Embryology of the Head & Neck: Pharyngeal Arches
An exhaustive, highly detailed anatomical and clinical master guide covering the structure, derivatives, special organs, and clinical conditions of the Pharyngeal Arches.
By the conclusion of this comprehensive guide, you will be deeply conversant with:
- The Basic Structure & Organization of the pharyngeal apparatus (Arches, Clefts, and Pouches) and their embryonic timeline.
- The exhaustive list of Arch Derivatives, perfectly correlating each arch with its specific Cranial Nerve, Skeletal/Cartilaginous elements, Muscles, and Aortic Blood Vessels.
- The intricate embryonic development of Special Organs, specifically the Tongue, Face, Thyroid Gland, and Pharyngeal Pouch derivatives.
- The pathophysiology and presentation of major Clinical Conditions and Congenital Anomalies linked to developmental failures in this region.
SECTION 1: Basic Structure & Organization
1.1 When Do Pharyngeal Arches Develop? (The Embryonic Timeline)
The pharyngeal (branchial) arches are the fundamental building blocks of the head and neck. The term "branchial" is historically derived from the Greek word branchia, meaning "gill," because during early embryonic development, these human structures strongly resemble the gill slits seen in fish and amphibian embryos.
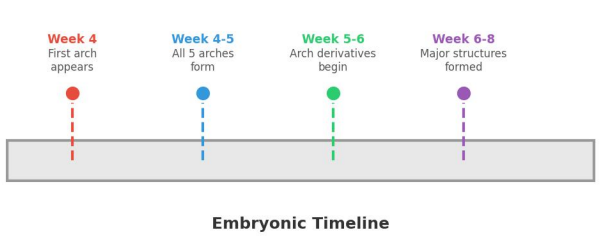
The development occurs rapidly during a highly vulnerable window of gestation:
- Week 4 (First Arch Appears): The head and neck region begins to take shape. The first pharyngeal arch appears as a distinct bar of mesoderm covered by ectoderm on the outside and endoderm on the inside.
- Weeks 4 to 5 (All Arches Form): All five human arches (labeled I, II, III, IV, and VI) form in a strict craniocaudal sequence (from top/head to bottom/tail).
Crucial Embryological Note: There is NO 5th Pharyngeal Arch in humans. In human embryos, the 5th arch either never forms at all, or it appears as a tiny, transient structure that regresses and disappears almost instantly without leaving any adult derivatives. - Weeks 5 to 6 (Derivatives Begin): Each arch acts as an independent factory, beginning to produce its own highly specific structures: a cranial nerve, an artery, muscle tissue, and a cartilage bar.
- Weeks 6 to 8 (Major Structures Formed): The arches remodel, fuse, and migrate. Their initial primitive derivatives morph into easily recognizable adult structures in the head and neck (e.g., the jaw, the bones of the middle ear, the larynx).
1.2 The Four Main Parts of Each Arch
Think of a pharyngeal arch as an independently pre-packaged "starter kit" for a segment of the neck. Every single arch consists of a core of mesodermal and neural crest tissue, and contains exactly four fundamental components:
Cranial Nerve Branch: Each arch is supplied by one specific cranial nerve that grows into it from the developing brainstem. This nerve will exclusively control the muscles that develop from that specific arch, and will provide sensory innervation to the skin/mucosa derived from it.
Aortic Arch Branch: Each arch has its own arterial blood supply, known as an aortic arch. These vessels arise from the primitive heart tube (aortic sac) and course through the arches. They eventually remodel to become the major arteries of the adult chest, neck, and head.
Skeletal Muscle: The muscle component is derived from the Mesoderm (specifically paraxial and lateral plate mesoderm). These muscle precursor cells migrate into the arch and differentiate into the skeletal muscles of facial expression, mastication, swallowing, and vocalization.
Skeletal Element: The cartilage and bone of the arches are derived primarily from Neural Crest Cells (neuroectoderm). These highly migratory cells travel into the arches to form the structural skeleton of the face, jaw, and neck.
