Internal Structures (Ventricles) of tha CNS & Cerebrospinal Fluid (CSF) Dynamics
By the conclusion of this exhaustive master guide, you will be deeply conversant with the internal structures of the Central Nervous System, specifically focusing on:
- The Embryological Origins of the neural tube and how it develops into the adult ventricular system.
- The intricate Structural Morphology and Boundaries of the lateral, third, and fourth ventricles, as well as the cerebral aqueduct.
- The comprehensive CSF Hydrodynamics and Flow Kinetics, from production to resorption.
- The specific Foramina and Communications that act as doorways between the ventricular chambers.
- The Neuroradiological Correlations for identifying these structures on CT and MRI scans.
- The Clinical Pathophysiology of Hydrocephalus and raised intracranial pressure.
1. Embryological Origins: From Neural Tube to Adult Ventricles
To truly understand the complex, winding shapes of the adult ventricles, we must first look at how they develop. The entire ventricular system is simply the adult remnant of the original hollow center of the embryonic neural tube.
The Neural Tube Timeline
- Week 3: The neural plate forms from the ectoderm on the dorsal surface of the embryo.
- Week 4: The neural plate folds inward to form the neural groove, and the edges fuse to create the neural tube. It closes from the middle outward (like a zipper). Failure of this closure leads to neural tube defects (e.g., Spina Bifida).
- The Core Concept: The hollow center of this neural tube becomes the fluid-filled ventricular system of the brain and the central canal of the spinal cord. Think of it like a simple garden hose that eventually gets pinched, bent, and ballooned out into different shapes.
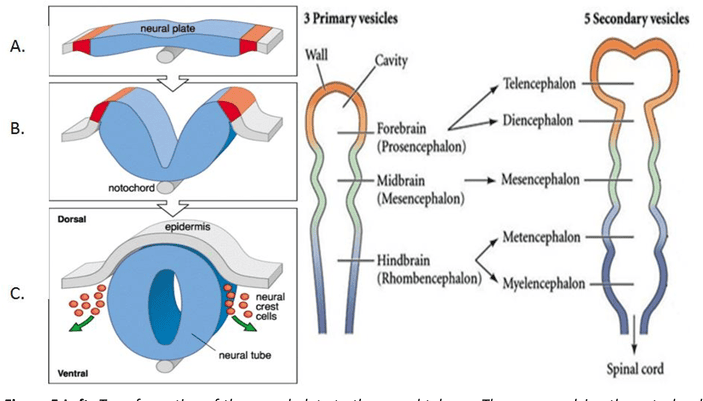
Primary Brain Vesicles (Weeks 4-5)
The anterior (head) end of the neural tube swells into three primary fluid-filled chambers:
The most anterior portion. The hollow space inside will eventually become the Lateral and 3rd Ventricles.
The middle portion. The hollow space here narrows to become the Cerebral Aqueduct.
The posterior portion. The hollow space becomes the 4th Ventricle.
Note: The rest of the neural tube extending down the back becomes the spinal cord, and its hollow center becomes the extremely narrow Central Canal.
Secondary Vesicles: The Forebrain Splits
As development continues, the primary vesicles divide further to form the mature structures of the brain.
The Prosencephalon splits into:
- Telencephalon: This forms the massive cerebral hemispheres, basal ganglia, and hippocampus. Because it grows so large and splits into two hemispheres, its internal cavity also splits to form the paired, C-shaped Lateral Ventricles.
- Diencephalon: This forms the central core (thalamus, hypothalamus, epithalamus, subthalamus). Its internal cavity remains in the exact midline and forms the slit-like Third Ventricle.
The Rhombencephalon splits into:
- Metencephalon: Forms the pons and cerebellum.
- Myelencephalon: Forms the medulla oblongata.
- Both of these structures share the diamond-shaped Fourth Ventricle.
Key Memory Points for Embryology
- PRO = FORE = FRONT: The lateral and 3rd ventricles are in the FRONT of the brain.
- MESO = MIDDLE: The cerebral aqueduct runs through the MIDDLE of the brain (midbrain).
- RHOMBO = DIAMOND: The 4th ventricle is DIAMOND-shaped.
- Lateral ventricles are PAIRED because the telencephalon forms two distinct cerebral hemispheres.
- The 3rd ventricle is MIDLINE because the diencephalon is a single central structure.
- The cerebral aqueduct is the NARROWEST part—it is essentially a squeezed, unexpanded portion of the original neural tube lumen.
