Cavities and Passageways of the Head and Neck
A Comprehensive Master Guide for Medical Students & Clinical Practice
This exhaustive guide covers the essential anatomy, neurovascular supply, and clinical pathology of the aerodigestive tracts, skull base fossae, and fascial spaces of the head and neck. By mastering these regions, you will be deeply conversant with:
- The Nasal Cavity & Paranasal Sinuses and the pathways of deadly intracranial infections.
- The Pharyngeal & Laryngeal structures crucial for airway management and swallowing.
- The 3D boundaries and contents of the Cranial Fossae, Infratemporal Fossa, and Pterygopalatine Fossa.
- The catastrophic spread of Deep Neck Space Infections.
- The complex neurovascular intersections of the Orbit, Ear, and Cavernous Sinus.
SECTION 1: THE NASAL CAVITY AND PARANASAL SINUSES
1.1 Overview and Clinical Significance
The nasal cavity is the proximal, uppermost portion of the respiratory tract. It extends from the external nostrils (anterior nares) to the choanae (posterior nares), where it directly communicates with the nasopharynx. It is divided symmetrically into right and left halves by the nasal septum.
Crucial Functions:
- Warming and humidifying inspired air via its extensive, highly vascular mucosal surface.
- Filtering particulate matter and trapping microbes using vibrissae (hairs) and the mucociliary escalator.
- Providing the special sense of olfaction (smell).
- Acting as a resonating chamber to give the voice its characteristic tone.
The paranasal sinuses are four paired, air-filled cavities entirely encased within the bones of the skull. They communicate directly with the nasal cavity. They serve to reduce the overall weight of the skull, provide voice resonance, act as shock absorbers for the brain during facial trauma, and produce immunologic mucus.
CLINICAL PEARL: The nasal cavity possesses a rich vascularity and a direct anatomical connection to the cranial vault via the perforated cribriform plate. Severe nasal trauma can result in cerebrospinal fluid (CSF) rhinorrhea. Because of this direct highway, aggressive nasal infections can spread intracranially, resulting in devastating, fatal meningitis or brain abscesses.
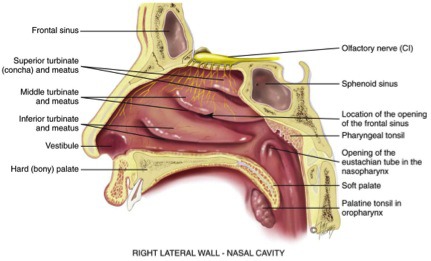
1.2 Boundaries and Bony Framework
The nasal cavity is a pyramidal space governed by four distinct walls:
- ROOF: Narrow and delicate. Formed primarily by the cribriform plate of the ethmoid bone. This is the thinnest and most clinically dangerous boundary, heavily perforated by small foramina transmitting the olfactory nerve filaments (CN I). The sphenoid sinus lies directly posterior to it, inferior to the sella turcica and pituitary gland.
- FLOOR: Smooth and concave. Formed by the palatine process of the maxilla (anterior 2/3) and the horizontal plate of the palatine bone (posterior 1/3). Together, these form the hard palate.
- MEDIAL WALL: The nasal septum (discussed below).
- LATERAL WALL: The most complex, convoluted wall. It features bony scroll-like projections called conchae (turbinates) and the air channels beneath them called meatuses. The inferior nasal concha is an independent bone, while the superior and middle conchae are mere projections of the massive ethmoid bone.
1.3 The Nasal Septum and Kiesselbach's Plexus
The nasal septum acts as the central dividing pillar. It comprises both bony and cartilaginous elements.
The septal nasal cartilage (quadrangular cartilage) forms the anterior and inferior portion. It provides the flexible structure of the nose, articulating superiorly with the perpendicular plate of the ethmoid.
The perpendicular plate of the ethmoid forms the superior-posterior aspect. The vomer forms the posterior-inferior foundation. The sphenoid crest and palatine processes lock the septum into place.
Kiesselbach's Plexus (Little's Area)
This is a massive, highly superficial vascular anastomosis located on the anterior-inferior nasal septum. It is the anatomical site for 90% of all epistaxis (nosebleeds), frequently triggered by dry air, digital trauma (nose-picking), or hypertension.