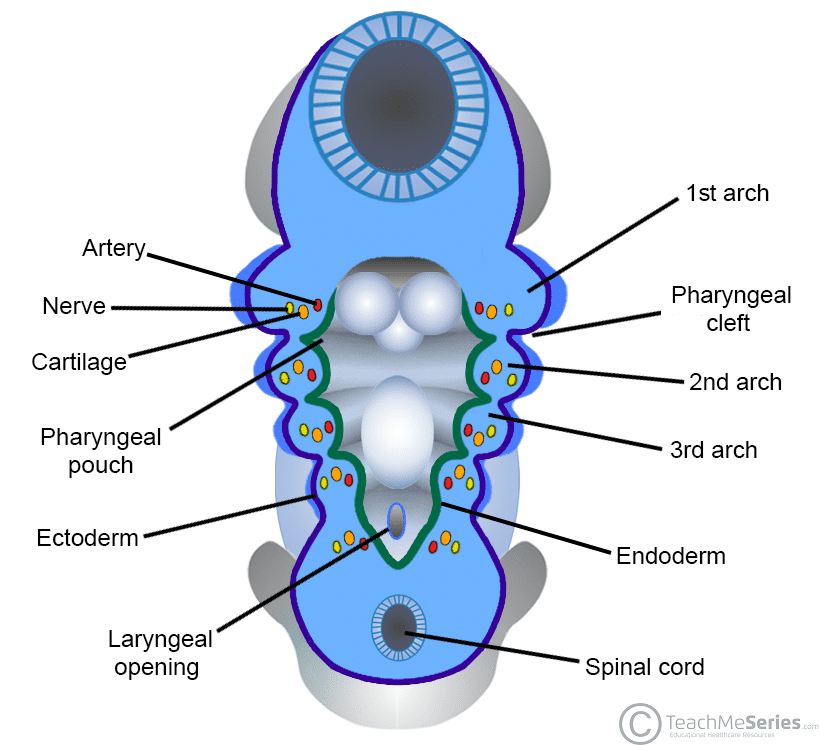
1.3 Arches vs. Clefts vs. Pouches (The Three Layers)
The pharyngeal apparatus is not just a solid block; it is corrugated. It consists of three distinct anatomical and embryological layers. Misunderstanding these layers is the leading cause of confusion in head and neck embryology.
| Structure | Anatomical Location | Embryonic Germ Layer Origin | What It Becomes (General Fate) |
|---|---|---|---|
| Pharyngeal Cleft (Groove) | The indentations on the OUTSIDE of the embryo neck. | Ectoderm | Only the 1st Cleft forms a permanent adult structure: the External Auditory Meatus (Ear Canal). Clefts 2, 3, and 4 are normally overgrown by Arch 2 and disappear. |
| Pharyngeal Arch | The bulging tissue masses between the cleft and pouch. | Mesoderm + Neural Crest | Forms the core structures: Muscles, bones, cartilage, specific cranial nerves, and arteries of the face and neck. |
| Pharyngeal Pouch | The indentations on the INSIDE of the primitive pharynx. | Endoderm | Forms crucial internal cavities and endocrine glands: Middle ear cavity, Palatine Tonsils, Thymus, and Parathyroid glands. |
SECTION 2: Arch Derivatives (What the Arches Become)
2.1 Cranial Nerves of the Pharyngeal Arches
The cranial nerves are the wiring of the head and neck. As muscles migrate away from their original arch during development, they drag their specific nerve with them. Therefore, knowing a muscle's nerve supply instantly tells you which pharyngeal arch it originated from.