2. Structural Morphology: Boundaries, Recesses, and Relations
The ventricles are not empty voids; they are anatomically precise rooms bordered by specific brain structures. Knowing these borders is essential for neurosurgery and reading brain scans.
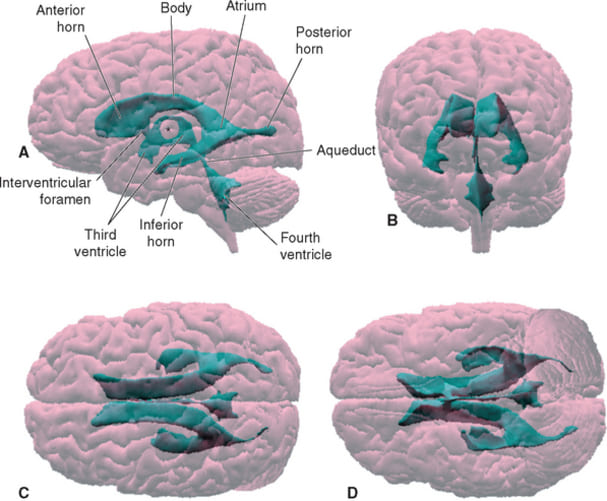
A. The Lateral Ventricles (The C-Shaped Chambers)
These are paired structures, one buried deep within each cerebral hemisphere. Each lateral ventricle is massive and has four distinct parts (a central body with three horn-like extensions):
| Region | Roof | Floor | Medial Wall | Lateral Wall |
|---|---|---|---|---|
| Frontal (Anterior) Horn Extends forward into the frontal lobe |
Corpus callosum (genu) | Head of the caudate nucleus | Septum pellucidum | Corpus callosum |
| Body (Central Part) The main horizontal portion |
Corpus callosum (body) | Thalamus + body of caudate nucleus | Septum pellucidum + fornix | Tapetum of the corpus callosum |
| Atrium (Trigone) The wide junction where the body, temporal, and occipital horns meet |
Corpus callosum | Collateral trigone | Crus of the fornix | Tapetum + optic radiation |
| Temporal (Inferior) Horn Curves downward and forward into the temporal lobe |
Tapetum + tail of caudate nucleus | Hippocampus (Very important landmark!) | Stria terminalis | Tapetum |
| Occipital (Posterior) Horn Extends backward into the occipital lobe |
Splenium of the corpus callosum | Collateral trigone | Crus of fornix + splenium | Tapetum |
B. The Third Ventricle (The Midline Slit)
The third ventricle is a narrow, vertical, slit-like cavity located exactly in the midline, sandwiched between the left and right halves of the diencephalon.
- Roof: Formed by the tela choroidea and the body of the fornix. The tela choroidea is a thin, two-layered membrane containing the highly vascular choroid plexus.
- Floor: Formed by the structures of the hypothalamus (including the mammillary bodies, tuber cinereum, and the optic chiasm).
- Anterior Wall: Formed by the lamina terminalis (a thin sheet of gray matter that marks the anterior limit of the original neural tube) and the anterior commissure.
- Posterior Wall: The pineal gland and the posterior commissure.
- Lateral Walls: Formed predominantly by the medial surfaces of the two thalami.
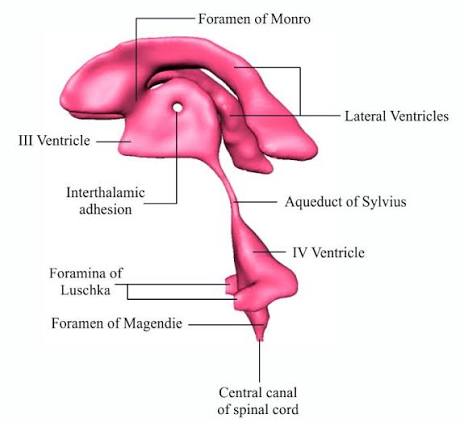
- Massa Intermedia (Interthalamic Adhesion): In about 70% of people, a small bridge of gray matter crosses directly through the center of the third ventricle to connect the left and right thalami.
Recesses of the 3rd Ventricle: These are small, blind-ended extensions of the fluid space pushing into surrounding structures. They include the Optic recess (above the optic chiasm), Infundibular recess (funneling down into the pituitary stalk), Pineal recess (pushing into the pineal gland), and Suprapineal recess.