Five contributing arteries anastomose here:
- Sphenopalatine artery (Terminal branch of Maxillary a.)
- Anterior ethmoidal artery (Branch of Ophthalmic a.)
- Posterior ethmoidal artery (Branch of Ophthalmic a.)
- Superior labial artery (Branch of Facial a.)
- Greater palatine artery (Branch of Maxillary a.)
Clinical Pearl: Because this plexus receives high-pressure blood from BOTH the internal carotid system (ethmoidal arteries) and the external carotid system (facial/maxillary arteries), epistaxis can be shockingly profuse. First-line management is firm, direct mechanical pressure against the septum for 10-15 uninterrupted minutes.
1.4 Lateral Nasal Wall and Meatuses
The lateral wall maximizes surface area. The spaces beneath the conchae are the receiving drains for the sinuses and eyes.
- Inferior Concha & Meatus: The largest concha. The inferior meatus receives the nasolacrimal duct. (This is why your nose runs heavily when you cry).
- Middle Concha & Meatus: The most clinically vital space. It receives drainage from the frontal sinus, maxillary sinus, and anterior/middle ethmoidal air cells.
- Superior Concha & Meatus: Receives drainage strictly from the posterior ethmoidal air cells.
The Ostiomeatal Complex (OMC): This is the functional "choke point" of the lateral wall. It comprises the maxillary ostium, hiatus semilunaris, ethmoid bulla, and uncinate process. Because so many sinuses drain through this narrow corridor, mucosal swelling here (from allergies or colds) causes OMC obstruction—the leading cause of acute bacterial rhinosinusitis.
1.5 Paranasal Sinuses: Anatomy and Drainage
| Sinus | Anatomy & Drainage Pathway | Clinical Significance |
|---|---|---|
| Frontal Sinuses | Located in the frontal bone. Drains via the frontonasal duct into the middle meatus. Absent at birth; develops fully by puberty. | Infection can erode the anterior bone causing Pott's puffy tumor (frontal osteomyelitis), or erode posteriorly causing epidural/brain abscesses. |
| Maxillary Sinuses | The largest sinuses (~15 mL). Drains via the maxillary ostium into the hiatus semilunaris (middle meatus). | The drainage ostium is located HIGH on the medial wall, forcing it to drain completely against gravity. The floor shares a border with upper molar roots; dental infections frequently punch through to cause massive odontogenic sinusitis. |
| Ethmoid Sinuses | 3-18 honeycomb-like cells per side. Separated from the orbit only by the paper-thin lamina papyracea. Anterior drains to middle meatus; posterior to superior meatus. | Because the bone is so thin, ethmoid sinusitis is the most common cause of devastating, vision-threatening orbital cellulitis in children. |
| Sphenoid Sinuses | Within the sphenoid bone body. Drains into the sphenoethmoidal recess. Sits directly beneath the pituitary gland and beside the cavernous sinus. | Neurosurgeons use this sinus as the primary, minimally invasive surgical corridor (transsphenoidal approach) to remove pituitary tumors without opening the skull. |
1.6 Neurovascular Supply of the Nasal Cavity
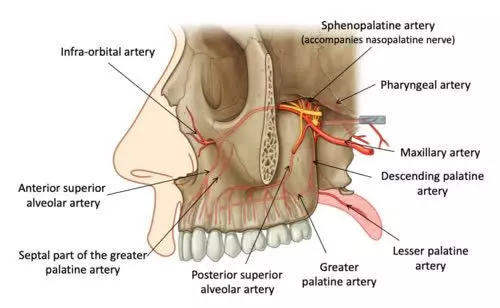
- Arterial Supply: Derived from both the ICA (anterior/posterior ethmoidal a.) and ECA (sphenopalatine a., greater palatine a., superior labial a.).
- Venous Drainage: Drains into the pterygoid plexus, facial vein, and ophthalmic veins. Danger: The facial vein is valveless and communicates directly with the cavernous sinus. Infections in the "danger area" (upper lip/nose) can spread retrogradely, causing lethal Cavernous Sinus Thrombosis.
