Blood supply of the CNS
Comprehensive Notes on the Blood Supply of the Central Nervous System
By the end of this comprehensive guide, you will be deeply conversant with:
- The complete Arterial Inflow pathways to the brain, including the Internal Carotid and Vertebrobasilar systems.
- The anatomical layout and functional importance of the Circle of Willis as a collateral network.
- The specific Cerebral Cortical Territories (ACA, MCA, PCA) and their functional correlates, including watershed zones.
- The intricate Deep Structure & Brainstem Perfusion, including the vulnerable lenticulostriate arteries.
- The layout of Spinal Cord Blood Supply and the critical Artery of Adamkiewicz.
- The Venous Drainage & Dural Sinuses, highlighting the anatomy and vulnerability of the cavernous sinus.
- Key Clinical Anatomy & Pathophysiology, distinguishing between stroke syndromes, lacunar infarcts, and types of intracranial hemorrhages (Epidural, Subdural, Subarachnoid).
1. Arterial Inflow to the Brain & The Circle of Willis
The brain is a highly metabolically active organ. Despite accounting for only about 2% of total body weight, it receives 15-20% of the body's cardiac output and consumes 20% of its oxygen. This massive demand is met by two major arterial systems that converge at the base of the brain.
A. The Anterior Circulation (Internal Carotid System)
The anterior circulation supplies the majority of the cerebral hemispheres, specifically the frontal, parietal, and lateral temporal lobes, as well as deep structures like the basal ganglia.
- Pathway from the Heart: Aortic Arch → Brachiocephalic trunk (on the Right) / Left Common Carotid (on the Left) → Common Carotid Artery (CCA).
- Bifurcation: The CCA bifurcates at the C3-C4 vertebral level into the External Carotid (supplying the face/neck) and the Internal Carotid Artery (ICA).
- Distribution: The ICA enters the skull and ultimately bifurcates into the Anterior Cerebral Artery (ACA) (supplying the medial hemisphere) and the Middle Cerebral Artery (MCA) (supplying the lateral hemisphere).
The Four Segments of the Internal Carotid Artery (ICA)
| Segment | Course and Anatomical Significance |
|---|---|
| 1. Cervical | Runs from the CCA bifurcation to the skull base. Contains NO branches in the neck. This is the primary site for atherosclerotic plaque buildup (evaluated via auscultation for bruits and treated with carotid endarterectomy). |
| 2. Petrous | Enters the carotid canal within the petrous portion of the temporal bone. It runs anterior to the cochlea. A fracture here can lead to massive epistaxis (nosebleeds) or hearing issues. |
| 3. Cavernous | Passes directly through the cavernous venous sinus, forming an S-shaped curve known as the "carotid siphon." It is intimately surrounded by cranial nerves (CN III, IV, V1, V2, VI). Trauma here can cause a carotid-cavernous fistula. |
| 4. Cerebral (Supraclinoid) | Pierces the dura mater to become intradural. It gives off important branches: Ophthalmic artery, Posterior Communicating Artery (PCoA), and Anterior Choroidal Artery (AChA), before finally bifurcating into the ACA and MCA. |
B. The Posterior Circulation (Vertebrobasilar System)
The posterior circulation supplies the brainstem, cerebellum, occipital lobes, and inferior temporal lobes.
- Pathway: Subclavian Artery → Vertebral Artery → Ascends through the transverse foramina of cervical vertebrae (C6-C1) → Enters the skull via the Foramen Magnum.
- The Basilar Artery: The two vertebral arteries merge at the pontomedullary junction to form the single Basilar Artery, which runs up the front of the pons.
- Distribution: The basilar artery bifurcates at the midbrain into the two Posterior Cerebral Arteries (PCA). These join the Circle of Willis via the Posterior Communicating Arteries (PCoA).
