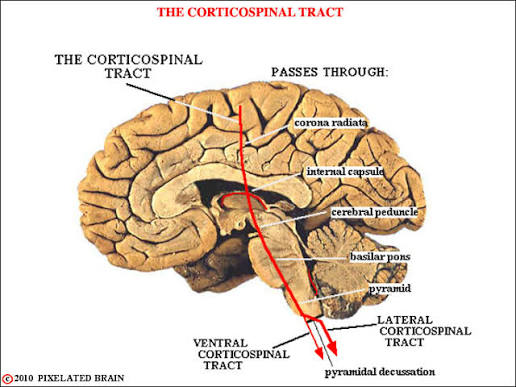
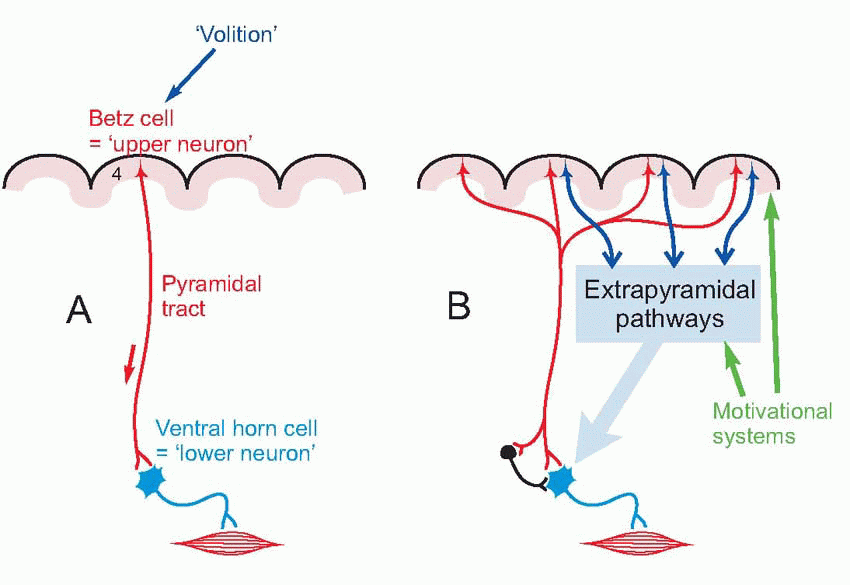
A. Corticospinal (Pyramidal) Tract
Function: This is the absolute main pathway for voluntary, skilled movement. It is the only direct cortical projection to spinal motor neurons.
The 2-Neuron Chain (Step by Step):
- Step 1 — Upper Motor Neuron (UMN): The cell body is a giant pyramidal cell of Betz (or smaller pyramidal cells) located in the primary motor cortex (the precentral gyrus, Brodmann area 4) and surrounding premotor/supplementary areas. These Betz cells are the largest neurons found in the cerebral cortex.
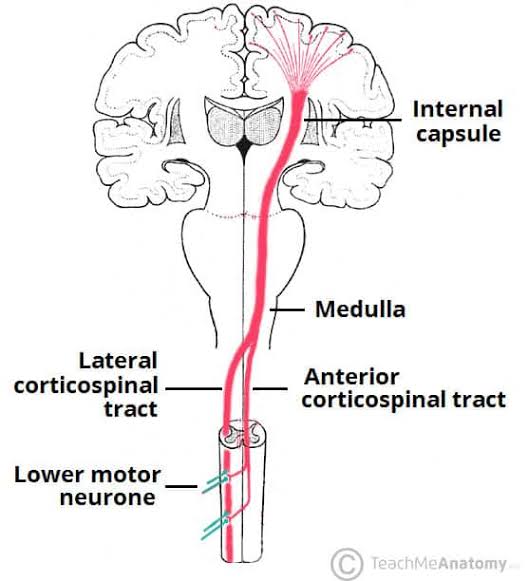
- Step 2 — Descent Through Brain: The UMN axon descends through the white matter of the corona radiata → squeezes through the posterior limb of the internal capsule (where leg fibers are medial and arm fibers are lateral) → descends through the cerebral peduncle (middle 3/5ths) in the midbrain → passes through the pons (where fibers become scattered) → and finally forms the thick medullary pyramids in the medulla.