- Sensory Innervation: Branches of V1 (anterior ethmoidal nerve) handle the front; V2 branches (nasopalatine, greater palatine, posterior lateral nasal nerves) handle the bulk of the cavity.
- Autonomic Innervation:
- Parasympathetic: From CN VII via the greater petrosal nerve & pterygopalatine ganglion. Causes profuse, watery rhinorrhea.
- Sympathetic: From superior cervical ganglion. Causes severe vasoconstriction (decongestion).
- Olfactory: CN I filaments plunge through the cribriform plate to reach the olfactory bulb.
1.7 Clinical Pathology
Epistaxis: Divided into Anterior (90%, from Kiesselbach's plexus, easily managed) and Posterior (10%, from the sphenopalatine artery/Woodruff's plexus, hidden deep in the throat, massive bleeding requiring balloon packing or surgical arterial ligation).
Rhinosinusitis: Usually Viral (70-80%). If it persists past 10 days or double-sickens, it is likely bacterial (Strep pneumoniae, H. influenzae, M. catarrhalis). In poorly controlled diabetics or immunocompromised patients, look out for Mucormycosis (a flesh-eating invasive fungus causing black necrotic eschars on the palate/nasal mucosa).
Warning: Any child with sinusitis who develops periorbital edema, proptosis (bulging eye), or restricted eye movements requires urgent CT and broad-spectrum IV antibiotics to prevent permanent blindness or death.
SECTION 2: THE PHARYNX
2.1 Overview and Functional Anatomy
The pharynx is a muscular, fibromembranous tube ~12-14 cm in length, extending continuously from the base of the skull down to C6, where it seamlessly transitions into the esophagus. It is the ultimate crossroad, serving as a common passageway for both the respiratory (air) and digestive (food/liquid) tracts.
Functions: Air conduction, food bolus propulsion, Eustachian tube pressure regulation, intense immune surveillance (Waldeyer's ring), and speech resonance.
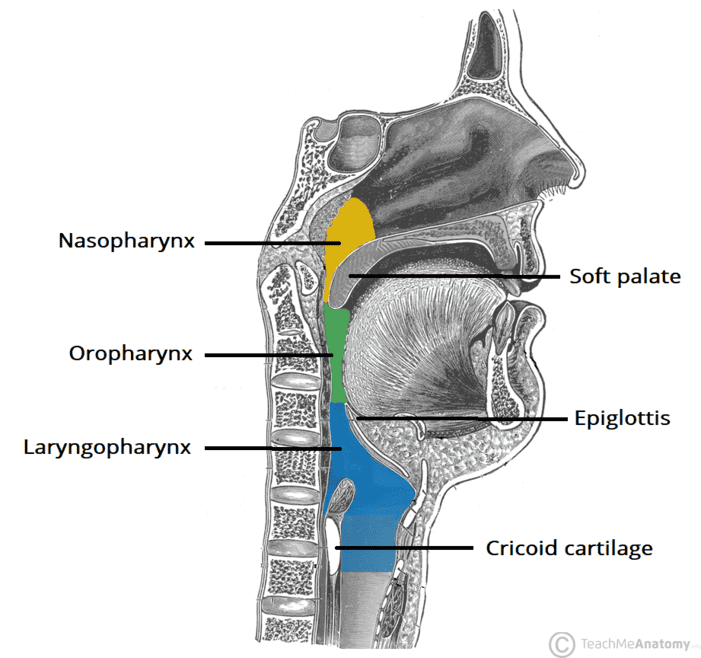
2.2 The Nasopharynx
Located directly posterior to the nasal cavity. It is strictly a respiratory passageway.
- Boundaries: Anterior = choanae; Posterior = C1 vertebra; Superior = skull base; Inferior = soft palate.
- Torus Tubarius: A firm mucosal elevation surrounding the opening of the Eustachian tube. The tensor and levator veli palatini muscles actively pull this open when you swallow to "pop" your ears.
- Pharyngeal Recess (Fossa of Rosenmüller): A deep slit-like recess just behind the torus tubarius. This is the most common anatomical origin site for Nasopharyngeal Carcinoma (NPC), a cancer heavily linked to the Epstein-Barr Virus (EBV), especially endemic in Southeast Asian populations.