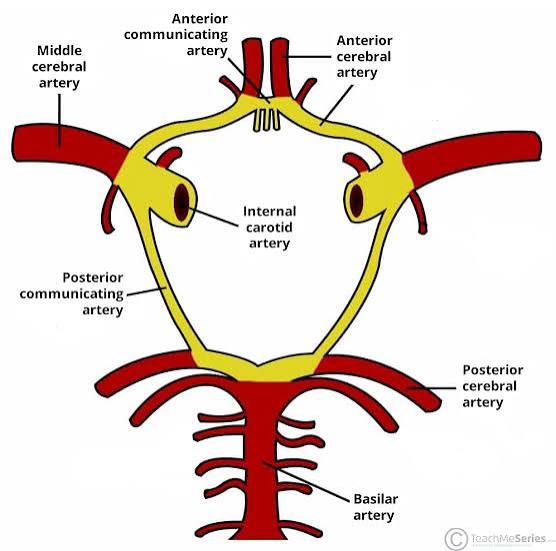
C. The Circle of Willis
The Circle of Willis is a ring of vessels at the base of the brain that connects the anterior and posterior circulations, as well as the left and right sides of the brain.
It serves as a critical pressure-equalizing anastomotic network. If one major artery slowly occludes (e.g., gradual ICA stenosis), blood can reroute across the communicating arteries to maintain perfusion to the deprived area, preventing a stroke. Interestingly, a complete, anatomically perfect circle is present in only ~50% of individuals (many have hypoplastic or missing segments, reducing this collateral capacity).
Components of the Circle:
- Anterior Communicating Artery (AComm): Connects the left and right ACAs. This is the most common site for berry aneurysms.
- Anterior Cerebral Artery (ACA): Supplies the medial cerebral hemispheres.
- Internal Carotid Artery (ICA): The main input for the anterior system.
- Posterior Communicating Artery (PComm): The vital bridge connecting the ICA (anterior) to the PCA (posterior).
- Posterior Cerebral Artery (PCA): Formed from the basilar artery; supplies the occipital lobe.
- Basilar Artery: (While technically the input, it is the foundation of the posterior portion of the circle).
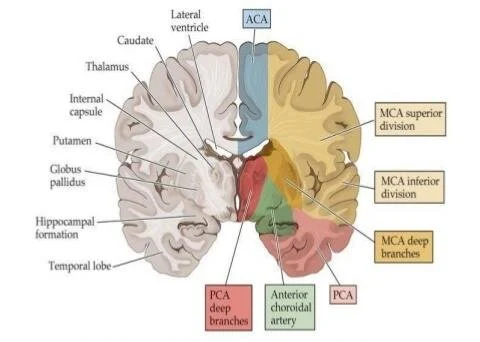
2. Cerebral Cortical Territories & Watershed Zones
Understanding which artery supplies which part of the brain cortex is essential for diagnosing strokes based on a patient's physical symptoms. This relies heavily on the "motor and sensory homunculus"—the map of the body on the brain's surface.
Arterial Territories & Functional Correlates
| Artery | Cortical Surface Supplied | Key Functional Areas Affected | Classic Stroke Deficits |
|---|---|---|---|
| ACA (Anterior Cerebral) | Medial Surface: Medial frontal and parietal lobes, cingulate gyrus, anterior corpus callosum. | Motor & sensory cortex for the LEG and FOOT, prefrontal cortex (executive function), micturition center. | Contralateral leg weakness > arm weakness. Urinary incontinence. Personality changes, abulia (lack of will), akinetic mutism. Grasp reflex return. |
| MCA (Middle Cerebral) | Lateral Surface: Most of the lateral convexity (precentral, postcentral, inferior frontal, superior temporal, angular gyri), insula. | Motor & sensory cortex for the FACE and ARM. Broca's area (speech production - dominant side). Wernicke's area (speech comprehension). | Contralateral face/arm weakness > leg weakness. Aphasia (if dominant hemisphere, usually left). Hemineglect (if non-dominant, usually right). Gaze deviation toward the lesion. |
| PCA (Posterior Cerebral) | Medial Occipital & Inferior Temporal: Lingual gyrus, calcarine sulcus, cuneus, thalamus (deep). | Primary Visual Cortex (calcarine fissure), visual association areas, memory formation. | Contralateral homonymous hemianopia (loss of half the visual field) with macular sparing. Alexia without agraphia (can write but can't read). Thalamic pain syndromes. |
Watershed Zones (Border Zones)
Watershed zones are the regions at the very periphery of arterial territories where the most distal branches of two different major arteries meet.