| Arch | Cranial Nerve Number | Nerve Name | Main Function / Territory |
|---|---|---|---|
| Arch I | CN V | Trigeminal Nerve (Specifically V3 - Mandibular Division) |
Chewing (Muscles of Mastication), general face and jaw sensation. |
| Arch II | CN VII | Facial Nerve | Facial expression (smiling, frowning, blinking), and taste to the anterior 2/3 of the tongue. |
| Arch III | CN IX | Glossopharyngeal Nerve | Swallowing (Stylopharyngeus muscle), and general sensation + taste to the posterior 1/3 of the tongue. |
| Arch IV | CN X | Vagus Nerve (Superior Laryngeal Branch) |
Sensation to the larynx ABOVE the vocal cords, and swallowing (pharyngeal constrictors). |
| Arch VI | CN X | Vagus Nerve (Recurrent Laryngeal Branch) |
Motor control to all intrinsic muscles of the larynx (voice production) BELOW the vocal cords. |
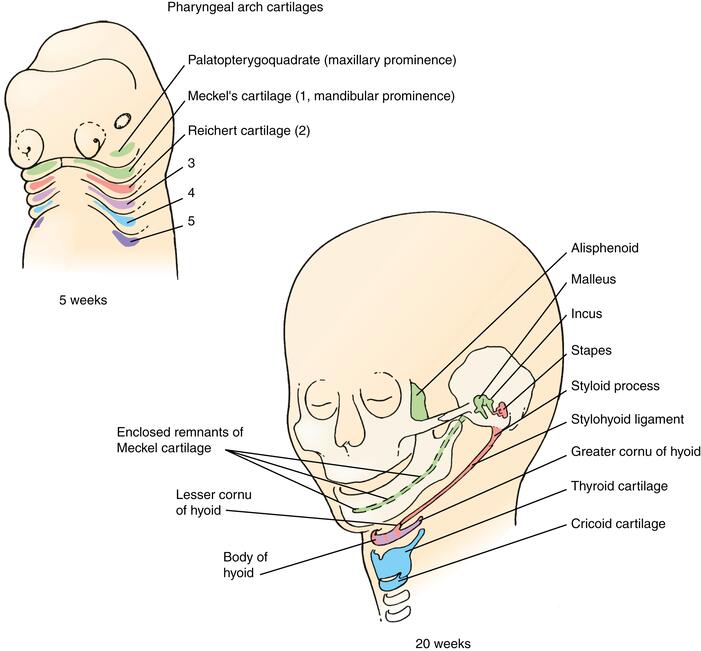
2.2 Bones & Cartilages (Skeletal Derivatives)
The cartilaginous rods within each arch give rise to the rigid structures of the jaw, middle ear, and voice box.
Meckel's Cartilage
This acts as the primary cartilage model for the lower face. However, most of Meckel's cartilage actually disappears (degenerates) and is replaced by bone via intramembranous ossification.
- Bones Formed: Mandible (lower jaw - forms around the cartilage, not from it), Maxilla (upper jaw), Zygomatic bone (cheekbone).
- Middle Ear Bones: The proximal ends of Meckel's cartilage directly ossify into the Malleus and Incus.
- Ligaments: Sphenomandibular ligament and the Anterior ligament of the malleus.
Reichert's Cartilage
Think of the "S" structures for the Second arch.
- Bones Formed: Stapes (the smallest bone in the human body, located in the middle ear), Styloid process of the temporal bone.
- Hyoid Bone Parts: Forms the Lesser horn and the Upper body of the hyoid bone.
- Ligaments: Stylohyoid ligament (connects the styloid process to the hyoid bone).
Hyoid Completion
Arch III has a very specialized, limited role in skeletal formation.
- Hyoid Bone Parts: Forms the Greater horn and the Lower body of the hyoid bone.
- Clinical Note: Because the hyoid bone is suspended in the neck and formed by the fusion of Arch II and Arch III derivatives, it is uniquely positioned to assist in swallowing and tongue movement without articulating directly with any other bone.
The Larynx (Voice Box)
Arches IV and VI fuse together to form the protective and functional cartilages of the airway. They do not form bone, only cartilage.
- Arch IV: Forms the Thyroid cartilage (the Adam's apple) and the Cricoid cartilage (the full complete ring below the thyroid).
- Arch VI: Forms the highly mobile internal cartilages that manipulate the vocal cords: Arytenoid, Corniculate, and Cuneiform cartilages.