- Pharyngeal Tonsil (Adenoids): A pad of immune lymphoid tissue on the roof. In children, chronic infections cause massive adenoid hypertrophy, physically blocking the airway and leading to chronic mouth-breathing, snoring, and obstructive sleep apnea.
Clinical Relevance: The pediatric Eustachian tube is anatomically shorter, wider, and much more horizontal than an adult's. Gravity does not help it drain, allowing throat bacteria to easily swim up into the middle ear, causing incredibly frequent Acute Otitis Media.
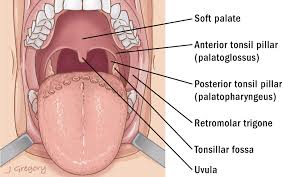
2.3 The Oropharynx
Located posterior to the oral cavity, bounded superiorly by the soft palate and inferiorly by the superior border of the epiglottis/hyoid bone.
- Palatine Tonsils: Massive, paired lymphoid tissues nestled perfectly between the palatoglossal arch (anterior muscular pillar) and the palatopharyngeal arch (posterior pillar). Their primary blood supply is the tonsillar branch of the facial artery (a major risk for hemorrhage post-tonsillectomy). Sensory innervation is via the glossopharyngeal nerve (CN IX), which explains why severe tonsillitis frequently causes referred pain to the ear.
- Waldeyer's Ring: The ultimate immune perimeter guarding the entry to the gut and lungs. Comprises the pharyngeal tonsils (top), tubal tonsils (lateral), palatine tonsils (lateral), and lingual tonsil (base of tongue).
2.4 The Laryngopharynx (Hypopharynx)
The lowest segment, extending from the hyoid bone down to the lower border of the cricoid cartilage (C6).
- Pyriform Sinus (Fossa): Paired, deep mucosal recesses on either side of the laryngeal inlet. Danger zone: Because they act as anatomical "gutters," sharp foreign bodies (like fish bones or chicken fragments) lodge here frequently. Furthermore, this area lacks early pain sensation, so hypopharyngeal squamous cell carcinomas can grow silently here for months before presenting as a massive neck mass.
- Postcricoid Region: Located on the anterior wall just above the esophagus. This region is notoriously associated with Plummer-Vinson syndrome (a classic triad of severe iron deficiency anemia, dysphagia, and esophageal webs), which carries a high risk of malignant transformation.
2.5 Pharyngeal Musculature
The pharynx is built like three overlapping flowerpots stacked inside one another (The Constrictors), flanked by three long elevator muscles.
- Superior: Originates from the pterygomandibular raphe. Forms the lateral wall of the tonsillar bed.
- Middle: Originates from the hyoid bone.
- Inferior: Originates from the thyroid/cricoid cartilages. The most inferior fibers form the Cricopharyngeus muscle (the extremely tight Upper Esophageal Sphincter that prevents air from filling your stomach).
- All three insert into the median pharyngeal raphe posteriorly and are innervated by the Vagus nerve (CN X).
- Stylopharyngeus: Elevates the pharynx to catch the food bolus. EXCEPTION RULE: This is the ONLY muscle in the entire pharynx innervated by the Glossopharyngeal nerve (CN IX).
- Salpingopharyngeus: Pulls up the pharynx and opens the Eustachian tube.
- Palatopharyngeus: Tenses the soft palate and acts as an elevator.
Anatomical Defect: Zenker's Diverticulum
There are natural gaps between the constrictor muscles to allow nerves and vessels to pass. The most famous weakness is Killian's dehiscence, a triangular weak spot perfectly situated between the oblique fibers of the inferior constrictor and the horizontal fibers of the cricopharyngeus muscle.
If the cricopharyngeus spasms and fails to relax during swallowing, extreme pressure builds up. The mucosa physically herniates backwards through Killian's triangle, creating a large, foul-smelling pouch (Zenker's Diverticulum).
Presentation: Progressive dysphagia, regurgitation of undigested food eaten days ago, severe halitosis (bad breath), and deadly aspiration pneumonia. Treated surgically via cricopharyngeal myotomy.