C. The Cerebral Aqueduct (of Sylvius) — The Bottleneck
This is a narrow channel running through the center of the midbrain. It connects the 3rd ventricle above to the 4th ventricle below.
- Dimensions: Approximately 15 mm long and only 1-2 mm in diameter. It is the NARROWEST part of the entire ventricular system, making it highly susceptible to blockage.
- Surrounding Structures: It is entirely surrounded by a ring of gray matter called the Periaqueductal Gray (PAG). The PAG is a critical control center for descending pain modulation, fear responses, and autonomic control.
- Borders: Posterior to the aqueduct is the tectum (superior and inferior colliculi). Anterior to it is the tegmentum (containing the red nucleus and substantia nigra).
D. The Fourth Ventricle (The Diamond)
Located in the posterior fossa of the skull, this tent-like cavity sits between the brainstem in front and the cerebellum in back.
- Roof (Superior/Posterior boundary): Formed primarily by the superior medullary velum (anteriorly) and the inferior medullary velum + tela choroidea (posteriorly). The tela here contains choroid plexus.
- Floor (Anterior boundary): Formed by the posterior surface of the pons and upper medulla. This diamond-shaped floor is clinically referred to as the Rhomboid Fossa. It features important landmarks like the facial colliculus and hypoglossal trigone.
- Lateral Walls: Formed by the superior, middle, and inferior cerebellar peduncles (the thick stalks of white matter connecting the brainstem to the cerebellum).
3. CSF Hydrodynamics & Flow Kinetics
Cerebrospinal Fluid (CSF) is a crystal-clear, colorless liquid that constantly bathes the brain and spinal cord. It is dynamically produced, circulated, and absorbed in a continuous, never-ending cycle.
A. Production: The Choroid Plexus
The vast majority of CSF is actively manufactured by the Choroid Plexus, a cauliflower-like network of specialized blood vessels covered by ependymal cells.
- Locations: Found in the lateral ventricles (where the majority of CSF is made), the roof of the 3rd ventricle, and the roof of the 4th ventricle. (Note: There is NO choroid plexus in the cerebral aqueduct, frontal horns, or occipital horns).
- Mechanism: It is an ACTIVE transport process, not just passive filtering. Sodium-Potassium (Na+/K+) ATPase pumps actively move sodium into the ventricles, creating an osmotic gradient. Water follows the sodium through aquaporin channels. It also actively pumps bicarbonate to maintain a strict pH of ~7.33.
- Production Rate: The choroid plexus produces about 500 mL of CSF per day (roughly 20-25 mL per hour).
- Total System Volume: The entire ventricular and subarachnoid space only holds about 150 mL of CSF in an adult at any given time. Because 500 mL is made daily but the system only holds 150 mL, the entire volume of CSF is completely replaced 3 to 4 times every single day.
Normal CSF is 99% water. Compared to blood plasma, normal CSF has:
- Very Low Protein: (0.15-0.45 g/L) compared to plasma (~70 g/L).
- Normal Glucose: Usually about 60% of whatever the blood glucose level is (2.5-4.4 mmol/L). If CSF glucose drops severely, suspect bacterial meningitis (the bacteria are eating the sugar).
- Very Few Cells: Normal CSF contains fewer than 5 lymphocytes/mm³. Finding neutrophils or high cell counts indicates severe infection or inflammation.
- High Electrolytes: Chloride and magnesium are higher in CSF than in blood plasma, while potassium and urea are lower.
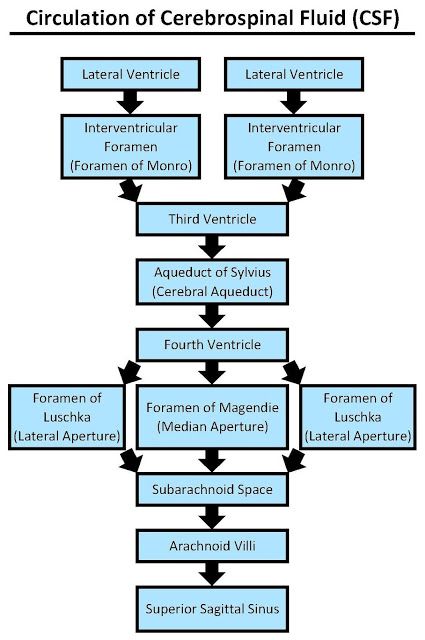
B. The Flow Pathway (Step-by-Step)
Think of CSF flow like a gentle underground river flowing outward to the sea. The flow is driven by the pressure gradient created by continuous production.