2.3 Muscles by Arch Origin
Because each arch has its own nerve, you can group all head and neck muscles simply by tracing their nerve supply.
| Arch | Innervating Nerve | Muscles Derived from this Arch | Primary Function |
|---|---|---|---|
| Arch I | Trigeminal (CN V3) | Muscles of Mastication: Temporalis, Masseter, Medial Pterygoid, Lateral Pterygoid. Others: Mylohyoid, Anterior belly of Digastric, Tensor tympani, Tensor veli palatini. |
Chewing, elevating the floor of the mouth, tensing the eardrum (Tensor tympani), and tensing the soft palate to prevent food from entering the nose. |
| Arch II | Facial (CN VII) | Muscles of Facial Expression: Frontalis, Orbicularis oculi, Orbicularis oris, Buccinator, Platysma. Others: Stapedius, Stylohyoid, Posterior belly of Digastric. |
Smiling, blinking, kissing, keeping food between teeth (Buccinator), and dampening loud sounds in the ear (Stapedius). |
| Arch III | Glossopharyngeal (CN IX) | Stylopharyngeus (This is the ONLY muscle supplied by the Glossopharyngeal nerve). | Elevates the larynx and widens the pharynx during the act of swallowing to accommodate large food boluses. |
| Arch IV | Vagus (Superior Laryngeal branch) | Pharyngeal Constrictors (Superior, Middle, Inferior), Cricothyroid, Levator veli palatini. | Constricting the throat to swallow food. The Cricothyroid is the only intrinsic laryngeal muscle that tenses the vocal cords (raising pitch). |
| Arch VI | Vagus (Recurrent Laryngeal branch) | All intrinsic muscles of the larynx (Thyroarytenoid, lateral/posterior cricoarytenoid) EXCEPT the cricothyroid. | Voice production, opening/closing the vocal cords to breathe and speak, and airway protection during swallowing. |
Clinical Correlate: The Recurrent Laryngeal Nerve
Because the Recurrent Laryngeal Nerve (Arch VI) wraps around the aortic arch (on the left) and the subclavian artery (on the right) before traveling back up the neck, it is highly vulnerable during thyroid surgery. If a surgeon accidentally severs this nerve, all intrinsic muscles of the larynx on that side become paralyzed. The patient will suffer from severe hoarseness (voice change) and potential airway compromise.
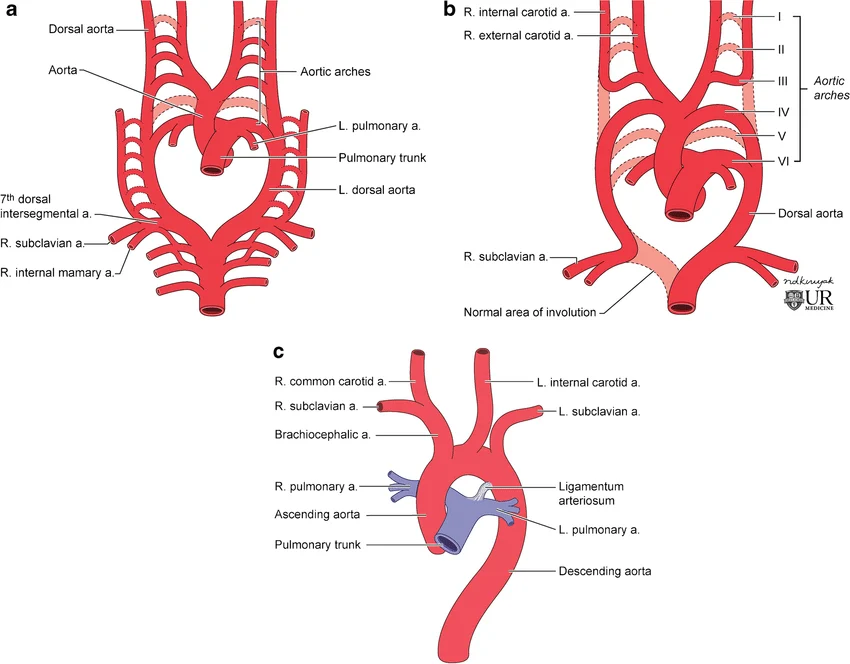
2.4 Blood Vessels: Aortic Arch Derivatives
The primitive heart pumps blood through a basket-like network of arteries within the arches. As the embryo matures, this basket is drastically remodeled.