2.6 Innervation and Blood Supply
- Pharyngeal Plexus: A massive nerve web plastered on the lateral pharyngeal wall. Composed of CN X (Vagus - driving all motor except stylopharyngeus), CN IX (Glossopharyngeal - providing all general sensory feedback for the gag reflex), and sympathetic fibers.
- Arterial Supply: Highly robust. Principally supplied by the Ascending Pharyngeal Artery (from the external carotid), heavily assisted by facial artery branches (tonsillar, ascending palatine) and maxillary artery branches (descending palatine).
2.7 Clinical Pathology
- Pharyngitis: 70-80% is viral. If bacterial, it is classically Group A Streptococcus (Strep pyogenes). The Centor criteria (fever, tonsillar exudates, tender cervical lymphadenopathy, absence of cough) dictate whether to swab and treat with Penicillin to prevent Rheumatic Fever.
- Peritonsillar Abscess (Quinsy): A massive bacterial pus collection trapped between the tonsillar capsule and the superior constrictor muscle. The swelling pushes the entire tonsil medially.
Classic Features: Unbearable unilateral throat pain, extreme trismus (lockjaw due to pterygoid muscle spasm), a muffled "hot potato" voice, and the classic sign: uvular deviation away from the affected side. Requires immediate needle aspiration or surgical I&D. - Retropharyngeal Abscess: Infection trapped behind the pharynx. Highly common in children <5 years due to lymph nodes that later atrophy.
Classic Features: High fever, stiff neck (torticollis), drooling, and stridor. The expanding abscess pushes the posterior pharyngeal wall forward, physically choking the child. Requires surgical drainage in the OR. - Pharyngeal Tumors: Overwhelmingly Squamous Cell Carcinoma (SCC). Today, Oropharyngeal SCC is increasingly caused by HPV-16 rather than tobacco, which thankfully carries a much better overall prognosis and responds beautifully to radiation.
SECTION 3: THE ORAL CAVITY
3.1 Overview and Divisions
The oral cavity is the muscular, dynamic beginning of the digestive tract. It handles mastication (chewing), salivary digestion, speech articulation, and complex taste. It is strictly divided into two zones:
- Oral Vestibule: The horseshoe-shaped, narrow slit located between the inner lips/cheeks and the outer surface of the teeth and gums. (This is where you place a toothbrush to brush the outer teeth).
- Oral Cavity Proper: The massive central cavern located entirely internal to the dental arches. It houses the tongue, the hard/soft palate, and the floor of the mouth.
3.2 The Oral Vestibule
- The Lips: Governed by the powerful, circular orbicularis oris muscle (CN VII). The Vermilion border (the red part of the lip) is intensely vascular but completely lacks sweat and sebaceous glands, making it highly prone to drying and cracking.
- The Cheeks: Formed almost entirely by the buccinator muscle (CN VII). Its job is not to move the jaw, but to forcefully compress the cheek inward against the teeth during chewing, preventing food from falling into the vestibule.
- Labial Frenula: Tough midline mucosal tethers holding the lips to the gums. An overly thick maxillary frenulum physically wedges the front teeth apart, causing a gap called a diastema.
Clinical Pearl: The massive parotid gland produces saliva, but it must dump it into the mouth. It utilizes the Parotid duct (Stensen's duct), which pierces straight through the buccinator muscle and opens visibly into the oral vestibule directly opposite the upper second molar.
3.3 The Oral Cavity Proper
- Hard Palate: The rigid bony roof, formed by the maxillary palatine processes and palatine bones. Features the incisive foramen (transmitting the nasopalatine nerve) and greater palatine foramen.
- Soft Palate: A highly mobile, muscular flap hanging off the back of the hard palate. During swallowing, its muscles (tensor/levator veli palatini) rip it sharply upwards, tightly sealing off the nasopharynx so food doesn't shoot out of your nose.
- Floor of the Mouth: A muscular hammock formed entirely by the paired mylohyoid muscles. It supports the heavy tongue and houses the deep submandibular/sublingual salivary glands.
3.4 The Tongue: Anatomy and Innervation
The tongue is a massive muscular hydrostat, divided into an anterior 2/3 (oral) and posterior 1/3 (pharyngeal) by the V-shaped sulcus terminalis.
Move the tongue as an entire unit (In/Out/Up/Down).