- Step 3 — Pyramidal Decussation: At the very bottom of the medulla (the caudal medulla), 85-90% of fibers cross to the opposite side (this is the pyramidal decussation) to form the lateral corticospinal tract. The remaining 10-15% of fibers remain uncrossed, continuing straight down as the anterior corticospinal tract.
- Step 4 — Lateral Corticospinal Tract: The crossed fibers descend in the lateral funiculus and synapse directly on lower motor neurons in the anterior horn. These specific fibers control distal muscles, especially the hands and feet — the muscles requiring the finest, most delicate control.
- Step 5 — Anterior Corticospinal Tract: The uncrossed fibers descend in the anterior funiculus and finally cross at the exact segmental level (spinal cord level) right before synapsing. These fibers control proximal and trunk muscles — coordinating posture and gross movements.
- Step 6 — Lower Motor Neuron (LMN): The cell body is in the anterior horn of the spinal cord. Its axon exits via the ventral root, joins a peripheral nerve, and innervates skeletal muscle fibers directly at the neuromuscular junction.
Key Points to Remember for Corticospinal:
- Somatotopic organization is maintained throughout the entire pathway: In the internal capsule, leg fibers are most medial, arm fibers are lateral, and face fibers (corticobulbar) are most lateral.
- The lateral corticospinal tract controls fine, skilled movements — especially independent finger dexterity. A lesion here completely wipes out the ability to move fingers independently (like playing a piano).
- The anterior corticospinal tract controls postural and gross movements — ensuring trunk stability and bilateral coordination.
- Acute UMN damage (e.g., spinal shock immediately after a trauma) initially causes a deceptive flaccid paralysis and areflexia. It is only after days to weeks that the classic spasticity and hyperreflexia develop as the spinal reflexes become uninhibited by the dead UMN.
UMN vs. LMN Lesions — The Critical Comparison
| Sign | UMN Lesion | LMN Lesion |
|---|---|---|
| Weakness | Present (spastic paralysis) | Present (flaccid paralysis) |
| Muscle tone | Increased (spasticity) | Decreased (hypotonia) |
| Deep tendon reflexes | Hyperreflexia (exaggerated) | Hyporeflexia/areflexia (absent) |
| Babinski sign | Present (toes fan upward) | Absent (normal plantar flexion) |
| Clonus | Present (rhythmic oscillations) | Absent |
| Muscle atrophy | Mild, disuse atrophy only | Severe, rapid neurogenic atrophy |
| Fasciculations | Absent | Present (spontaneous muscle twitching) |
| Location of lesion | Above anterior horn (cortex, internal capsule, brainstem, spinal cord white matter) | Anterior horn, ventral root, peripheral nerve, neuromuscular junction |
Amyotrophic Lateral Sclerosis (ALS)
ALS (Lou Gehrig's disease) is a devastating neurodegenerative disease that mysteriously damages BOTH the lateral corticospinal tract (UMNs) and the anterior horn cells (LMNs). This produces a highly unique, simultaneous combination of spasticity (from the UMN loss) and severe muscle atrophy with fasciculations (from the LMN loss) present in the exact same limb. Crucially, there is no sensory loss because the sensory tracts are entirely spared.
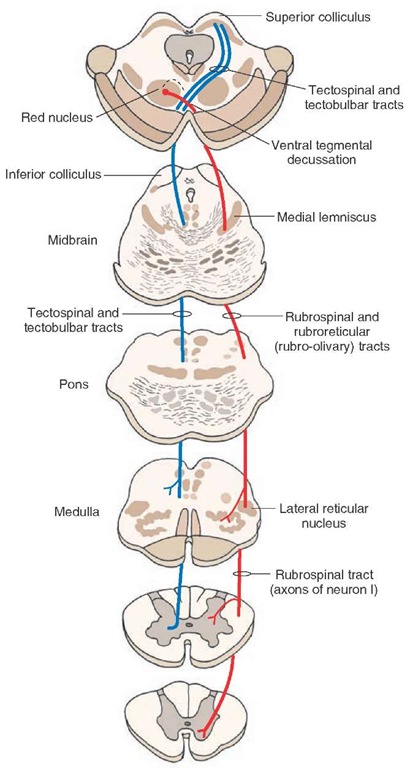
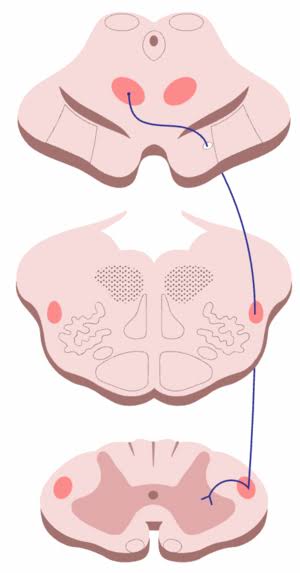
B. Rubrospinal Tract
- Origin: The Red nucleus located in the midbrain (mesencephalon).