Fate: They mostly REGRESS (disappear) in the adult.
Minor remnants: A small portion of Arch I forms the Maxillary artery. Arch II forms the tiny Stapedial artery.
Fate: Forms the primary blood supply to the head.
Becomes the Common Carotid Artery and the proximal portion of the Internal Carotid Artery.
Fate: Highly asymmetrical remodeling.
- Left Side: Forms the definitive Aortic Arch in the adult chest.
- Right Side: Forms the proximal part of the Right Subclavian Artery (supplying the right arm).
Fate: The Pulmonary system.
- Right Side: Forms the Right Pulmonary Artery.
- Left Side: Forms the Left Pulmonary Artery AND the Ductus Arteriosus.
Clinical Note: The Ductus Arteriosus allows fetal blood to bypass the lungs. After birth, it must close and become the Ligamentum Arteriosum. If it fails to close, the infant is born with a congenital heart defect known as Patent Ductus Arteriosus (PDA).
SECTION 3: Special Organs
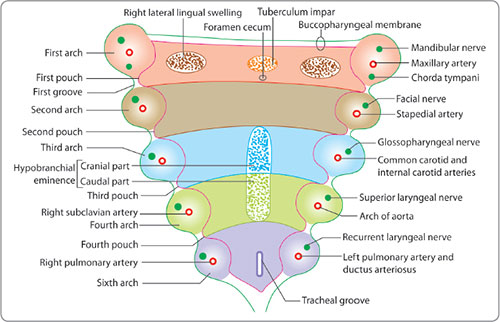
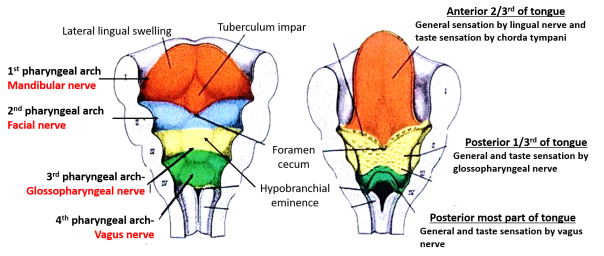
3.1 & 3.2 Tongue Development and Sensory Nerve Supply
The tongue is an incredibly complex organ because it is constructed by fusing different pharyngeal arches together. This explains why the tongue requires three different cranial nerves just to feel sensation and taste!
- Anterior 2/3 of the Tongue:
- Origin: Derives from Arch I (specifically, two lateral lingual swellings that overgrow a central bump called the tuberculum impar).
- General Sensation (Pain/Touch/Temperature): Handled by the Lingual Nerve (a branch of CN V3 - Trigeminal), perfectly matching its Arch I origin.
- Taste Sensation: Handled by the Chorda Tympani (a branch of CN VII - Facial). Mechanism: The chorda tympani "hitchhikes" along the lingual nerve to reach the front of the tongue.
- Posterior 1/3 of the Tongue:
- Origin: Derives from Arch III (a swelling called the hypobranchial eminence or copula).
- General Sensation AND Taste: Both are handled entirely by the Glossopharyngeal Nerve (CN IX), perfectly matching its Arch III origin.
- Extreme Posterior (Root/Epiglottis region):
- Origin: Derives from Arch IV.
- General Sensation AND Taste: Handled by the Vagus Nerve (CN X).
Anatomical Landmark: The border between the anterior 2/3 and the posterior 1/3 is marked by a V-shaped groove on the surface of the tongue called the Sulcus Terminalis. At the absolute center (the point of the V) is a pit called the Foramen Cecum.
3.3 Face Formation from Facial Prominences
The human face is formed by five distinct blocks of tissue (prominences) that grow inward and fuse together around the primitive mouth (stomodeum).
- Frontonasal Prominence (1): Forms the forehead, the bridge of the nose, the nasal septum, and the central part of the upper lip (the philtrum).
- Medial Nasal Prominences (from Frontonasal): Fuse together in the midline to form the central tip of the nose and the philtrum.