- Genioglossus: The "Lifesaver Muscle". It strongly protrudes the tongue forward out of the mouth. If a patient is deeply unconscious, this muscle relaxes, allowing the heavy tongue to fall backward and suffocate them. ("Genioglossus advances the tongue").
- Hyoglossus: Depresses and flattens the tongue.
- Styloglossus: Elevates and aggressively retracts the tongue back for swallowing.
- Palatoglossus: Pulls the back of the tongue up. Exception: Innervated by CN X (Vagus), while all others are CN XII.
Alter the physical shape of the tongue (Rolling, Curling, Flattening). Comprises the superior/inferior longitudinal, transverse, and vertical fibers. All are innervated by the Hypoglossal Nerve (CN XII).
Neurological Rules of the Tongue
- Motor Control: Entirely Hypoglossal Nerve (CN XII) (except palatoglossus = Vagus X).
- Anterior 2/3 Sensation: General touch/pain/heat = Lingual nerve (V3). Special Taste = Chorda tympani (CN VII).
- Posterior 1/3 Sensation: Both general touch and special taste = Glossopharyngeal nerve (CN IX).
- CN XII Palsy Presentation: If a patient's right CN XII is severed (e.g., by a carotid artery dissection or tumor), the right side of the tongue becomes paralyzed and atrophies. When asked to stick their tongue straight out, the healthy left genioglossus pushes unopposed, causing the tongue to violently deviate TOWARD the paralyzed side ("The tongue licks the wound").
3.5 Salivary Glands and Ducts
- Parotid Gland: The largest gland, tucked in the retromandibular fossa. Secretes via Stensen's duct. Innervated by parasympathetics from CN IX (via the otic ganglion/auriculotemporal nerve). Clinical: The Facial Nerve (CN VII) physically runs straight through the middle of the parotid gland. Parotid tumors (like pleomorphic adenomas) or parotid surgery carry a massive risk of causing permanent facial paralysis.
- Submandibular Gland: Wraps around the posterior edge of the mylohyoid muscle. Secretes via Wharton's duct, which opens under the tongue at the sublingual caruncle. Innervated by CN VII (via the submandibular ganglion). Clinical: Because Wharton's duct runs uphill against gravity and the saliva here is thick and alkaline, it is the most common site for excruciating sialolithiasis (salivary stones).
- Sublingual Gland: Smallest, lying in the floor of the mouth. Secretes via dozens of tiny ducts of Rivinus. Clinical: A blocked sublingual duct causes a massive, painless, frog-belly-like mucosal cyst under the tongue called a Ranula.
3.6 Teeth and Palate
Humans possess 20 deciduous (baby) teeth and 32 permanent teeth (incisors for cutting, canines for tearing, premolars/molars for crushing). The upper maxillary teeth are wired directly to the Superior Alveolar Nerves (V2). The lower mandibular teeth are wired to the thick Inferior Alveolar Nerve (V3).
Clinical Relevance: The roots of the lower 2nd and 3rd molars dip beneath the mylohyoid muscle line. Severe dental decay here will burst out of the bone and immediately flood the submandibular fascial space with pus, causing Ludwig's Angina.
3.7 Clinical Pathology
- Oral Cancer: 90% are aggressive Squamous Cell Carcinomas (SCC). Risk factors: Heavy tobacco, alcohol, betel nut chewing (Asia), and HPV. Usually presents as a painless, non-healing ulcer or a thick white plaque (leukoplakia) on the lateral tongue or floor of the mouth.
- Oral Candidiasis (Thrush): An opportunistic overgrowth of Candida albicans fungus. Presents as thick, white, cottage-cheese-like plaques that CAN be scraped off, revealing a raw, bleeding, erythematous base beneath. Seen in HIV/AIDS, inhaled steroid users, and diabetics.
- Aphthous Ulcers (Canker Sores): Excruciatingly painful, shallow, recurrent mucosal ulcers with a grey/yellow base and a bright red inflammatory halo. Linked to stress, IBD, and nutritional deficiencies.
Life-Threatening Emergency: Ludwig's Angina
This is a terrifying, rapidly spreading, bilateral cellulitis of the floor of the mouth and neck spaces. It is almost always polymicrobial, originating from an infected lower molar.