- Lateral Ventricles: Bulk of CSF is produced here.
- Foramina of Monro: CSF passes from each lateral ventricle into the midline 3rd ventricle.
- Third Ventricle: More CSF is added by the choroid plexus located in its roof.
- Cerebral Aqueduct: The fluid funnels down through the midbrain.
- Fourth Ventricle: More CSF is added. The fluid collects here before exiting the inside of the brain.
- Exit Foramina: The CSF leaves the ventricular system via three doors in the 4th ventricle: the midline Foramen of Magendie and the paired lateral Foramina of Luschka.
- Subarachnoid Space: The CSF now bathes the entire outer surface of the brain and spinal cord, filling large pooling areas called cisterns.
- Arachnoid Granulations: The fluid is pushed into these cauliflower-like projections of the arachnoid membrane that poke into the dural venous sinuses (mostly the superior sagittal sinus).
- Superior Sagittal Sinus: The CSF safely mixes back into the venous bloodstream and returns to the heart.
C. Functions of the CSF
- Buoyancy: The physical brain weighs about 1400g. By floating suspended in CSF, its effective weight drops to roughly 50g. This massive reduction in effective weight prevents the heavy brain from crushing its own delicate base and cranial nerves against the bony skull.
- Protection: Acts as a physical shock absorber against sudden trauma, acceleration, and deceleration.
- Homeostasis: Maintains a highly stable, tightly controlled ionic environment necessary for neuronal firing.
- Transport & Waste Removal: Delivers nutrients to deep brain tissue and actively flushes out metabolic waste products (especially during sleep).
D. Major Subarachnoid Cisterns
When the CSF exits the 4th ventricle, it enters the subarachnoid space. In certain areas where the brain pulls away from the skull, this space widens significantly to form large pools of fluid called cisterns.
- Cisterna Magna (Cerebellomedullary cistern): The largest cistern. Located between the cerebellum and the medulla. CSF from the Foramen of Magendie pools directly here. Can be tapped via needle puncture for CSF samples.
- Pontine Cistern: Anterior to the pons. Contains the crucial basilar artery.
- Interpeduncular Cistern: Between the cerebral peduncles of the midbrain. Contains the vessels of the Circle of Willis.
- Suprasellar (Chiasmatic) Cistern: Located above the sella turcica. Contains the optic chiasm.
- Ambient Cistern: Wraps around the sides of the midbrain.
- Quadrigeminal Cistern: Located above the cerebellum, behind the midbrain. Contains the great cerebral vein (of Galen).
4. Foramina and Communications: The Doorways
The ventricular system features five critical openings (doorways) and one major tunnel (the aqueduct). Blockage at any of these choke points causes obstructive hydrocephalus.
- Interventricular Foramina of Monro:
- Number: Paired (one on the left, one on the right).
- Function: Connects each lateral ventricle to the singular 3rd ventricle.
- Location: Located at the anterior-inferior corner of the lateral ventricle, bounded anteriorly by the column of the fornix and posteriorly by the anterior tubercle of the thalamus.
- Clinical Note: A benign, fluid-filled growth called a Colloid Cyst classically grows exactly at this foramen. It acts like a ball valve, suddenly blocking flow and causing severe, life-threatening sudden obstructive hydrocephalus.
- Cerebral Aqueduct (of Sylvius):
- Function: Connects the 3rd to the 4th ventricle.
- Clinical Note: It is the most common site of congenital obstruction (Aqueductal stenosis). Because it is surrounded by the midbrain tectum, tumors of the pineal gland push down on the midbrain and easily crush the aqueduct flat from the outside.
- Foramina of Luschka:
- Number: Paired (two lateral openings). Mnemonic: Luschka = Lateral.
- Location: Located at the extreme ends of the lateral recesses of the 4th ventricle, near the cerebellopontine angle.
- Function: Allows CSF to exit the inside of the brain into the cerebellopontine angle cisterns.
- Foramen of Magendie:
- Number: Single, midline opening. Mnemonic: Magendie = Midline.
- Location: Located in the inferior roof of the 4th ventricle.
- Function: The largest of the three exits. It opens directly into the massive cisterna magna.
Clinical rule: ALL THREE 4th ventricle foramina must be fully patent (open) for normal CSF flow. Blockage of any can cause fluid backup.
5. Neuroradiological Correlation
Understanding anatomy means recognizing it on clinical imaging. Different modalities highlight different aspects of the ventricles.