- Function: Facilitates flexor muscle tone, predominantly functioning in the upper extremities. It works as a flexor antagonist to the extensor-promoting vestibulospinal tract.
- Decussation: Crosses immediately inside the midbrain via the ventral tegmental decussation (located just below the red nucleus).
- Path: After crossing, the tract descends straight through the pons and medulla into the lateral funiculus of the spinal cord, where it synapses on interneurons that influence the lower motor neurons.
Clinical Correlation: Decorticate vs. Decerebrate Posturing
These severe postures result from catastrophic brainstem lesions at different levels. They graphically demonstrate the delicate balance between flexor tone (rubrospinal) and extensor tone (vestibulospinal).
- Decorticate posturing (lesion ABOVE the red nucleus, e.g., an internal capsule hemorrhage): Because the lesion is high up, the rubrospinal tract remains intact and unopposed. Therefore, the arms are rigidly flexed (rubrospinal flexor facilitation), while the legs are extended (vestibulospinal extensor tone).
- Decerebrate posturing (lesion AT or BELOW the red nucleus, e.g., a midbrain lesion): The rubrospinal tract is destroyed. Now, BOTH arms and legs are rigidly extended because the vestibulospinal extensor tone dominates completely unopposed. This indicates deeper brainstem damage and carries a significantly worse prognosis.
Mnemonic: "Decorticate = arms flexed toward the CORE (cortex). Decerebrate = all limbs extended out like a rigid BEAM."
C. Vestibulospinal and Reticulospinal Tracts (Extrapyramidal)
These are the involuntary postural and balance pathways that modulate spinal reflexes and unconsciously maintain our upright posture against gravity. Crucially, they do NOT originate from the motor cortex.
Vestibulospinal Tracts:
- Lateral vestibulospinal tract: Originates from the lateral vestibular nucleus (Deiters' nucleus) in the pons. It strongly excites extensor motor neurons (the anti-gravity muscles) to maintain an upright posture. It receives direct sensory input from the inner ear (semicircular canals and otolith organs) about the head's exact position and acceleration.
- Medial vestibulospinal tract: Originates from the medial vestibular nucleus. It specifically controls head and neck position via rapid, reflexive turning movements. It only descends as far as the cervical and upper thoracic spinal cord levels.
Reticulospinal Tracts:
- Pontine (medial) reticulospinal tract: Originates from the pontine reticular formation. It heavily facilitates extensor tone and works synergistically alongside the vestibulospinal tract to maintain posture.
- Medullary (lateral) reticulospinal tract: Originates from the medullary reticular formation. It inhibits extensor tone, successfully allowing voluntary movement (from the corticospinal tract) to override our rigid postural reflexes. This inhibition is absolutely essential for initiating any movement.
5. Integrative Clinical Correlations
This section synthesizes your knowledge of individual tracts to understand complex clinical syndromes. The ability to predict deficits directly from a lesion location is the ultimate test of neuroanatomy mastery.