The patient presents with massive submandibular swelling (a tough, woody "bull neck" appearance). As the pus expands, it physically pushes the floor of the mouth and the entire tongue straight up and backward against the roof of the mouth, completely occluding the airway.
Features: Severe drooling (cannot swallow), stridor, extreme distress.
Management: Immediate airway protection (awake fiberoptic intubation or emergent surgical tracheostomy), massive IV broad-spectrum antibiotics, and surgical decompression.
SECTION 4: THE LARYNX AND AIRWAY PASSAGEWAYS
4.1 Overview and Functional Significance
The larynx (voice box) is a complex, cartilaginous tube located in the anterior neck spanning vertebrae C3 to C6. It connects the pharynx above to the trachea below.
- 1. Airway Protection: The absolute most critical function. It acts as an impenetrable valve, closing the glottis during swallowing to prevent food and liquid from pouring into the lungs (aspiration).
- 2. Phonation: Produces highly refined sound through the rapid vibration of the taut vocal folds.
- 3. Respiratory Regulation: Controls airflow resistance and allows for the Valsalva maneuver (building immense intra-abdominal pressure for lifting, coughing, or defecation by locking the vocal cords shut).
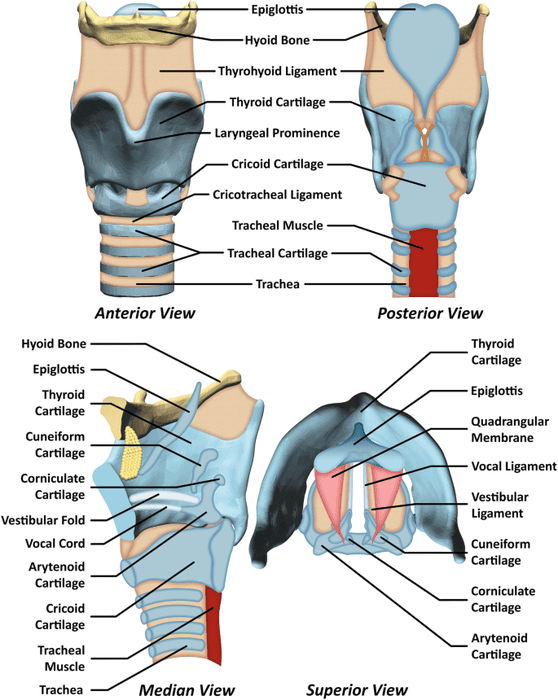
4.2 Laryngeal Framework: Cartilages and Joints
- Thyroid Cartilage: The massive shield. Two wide laminae meet anteriorly to form the laryngeal prominence (Adam's apple). It hangs from the hyoid bone via the thyrohyoid membrane (which is pierced by the internal laryngeal nerve).
- Cricoid Cartilage: The structural foundation. It is the ONLY completely solid, unbroken ring of cartilage in the entire human respiratory tract. Shaped like a signet ring, it sits at C6.
- Epiglottis: A highly flexible, leaf-shaped flap of elastic cartilage. During swallowing, the entire larynx violently jerks upward, forcing the epiglottis to snap backward like a lid, perfectly covering the laryngeal inlet.
- Arytenoid Cartilages: Pyramidal shaped, sitting on top of the posterior cricoid lamina. These are the mechanical levers of the voice. They have a vocal process pointing forward (where the vocal cords attach) and a muscular process pointing outward (where the muscles attach to pull the cords open/shut).
- Corniculate & Cuneiform: Tiny cartilages buried in the aryepiglottic folds for support.
- Cricothyroid Joint: A synovial joint that allows the massive thyroid cartilage to tilt forward like a visor. This stretches and tightens the vocal cords, raising the pitch of the voice.
4.3 Laryngeal Cavity: Vestibule, Ventricle, and Glottis
- Supraglottis (Vestibule): The entryway, stretching down to the false vocal cords (vestibular folds).
- Glottis: The precise space occurring exactly between the true vocal folds. The true vocal folds contain the tough vocal ligament and the vocalis muscle. Air violently rushing through this microscopic gap causes phonation. The rima glottidis is the absolute narrowest point of the adult airway.