- Why are they vulnerable? Because they represent the absolute end of the line for blood flow, they have the lowest perfusion pressure. During states of severe systemic hypotension (e.g., massive blood loss, cardiac arrest, or severe shock), the brain shunts blood to core territories first to survive. The distal watershed areas dry up first, leading to ischemic infarcts.
- ACA-MCA Watershed: Located high on the lateral convexity. Infarct causes proximal arm and shoulder weakness (classic "man in a barrel" syndrome where the trunk and proximal limbs are paralyzed but hands and face are spared).
- MCA-PCA Watershed: Located in the posterior temporal-parietal-occipital junction. Infarct causes complex higher-order visual and language processing deficits.
- Internal Border Zones: Deep white matter zones situated between the deep penetrating lenticulostriate arteries and the superficial cortical branches of the MCA.
3. Deep Structures, Ventricles & Brainstem Perfusion
While the large cortical branches supply the surface, tiny, fragile penetrating arteries dive straight into the brain tissue to supply the critical relay stations (basal ganglia, thalamus, internal capsule) and the life-sustaining brainstem.
A. Blood Supply to the Ventricles (Choroid Plexus)
To address the specific vascularization of the ventricular system (which produces Cerebrospinal Fluid via the choroid plexus):
- Anterior Choroidal Artery (AChA): A direct branch of the distal ICA. It supplies the choroid plexus of the lateral ventricles, as well as the optic tract, hippocampus, and posterior limb of the internal capsule.
- Posterior Choroidal Arteries (Medial and Lateral): Branches of the PCA. They supply the choroid plexus of the third and lateral ventricles, and parts of the thalamus.
B. Lenticulostriate Arteries
- Origin: Arise at sharp 90-degree angles directly from the M1 segment of the MCA. There are typically 6-12 small vessels.
- Structures Perfused: Caudate nucleus, putamen, globus pallidus, and the critical internal capsule (posterior limb and genu).
- Vulnerability: Because these are "end-arteries" with NO collateral circulation, and because they branch off a high-pressure main pipe at a sharp angle, they are extremely susceptible to hypertensive damage (lipohyalinosis and microatheroma), leading to Lacunar Infarcts.
- Note: The Recurrent Artery of Heubner is an analogous deep branch originating from the ACA, supplying the anteromedial caudate and anterior limb of the internal capsule.
C. Thalamic Blood Supply
The thalamus is the brain's central sensory relay station, supplied almost entirely by deep branches of the Posterior Cerebral Artery (PCA):
- Thalamoperforating arteries (P1 segment): Supply the medial thalamus.
- Thalamogeniculate arteries (P2 segment): Supply the lateral thalamus (including the VPL/VPM nuclei for bodily and facial sensation).