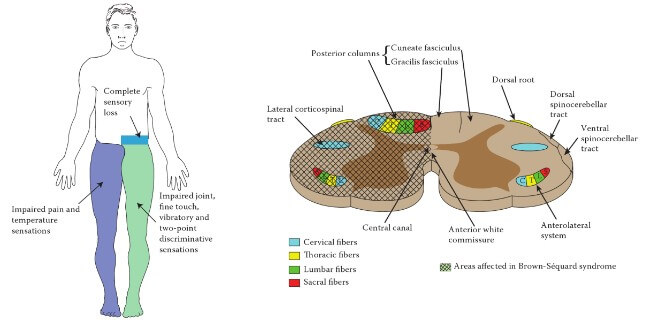
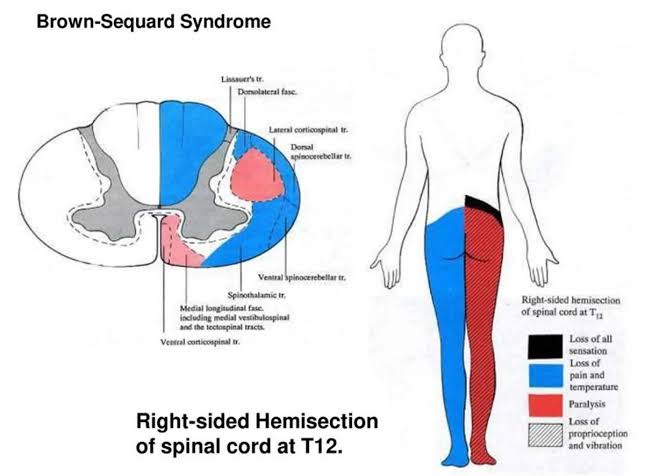
A. Brown-Séquard Syndrome (Spinal Cord Hemisection)
This occurs when a lesion cuts exactly half of the spinal cord (e.g., from a stab wound, a localized tumor, or a severe multiple sclerosis plaque). Fully understanding this syndrome requires knowing the exact decussation point of each individual tract.
At the exact level of the lesion (ipsilateral):
- Complete sensory loss in the specific dermatome at the lesion level (because all afferent sensory fibers entering the cord at that exact level are physically destroyed).
- LMN signs (flaccid paralysis, areflexia, severe muscle atrophy) because the anterior horn cells at that exact level are destroyed.
Below the level of the lesion:
| Deficit | Side | Tract | Why? (The Anatomical Reason) |
|---|---|---|---|
| Loss of proprioception, vibration, fine touch | Ipsilateral | DCML | 1st order neurons ascend on the same side and have NOT yet decussated (they wait to cross in the medulla). |
| Loss of pain and temperature | Contralateral | Spinothalamic | Fibers already decussated 1-2 segments above their entry point via the anterior white commissure. The cut tract contains fibers from the other side of the body. |
| UMN signs (spastic paralysis, hyperreflexia) | Ipsilateral | Lateral corticospinal | UMNs have already decussated high up at the pyramidal decussation in the medulla, so they are descending on the same side as the target muscle. |
| Loss of coordination | Ipsilateral | Spinocerebellar | Both posterior and anterior tracts ultimately project ipsilaterally to the cerebellum. |
Summary Mnemonic: "Same side motor, same side touch; opposite side pain."
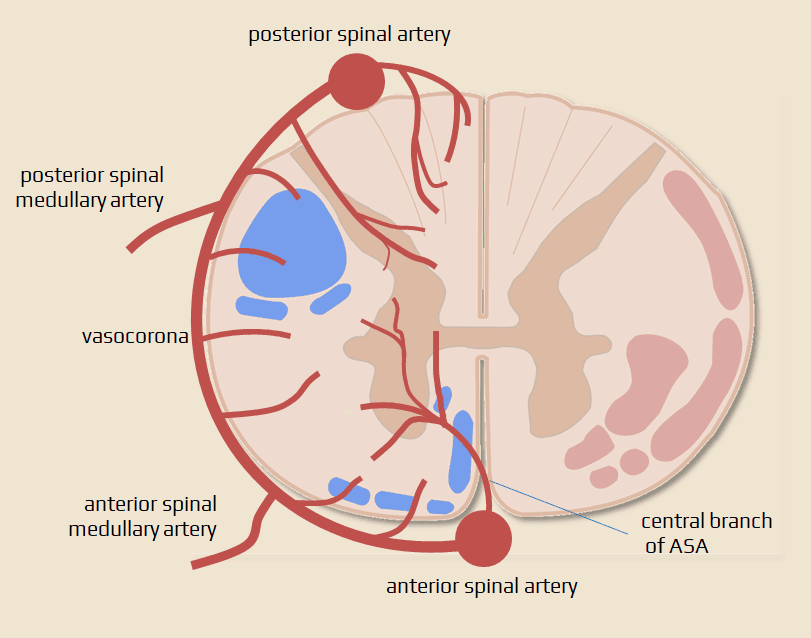
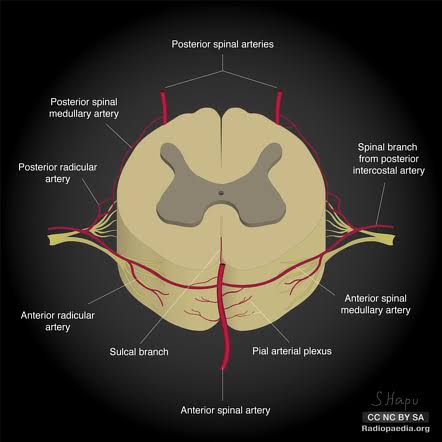
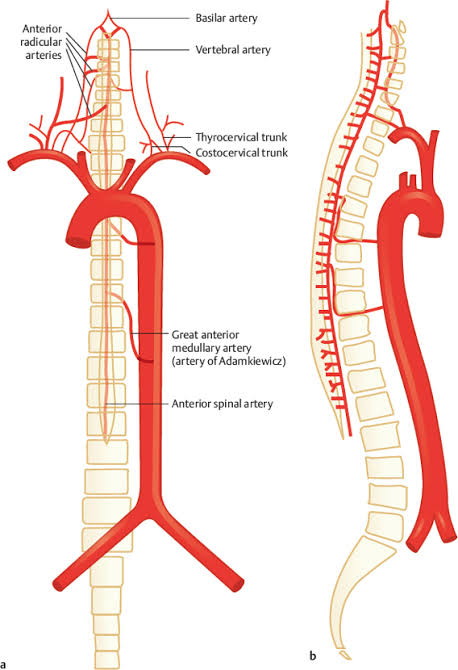
B. Blood Supply of the Spinal Cord
The spinal cord receives its blood from one anterior and two posterior spinal arteries. Understanding this vascular map instantly explains why certain tracts are highly vulnerable to ischemia while others remain spared.