- Lateral Nasal Prominences: Form the sides (ala) of the nose.
- Maxillary Prominences (2 - Arch I): Form the upper cheeks, the lateral parts of the upper lip, and the upper jaw.
- Mandibular Prominences (2 - Arch I): Fuse early to form the entire lower jaw, lower lip, and chin.
Cleft Lip and Cleft Palate
Understanding facial prominences makes diagnosing congenital facial clefts highly logical:
- Cleft Lip: Occurs when the Maxillary Prominence fails to fuse with the Medial Nasal Prominence. This leaves a visible gap in the upper lip.
- Cleft Palate: Occurs later in development when the palatine shelves (internal extensions of the maxillary prominences) fail to meet and fuse in the midline inside the mouth, leaving a gap connecting the oral and nasal cavities.
3.4 Pharyngeal Pouch Derivatives (Endodermal)
The internal pouches (lined by endoderm) bud outward into the surrounding mesoderm to form critical glands and cavities.
| Pouch | Derivatives | Clinical Relevance |
|---|---|---|
| 1st Pouch | Middle ear cavity (tympanic cavity) and the Auditory (Eustachian) tube. | Defects here can cause conductive hearing loss or chronic ear infections (otitis media). |
| 2nd Pouch | Epithelial lining of the Palatine tonsil and the Tonsillar fossa. | Remnants of the 2nd pouch can abnormally persist and form deep tonsillar cysts. |
| 3rd Pouch | Thymus gland and the Inferior Parathyroid glands. | Embryonic trick: The 3rd pouch derivatives must physically migrate down the neck. They travel further down than the 4th pouch, which is why the 3rd pouch forms the inferior parathyroids. |
| 4th Pouch | Superior Parathyroid glands and the Ultimobranchial body. | The ultimobranchial body gives rise to the parafollicular C-cells of the thyroid gland, which produce the hormone calcitonin to regulate calcium. |
SECTION 4: Clinical Conditions (Developmental Failures)
When the intricate ballet of pharyngeal arch migration, fusion, or apoptosis fails, characteristic congenital syndromes arise.
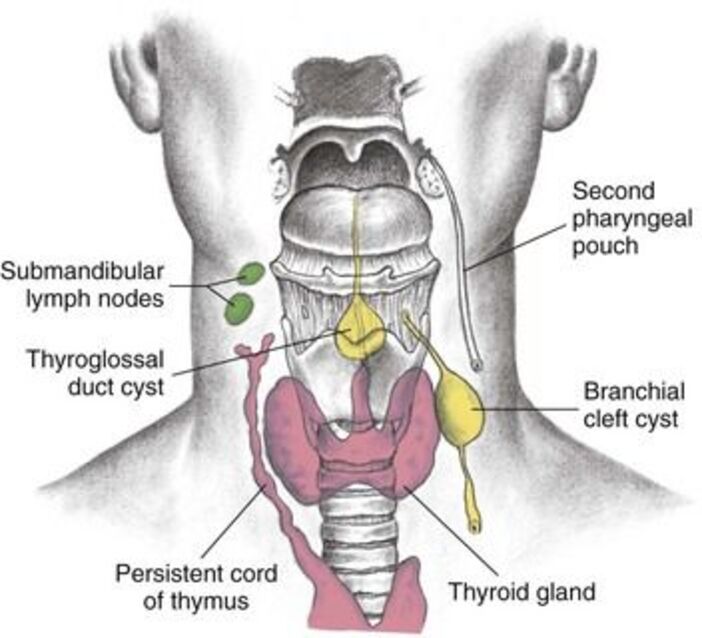
Pathophysiology: Formed from remnants of the pharyngeal clefts (usually the 2nd cleft) that fail to completely close and obliterate during development.
- Presentation: A painless, fluid-filled cystic swelling located strictly on the LATERAL (side) of the neck, usually just anterior to the sternocleidomastoid (SCM) muscle, near the angle of the mandible.
- Complications: Lined by squamous epithelium, it can easily become infected with upper respiratory pathogens, forming a painful abscess.
- Treatment: Complete surgical excision of the cyst and any associated fistulous tract.