Imaging Modalities
| Modality | Best For | Ventricle/CSF Appearance | Key Advantage |
|---|---|---|---|
| CT (Non-contrast) | Acute hemorrhage, massive hydrocephalus, skull fractures. | CSF is dark (HYPOdense, 0-20 Hounsfield Units). Bone is bright white. | Very fast, widely available, excellent for unstable trauma patients. |
| T1-weighted MRI | Detailed anatomy, gray-white matter differentiation. | CSF is dark (HYPOintense). Fat is bright. | Excellent soft tissue contrast for structural abnormalities. |
| T2-weighted MRI | Pathology (edema, tumors), mapping CSF spaces. | CSF is bright white (HYPERintense). | The absolute best sequence for visualizing the exact shape of ventricles. |
| FLAIR MRI | Suppressing the bright CSF signal to see lesions next to the ventricles. | CSF is made dark (SUPPRESSED), but fluid in tissue (edema) stays bright. | Excellent for detecting periventricular lesions (like Multiple Sclerosis plaques). |
Recognizing Planes and Shapes
- Axial Plane (Top-down view):
- At a high level, the bodies of the lateral ventricles look like the wings of a butterfly, separated by the thin midline septum pellucidum.
- At a mid level, the 3rd ventricle appears as a very thin vertical slit between the large oval thalami. If this slit is wide and round, suspect hydrocephalus.
- At a low level, the 4th ventricle appears as a small diamond or arrowhead shape resting directly behind the brainstem.
- Coronal Plane (Front-to-back view): Best for visualizing the frontal horns and the inferiorly looping temporal horns simultaneously. The width of the temporal horns is a highly sensitive early marker for hydrocephalus; normally, they are barely visible slits.
- Normal Variants vs. Pathology:
- Cavum Septi Pellucidi: A harmless normal variant. Fluid collects between the leaflets of the septum pellucidum. Common in infants, usually fusing by 3-6 months.
- Hydrocephalus vs. Ex Vacuo: If a scan shows enlarged ventricles AND tightly packed, normal-looking cortical sulci, the pressure is high (Hydrocephalus). However, if a scan shows enlarged ventricles AND massively widened, gaping cortical sulci, the brain tissue itself has shrunk (atrophy). The ventricles merely expanded to fill the empty space. This is called Hydrocephalus Ex Vacuo and is seen in severe Alzheimer's or aging.
- Midline Shift: If the ventricular system is physically pushed off-center, it indicates a massive, dangerous pressure effect from a one-sided tumor, hematoma, or severe swelling.
6. Clinical Pathophysiology: Hydrocephalus ("Water on the Brain")
Hydrocephalus is the abnormal accumulation of CSF in the ventricles due to impaired production, impaired flow, or impaired absorption. It leads to ventricular ballooning and dangerous raised intracranial pressure (ICP).
Types of Hydrocephalus
The blockage is WITHIN the ventricular system itself. The fluid cannot physically flow out of the brain to communicate with the subarachnoid space.
Pathophysiology: Ventricles *proximal* to the blockage balloon massively, while ventricles *distal* to the blockage remain normal or shrink. This localized ballooning points the radiologist directly to the location of the block.
Common Causes:
- Foramen of Monro: Colloid cyst. (Sudden headache, syncope).
- 3rd Ventricle: Craniopharyngioma, pineal tumor.
- Cerebral Aqueduct: Aqueductal stenosis (web/forking), tectal glioma.
- 4th Ventricle: Ependymoma, Medulloblastoma, Dandy-Walker malformation (cerebellar signs, ataxia).
The blockage is OUTSIDE the ventricular system. The ventricles communicate freely with each other and the subarachnoid space, but the fluid cannot be absorbed into the venous blood.
Pathophysiology: Because flow is normal but absorption is blocked, ALL ventricles enlarge uniformly.
Common Causes:
- Post-hemorrhagic: Subarachnoid hemorrhage (SAH). Blood products physically clog the delicate arachnoid granulations.
- Post-infectious: Bacterial/TB meningitis. Severe inflammation scars and fibroses the arachnoid villi, destroying their absorptive capacity.
- Neoplastic: Leptomeningeal carcinomatosis (cancer cells floating in the CSF plug the granulations).
Aqueductal Stenosis: The Congenital Culprit
This is the most common cause of congenital obstructive hydrocephalus. It can be intrinsic (gliosis, inflammatory webs, or physical forking of the aqueduct into tiny channels) or extrinsic (a tumor pressing from the outside).