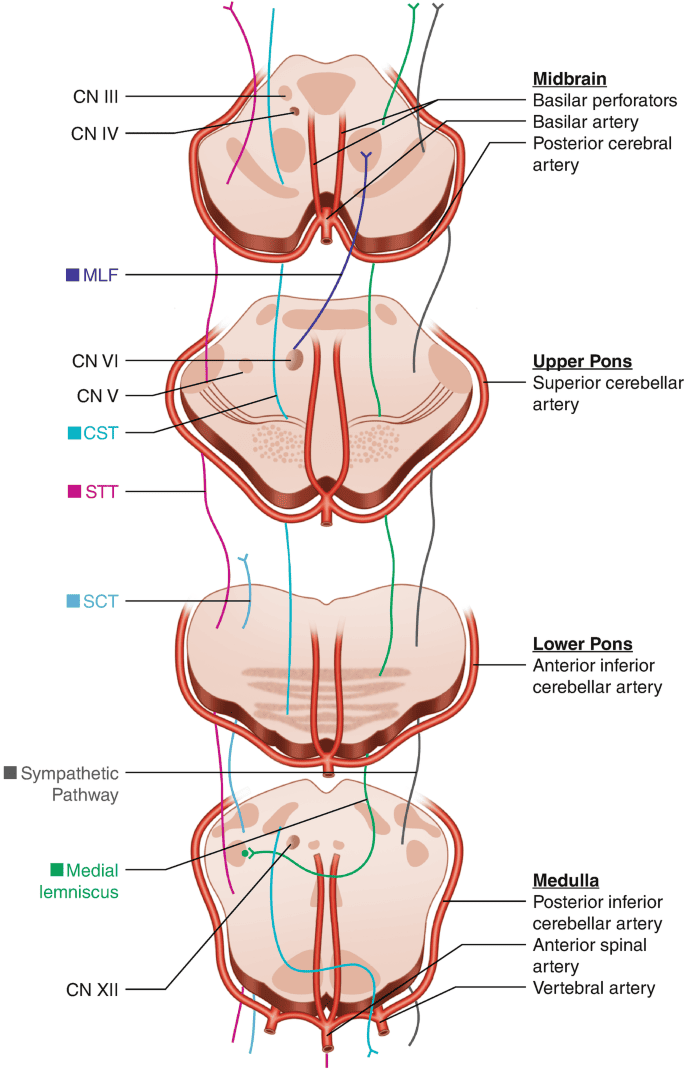
D. Brainstem Blood Supply Zones
The brainstem (midbrain, pons, medulla) is supplied by the vertebrobasilar system. Each level is divided into Medial and Lateral vascular zones.
| Region | Medial Supply (Paramedian Branches) | Lateral Supply (Circumferential Branches) |
|---|---|---|
| Midbrain | Basilar apex + PCA (P1). Supplies: Red nucleus, CN III/IV, MLF. Syndrome: Weber syndrome (CN III palsy + contralateral hemiparesis). |
PCA (P2) + Superior Cerebellar Artery (SCA). Supplies: Lateral lemniscus, colliculi. |
| Pons | Basilar Artery (paramedian branches). Supplies: Abducens nerve (CN VI), MLF, pyramidal tracts (motor). Massive infarct causes Locked-in Syndrome. |
Basilar Artery + Anterior Inferior Cerebellar Artery (AICA). Supplies: Facial nerve (CN VII), Vestibulocochlear nerve (CN VIII), spinal trigeminal nucleus. |
| Medulla | Anterior Spinal Artery (ASA) + Vertebral Artery. Supplies: Corticospinal tract, medial lemniscus, hypoglossal nerve (CN XII). | Vertebral Artery + Posterior Inferior Cerebellar Artery (PICA). Supplies: Spinothalamic tract, vestibular nuclei, nucleus ambiguus. Syndrome: Wallenberg (Lateral Medullary) Syndrome. |
4. Spinal Cord Blood Supply
The spinal cord relies on a delicate balance of longitudinal arteries running its entire length, reinforced by horizontal arteries feeding in from the body wall.
A. Longitudinal Arteries
- Anterior Spinal Artery (ASA):
- Origin: Formed by the fusion of branches from both vertebral arteries near the foramen magnum.
- Course: A single, continuous artery running down the anterior median fissure.
- Territory: Supplies the Anterior 2/3 of the cord. This includes the motor tracts (corticospinal), pain/temperature tracts (spinothalamic), and anterior horn motor cells.
- Posterior Spinal Arteries (PSA):
- Origin: Arise from the vertebral arteries or PICA.
- Course: Paired arteries running down the posterolateral sulci.
- Territory: Supply the Posterior 1/3 of the cord. This specifically includes the dorsal columns (responsible for fine touch, vibration, and proprioception) and the dorsal grey matter.