Pathophysiology: The thyroid gland originates at the base of the tongue (at the Foramen Cecum) and must travel down the midline of the neck to its final resting place over the trachea. It leaves behind a trail called the thyroglossal duct, which normally disappears. If it persists, it fills with fluid.
- Presentation: A painless cystic swelling located strictly in the MIDLINE of the neck (often near the hyoid bone).
- Defining Clinical Sign: Because the cyst is still tethered to the base of the tongue, the cyst will visibly MOVE UPWARDS when the patient sticks their tongue out or swallows. (A branchial cyst will NOT move with tongue protrusion).
- Treatment: Sistrunk procedure (surgical removal of the cyst along with the central portion of the hyoid bone to prevent recurrence).
First Arch Syndromes
Failure of Neural Crest cells to properly migrate into the 1st Pharyngeal Arch results in severe underdevelopment of the facial skeleton.
- Treacher Collins Syndrome (Mandibulofacial Dysostosis):
- Cause: A genetic mutation (typically the TCOF1 gene) that severely impairs 1st arch development.
- Phenotype: Underdeveloped cheekbones (zygomatic hypoplasia), downward-slanting eyes, profound micrognathia (abnormally small lower jaw), severe outer ear abnormalities, cleft palate, and subsequent conductive hearing loss (due to malformed malleus/incus).
- Pierre Robin Sequence:
- Cause: Can be isolated or part of a broader syndrome (e.g., Stickler syndrome). It is termed a "sequence" because one initial defect triggers a cascade of secondary defects.
- Phenotype & Cascade: The primary defect is severe Micrognathia (small jaw). Because the jaw is so small, the tongue is forced backward and upward into the airway (Glossoptosis). The tongue physically blocks the palatine shelves from fusing during weeks 6-8, resulting in a U-shaped Cleft Palate.
- Clinical Emergency: These neonates face life-threatening airway obstruction and severe feeding difficulties immediately upon birth.
DiGeorge Syndrome (22q11.2 Deletion Syndrome)
Pathophysiology: A microdeletion on chromosome 22 leads to a catastrophic failure in the development of the 3rd and 4th Pharyngeal Pouches.
Clinical Features (The CATCH-22 Mnemonic):
- C - Cardiac defects: Aortic arch abnormalities such as Tetralogy of Fallot, Truncus Arteriosus, or Interrupted Aortic Arch.
- A - Abnormal facies: Hypertelorism (widely spaced eyes), a short philtrum, and small/low-set ears.
- T - Thymic aplasia/hypoplasia: The Thymus is completely missing or tiny. Without a thymus, T-cells cannot mature, leading to profound T-cell immunodeficiency and recurrent, life-threatening viral and fungal infections.
- C - Cleft palate: Often accompanies the syndrome.
- H - Hypocalcemia: The Parathyroid glands are missing. Without parathyroid hormone (PTH), blood calcium levels crash, leading to severe neuromuscular irritability, muscle spasms (tetany), and fatal seizures.
- 22 - Chromosome 22q11.2 microdeletion.
Developmental Delay: These patients frequently experience learning difficulties, speech problems, and psychiatric disorders later in life.
List of References
- Sadler, T. W. (2018). Langman's Medical Embryology (14th ed.). Wolters Kluwer. (Comprehensive reference for timeline, germ layer origins, and pouch derivatives).
- Moore, K. L., Persaud, T. V. N., & Torchia, M. G. (2019). The Developing Human: Clinically Oriented Embryology (11th ed.). Elsevier. (In-depth analysis of clinical conditions like DiGeorge syndrome and Pierre Robin Sequence).
- Schoenwolf, G. C., Bleyl, S. B., Brauer, P. R., & Francis-West, P. H. (2020). Larsen's Human Embryology (6th ed.). Elsevier. (Excellent illustrative context for cranial nerve and aortic arch remodeling).
- Rohen, J. W., Yokochi, C., & Lütjen-Drecoll, E. (2015). Anatomy: A Photographic Atlas (8th ed.). Schattauer. (Structural and functional muscle correlations matching arch origins).