Imaging Hallmark: Massively enlarged lateral and 3rd ventricles, with a completely NORMAL or tiny 4th ventricle. The fluid gets stuck before reaching the 4th.
Treatment: Endoscopic Third Ventriculostomy (ETV) — a surgeon punches a tiny hole in the floor of the 3rd ventricle to create a new bypass directly to the subarachnoid space, or a traditional VP (Ventriculoperitoneal) shunt.
Normal Pressure Hydrocephalus (NPH) — "The Treatable Dementia"
NPH is a unique condition affecting the elderly, caused by chronically impaired CSF absorption combined with reduced brain compliance. Unlike classic hydrocephalus, the CSF pressure is generally normal or only intermittently elevated on a spinal tap.
The Classic Clinical Triad of NPH: "Wet, Wobbly, and Wacky"
- Gait Apraxia (Wobbly): The patient develops a distinctive "magnetic gait" — their feet seem glued to the floor, requiring a shuffling, wide-based walk. This is typically the FIRST and most prominent symptom, caused by the expanding ventricles stretching the motor nerve fibers controlling the legs.
- Urinary Incontinence (Wet): Starts as urgency and frequency, progressing to complete loss of bladder control.
- Cognitive Decline (Wacky): Memory loss, extreme apathy, slowness of thought, and poor attention. Unlike Alzheimer's disease, NPH patients are less confused and more "slowed down".
Diagnostic Test & Treatment: A high-volume CSF tap (removing 30-50 mL of fluid via lumbar puncture). If the patient's gait suddenly improves after the tap, it confirms NPH. The definitive treatment is placing a permanent VP shunt. Gait improves most reliably; cognitive decline is the hardest to reverse.
Clinical Signs of Raised Intracranial Pressure (ICP)
When hydrocephalus occurs, the skull acts as a rigid box (except in infants). Excess fluid has nowhere to go, causing life-threatening pressure on the brain tissue.
- Headache: Typically worse in the morning, exacerbated by coughing, sneezing, or lying flat (which increases venous pressure). Mechanism: stretching of pain-sensitive dural structures.
- Papilledema: Swelling of the optic disc seen on eye exam. Causes blurred vision. Mechanism: High pressure blocks normal axoplasmic flow down the optic nerve sheath.
- Nausea/Vomiting: Often sudden and projectile (not related to meals). Mechanism: Direct pressure on the area postrema (the brain's vomiting center in the medulla).
- Altered Consciousness: Ranges from drowsiness to deep coma. Mechanism: Direct compression of the brainstem and reticular activating system.
- Cushing Triad (Late, ominous sign): Hypertension + Bradycardia (slow heart rate) + Irregular breathing. Mechanism: The brainstem mounts a massive, desperate sympathetic response to force blood into the highly-pressurized skull.
- Sunsetting Eyes: The patient's eyes are forced downward; the whites (sclera) are visible above the iris. Mechanism: Pressure specifically on the tectum (superior colliculi) of the midbrain blocking upward gaze.
- Cranial Nerve Palsies: CN VI (Abducens nerve) palsy is the most common. It causes the eye to turn inward. It is a "false localizing sign" because the nerve is simply stretched tight by the shifting brain mass.
- Macrocephaly: Rapid, massive enlargement of the head circumference in infants. Mechanism: In babies, the cranial bone sutures have not yet fused, so the high pressure physically forces the skull bones apart.
List of References
- Crossman, A. R., & Neary, D. (2019). Neuroanatomy: An Illustrated Colour Text (6th ed.). Elsevier. (Excellent resource for visualizing the 3D morphology of the ventricular system and subarachnoid cisterns).
- Haines, D. E. (2018). Neuroanatomy in Clinical Context: An Atlas of Structures, Sections, Systems, and Syndromes (10th ed.). Wolters Kluwer. (Comprehensive atlas for correlating gross anatomy with neuroradiological imaging like CT and MRI).
- Ropper, A. H., Samuels, M. A., Klein, J. P., & Prasad, S. (2019). Adams and Victor's Principles of Neurology (11th ed.). McGraw-Hill Education. (Definitive text for the clinical pathophysiology of hydrocephalus, NPH, and raised intracranial pressure).
- Sadler, T. W. (2018). Langman's Medical Embryology (14th ed.). Wolters Kluwer. (Primary reference for the embryological timeline, neural tube development, and primary/secondary vesicle differentiation).