B. Segmental Medullary Arteries
The ASA and PSAs alone are not powerful enough to supply the entire length of the spinal cord. They must be reinforced at irregular intervals by radicular and medullary arteries arising from the aorta (via intercostal and lumbar arteries). The most dominant of these exist to keep the lower cord alive.
The Artery of Adamkiewicz (Great Anterior Radiculomedullary Artery)
- Origin: Typically arises from a left posterior intercostal artery between T8 and L2 (in 75% of people).
- Significance: It is the largest single feeder to the ASA, providing the dominant blood supply for the lower thoracic, lumbar, and sacral spinal cord.
- Vulnerable Zone: The mid-thoracic cord (T2-T10) is a watershed zone with very few segmental feeders, making it highly susceptible to ischemic injury.
- Clinical Relevance: During complex thoracoabdominal aortic surgeries (like aneurysm repairs), clamping the aorta can block the Artery of Adamkiewicz. This leads to Anterior Spinal Artery Syndrome: The patient wakes up paralyzed from the waist down (paraplegia) with complete loss of pain and temperature sensation below the lesion, BUT preserved vibration and proprioception (because the posterior 1/3 supplied by the PSAs is intact).
5. Venous Drainage & Dural Sinuses
Unlike veins in the rest of the body, cerebral veins lack valves and have extremely thin walls without a muscular layer. They drain into large, endothelium-lined channels formed between layers of the dura mater called Dural Venous Sinuses.
A. Major Cerebral Veins & Sinus Flow Pathway
- Superior Cerebral Veins: Drain the lateral/superior cortical surfaces directly into the Superior Sagittal Sinus (located along the upper margin of the falx cerebri).
- Great Vein of Galen: Drains deep structures (thalamus, basal ganglia). It joins with the Inferior Sagittal Sinus to form the Straight Sinus.
- The Flow Pathway:
Superior Sagittal Sinus + Straight Sinus meet at the back of the skull at the Confluence of Sinuses (Torcular Herophili).
From there, blood flows outward laterally into the Transverse Sinuses.
The Transverse Sinuses curve downward to become the S-shaped Sigmoid Sinuses.
The Sigmoid Sinuses exit the skull via the jugular foramen to become the Internal Jugular Veins (IJV), returning blood to the heart.
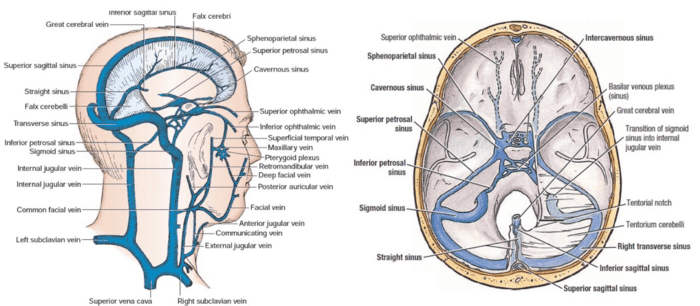
B. The Cavernous Sinus
Located on either side of the sella turcica (which houses the pituitary gland), this sinus is unique because multiple vital structures pass directly through it. It receives blood from the ophthalmic veins and superficial MCA veins, eventually draining into the petrosal sinuses.
- Through the center: Internal Carotid Artery (ICA) with its surrounding sympathetic plexus.
- Free-floating within the sinus: Abducens Nerve (CN VI). Because it is floating next to the ICA, it is the most vulnerable nerve to aneurysms or pressure here.
- Embedded in the lateral wall (top to bottom): Oculomotor (CN III), Trochlear (CN IV), Ophthalmic (CN V1), and Maxillary (CN V2).
Often caused by infections spreading backward from the face/nose via valveless ophthalmic veins.
Symptoms include:
- Painful ophthalmoplegia (paralysis of eye movements due to CN III, IV, VI palsies).
- Sensory loss over the forehead and cheek (CN V1/V2).