- Anterior Spinal Artery (ASA):
- A single artery running straight down the anterior median fissure.
- It supplies the entire anterior two-thirds of the spinal cord.
- It gives off deep sulcal branches that penetrate into the cord.
- Supplies: Lateral corticospinal tract, spinothalamic tract, anterior corticospinal tract, and most of the gray matter.
- Posterior Spinal Arteries (PSA):
- Two separate arteries running down along the posterolateral sulci (one on each side).
- They supply the posterior one-third of the spinal cord.
- Supplies: Dorsal columns (fasciculus gracilis and cuneatus), posterior spinocerebellar tract, and the dorsal horn.
- Radicular Arteries:
- Segmental arteries branching from the aorta (intercostal and lumbar arteries) that reinforce the spinal arteries at various levels along the back.
- The great anterior radiculomedullary artery (Artery of Adamkiewicz): This is the largest and most critical reinforcement. It typically arises from a left intercostal or lumbar artery between levels T9 and L2 and provides the massive blood supply for the lower two-thirds of the spinal cord. Accidental damage to this artery during abdominal aortic surgery can cause catastrophic paraplegia.
C. Anterior Spinal Artery Occlusion (Anterior Cord Syndrome)
A blockage of the anterior spinal artery (e.g., from an aortic dissection, heavy atherosclerosis, or profound hypotension during surgery) produces a characteristic syndrome based entirely on which tracts are choked off versus which are spared by the posterior arteries.
Damaged (anterior 2/3 of cord):
- Bilateral motor loss: Both lateral corticospinal tracts are ischemic → results in spastic paralysis below the lesion (presenting with UMN signs: hyperreflexia, clonus, Babinski sign).
- Bilateral pain and temperature loss: Both spinothalamic tracts are ischemic → results in loss of pain and temperature sensation below the lesion.
- Bladder and bowel dysfunction: The autonomic control fibers running in the lateral funiculi are affected.