- Severe proptosis (bulging eye) and chemosis due to venous congestion.
6. Clinical Anatomy & Pathophysiology
Combining the anatomical pathways above allows us to quickly pinpoint the location of vascular lesions based purely on clinical presentation.
A. Lacunar Infarcts
Small (<15mm) ischemic strokes occurring in deep, penetrating artery territories. Because these vessels (like the lenticulostriate arteries) have no collateral supply, occlusion leads to highly specific, localized tissue death.
- Pure Motor Stroke: Caused by a lacunar infarct in the posterior limb of the internal capsule or the basis pontis. The internal capsule packs motor fibers tightly together. A tiny stroke here wipes out motor control to the contralateral face, arm, and leg equally, with absolutely NO sensory or visual deficits. This accounts for ~45% of all lacunar strokes.
- Pure Sensory Stroke: Caused by a lacunar infarct in the ventral posterolateral (VPL) nucleus of the thalamus (supplied by thalamogeniculate arteries). Presents as contralateral sensory loss (pain, temperature, touch) across the face, arm, and leg, with no motor weakness. Can eventually lead to Dejerine-Roussy syndrome (severe post-stroke thalamic pain).
B. Intracranial Hemorrhages: Anatomical Contrast
Understanding exactly which vessel breaks defines the type of hematoma and the clinical presentation.
| Type of Hemorrhage | Location | Vascular Source | CT Scan Appearance | Classic Clinical Presentation |
|---|---|---|---|---|
| Epidural Hematoma | Between Skull & Dura mater. | Middle Meningeal Artery (Arterial bleed, high pressure). Usually due to skull fracture at the pterion. | Biconvex (lens-shaped). Does NOT cross suture lines. | Rapid deterioration. Classic "Lucid Interval" (patient gets knocked out, wakes up fine, then rapidly declines into coma). Ipsilateral blown pupil, contralateral hemiparesis. |
| Subdural Hematoma | Between Dura & Arachnoid mater. | Bridging Veins (Venous bleed, low pressure). Prone to tearing from sheer force due to brain atrophy (elderly, chronic alcoholics). | Crescent-shaped (moon-shaped). Crosses suture lines. | Gradual, insidious onset. Fluctuating consciousness, vague headaches, focal deficits. Can be acute (major trauma) or chronic. |
| Subarachnoid Hemorrhage (SAH) | Within Subarachnoid space (where CSF flows). | Rupture of Berry Aneurysm (often at AComm or MCA bifurcation). Arterial bleed. | Blood tracking deeply into CSF spaces, basal cisterns, and sulci. Hydrocephalus risk. | Sudden, absolutely explosive "Worst headache of my life" (Thunderclap headache). Nuchal rigidity, photophobia, meningismus. |
Quick Reference Summary & Takeaways
- Anterior Circulation: ICA → ACA (Leg) + MCA (Face/Arm).
- Posterior Circulation: Vertebral → Basilar → PCA (Vision).
- Collateral Safety: Circle of Willis routes blood via AComm and PComm.
- Watershed Vulnerability: Border zones (ACA-MCA, MCA-PCA) suffer first during massive blood pressure drops.
- Spinal Cord Safety: Artery of Adamkiewicz is the massive backup generator for the lower spine's ASA.
- Cavernous Sinus Danger: CN VI is free-floating next to the ICA; highly susceptible to pressure/thrombosis.
- Bleed Types: Epidural = Arterial/Lens/Lucid; Subdural = Venous/Crescent/Elderly; SAH = Aneurysm/Thunderclap.
List of References:
- Core Vascular Anatomy & Pathophysiology: Complete Illustrated Notes. (Generated 2026-06-30).
- Core Vascular Neuroanatomy: Comprehensive Illustrated Learning Notes. Professional Medical Education Resource.
- Content synthesized and structured based on standard medical neuroanatomy and vascular pathophysiology curricula regarding cerebrovascular arterial inflow, cortical territories, brainstem perfusion, spinal cord supply, and associated clinical syndromes.