Spared (posterior 1/3 of cord):
- Dorsal columns are completely intact: Proprioception, vibration, and fine touch are PRESERVED. This is the absolute hallmark of anterior cord syndrome. The patient can feel the exact position of their toes and sense a tuning fork perfectly, but they cannot move their legs or feel a painful pinprick.
- Posterior spinocerebellar tracts are intact: Unconscious proprioception to the cerebellum survives, meaning coordination may be relatively better preserved than expected if any motor function returns.
Clinical Pearl
The combination of preserved proprioception alongside motor and pain/temperature loss is diagnostic for an ASA occlusion. Ask the patient: "Can you tell me which toe I am moving up or down?" (Yes, DCML proprioception is spared). Then ask: "Can you feel this sharp pinprick?" (No, spinothalamic is damaged).
6. Quick Reference: Lesion Localization
A summary table for rapid review before exams or clinical rounds.
| Condition | Tract(s) Damaged | Key Finding |
|---|---|---|
| Tabes dorsalis | Dorsal columns | Loss of proprioception + vibration; stamping gait; Romberg test positive. |
| Vitamin B12 deficiency | Dorsal columns + lateral CST | Loss of proprioception + UMN signs (spasticity, hyperreflexia); megaloblastic anemia. |
| Syringomyelia | Anterior white commissure | Bilateral cape-like loss of pain/temp; preserved fine touch; dissociated sensory loss. |
| Brown-Séquard | Hemisection of cord | Ipsilateral motor + proprioception loss; contralateral pain/temp loss. |
| Anterior spinal artery occlusion | Anterior 2/3 of cord | Bilateral motor + pain/temp loss; proprioception SPARED. |
| ALS | Lateral CST + anterior horn cells | BOTH UMN and LMN signs; no sensory loss; fasciculations present. |
| Friedreich's ataxia | Spinocerebellar tracts | Ataxia, dysmetria, loss of coordination; preserved conscious sensation. |
7. Decussation Cheat Sheet
You must know these decussation points cold. They determine whether a lesion causes ipsilateral or contralateral deficits.
| Tract | Where It Decussates | Clinical Rule |
|---|---|---|
| DCML (2nd order neuron) | Caudal medulla (sensory decussation) | Spinal cord lesion → ipsilateral loss |
| Spinothalamic (2nd order neuron) | Immediately in spinal cord (anterior white commissure) | Spinal cord lesion → contralateral loss |
| Posterior spinocerebellar | Does NOT decussate | Always ipsilateral to cerebellum |
| Anterior spinocerebellar | Spinal cord (then crosses back in the cerebellum) | Double decussation → ipsilateral to cerebellum |
| Lateral corticospinal | Caudal medulla (pyramidal decussation) | Spinal cord lesion → ipsilateral UMN signs |
| Anterior corticospinal | At segmental level in spinal cord | Crosses just before synapsing on LMN |
| Rubrospinal | Immediately in midbrain (ventral tegmental decussation) | Lesion above red nucleus → decorticate (flexed arms) |
8. Mnemonics & Memory Aids
These mnemonics will help you rapidly recall key facts during high-stress exams and clinical practice.
- Gracilis vs. Cuneatus:
"Gracilis = Graceful legs" → Fasciculus gracilis = lower body
"Cuneatus = Arms" (cune sounds like cue for arms) → Fasciculus cuneatus = upper body - Decussation Timing:
"Pain crosses EARLY" → Spinothalamic decussates immediately in the cord
"Touch crosses LATE" → DCML decussates high in the medulla - Brown-Séquard Summary:
"Same side motor, same side touch; opposite side pain" - Anterior Spinal Artery:
"Anterior artery = anterior deficits; posterior spared" → Motor and pain/temp are lost; proprioception is completely preserved. - UMN vs. LMN:
UMN = Everything goes UP (increased tone, increased reflexes, toes go UP for Babinski).
LMN = Everything goes DOWN (decreased tone, decreased reflexes, decreased muscle bulk). - Decorticate vs. Decerebrate:
"Decorticate = arms flexed toward the CORE (cortex)"
"Decerebrate = all limbs extended out like a rigid BEAM" - Sensory = 3, Motor = 2:
Think of dialing a telephone: you need 3 numbers to dial long-distance to the brain (sensory = 3 neurons), but only 2 numbers for a quick local call out to the muscles (motor = 2 neurons).