- Subglottis: The smooth, expanding space below the vocal folds leading straight into the trachea. Clinical note: In infants and children under 10, the cricoid cartilage ring is completely inflexible and is the narrowest point of their airway, making them highly susceptible to fatal subglottic stenosis after prolonged intubation.
4.4 Intrinsic Laryngeal Muscles
These muscles manipulate the arytenoid cartilages to open, close, and tighten the vocal cords.
THE GOLDEN RULE: Every single intrinsic muscle is innervated by the Recurrent Laryngeal Nerve (RLN), EXCEPT for one.
| Muscle | Action on Vocal Cords | Innervation |
|---|---|---|
| Posterior Cricoarytenoid (PCA) | ABDUCTS (Opens) the vocal folds. This is the ultimate safety muscle. It is the ONLY muscle capable of opening the airway to let you breathe. | Recurrent Laryngeal N. (RLN) |
| Lateral Cricoarytenoid | Adducts (Closes) the vocal folds. Closes the airway for swallowing or whispering. | Recurrent Laryngeal N. (RLN) |
| Transverse & Oblique Arytenoids | Adducts and tightly squeezes the arytenoid cartilages together. | Recurrent Laryngeal N. (RLN) |
| Thyroarytenoid | Relaxes and dramatically shortens the vocal folds, dropping the vocal pitch into a deep register. | Recurrent Laryngeal N. (RLN) |
| Cricothyroid | Tenses, stretches, and brutally elongates the vocal folds, driving the voice into a high-pitched scream. | EXTERNAL LARYNGEAL NERVE (Exception) |
Clinical Pearl: If a patient suffers a bilateral Recurrent Laryngeal Nerve (RLN) palsy, the Posterior Cricoarytenoid muscles are paralyzed. The vocal folds become locked in a fixed, adducted (closed) paramedian position. The patient will instantly suffocate and require a surgical tracheostomy. This is why aggressive thyroid cancer surgery carries such a terrifying risk of airway compromise.
4.5 Extrinsic Laryngeal Muscles
These large strap muscles move the entire larynx up and down within the neck during swallowing and singing.
- Elevators (Suprahyoid muscles): Digastric, stylohyoid, mylohyoid, geniohyoid. They aggressively yank the larynx up under the tongue to protect it while swallowing food.
- Depressors (Infrahyoid muscles): Sternohyoid, sternothyroid, omohyoid. Innervated by the ansa cervicalis (C1-C3). They pull the larynx back down after swallowing to resume breathing.
4.6 Innervation: Superior and Recurrent Laryngeal Nerves
Both are branches of the Vagus Nerve (CN X), but they take wildly different paths.
- Superior Laryngeal Nerve (SLN): Drops directly down the neck.
- Internal Laryngeal Branch: Purely Sensory. Pierces the thyrohyoid membrane. Provides all cough-reflex sensation to the larynx ABOVE the vocal cords.
- External Laryngeal Branch: Purely Motor. Drives the cricothyroid muscle (for high pitch).
Surgical Risk: Lies dangerously close to the superior thyroid artery. If cut during a thyroidectomy, the patient's voice becomes deeply monotonous, weak, and fatigues easily because they can no longer tense their cords.
- Recurrent Laryngeal Nerve (RLN):
- Right RLN: Loops under the right subclavian artery, then climbs up the neck in the tracheoesophageal groove.
- Left RLN: Plunges deep into the chest, loops directly under the massive Aortic Arch (near the ligamentum arteriosum), and then climbs all the way back up the neck.
- Function: Provides all motor control (except cricothyroid) and all sensation BELOW the vocal folds.
WARNING: The Left RLN Vulnerability
Because the left recurrent laryngeal nerve dives deep into the mediastinum, it is significantly longer and exponentially more vulnerable than the right. A patient presenting with a sudden, unexplained hoarse, breathy voice may not have a throat problem at all. They could have an expanding Aortic Aneurysm, massive mediastinal lymphadenopathy, or an aggressive apical Lung Cancer (Pancoast tumor) physically crushing the left RLN deep in their chest.
4.7 Blood Supply and Lymphatic Drainage
- Superior Laryngeal Artery: A branch of the superior thyroid artery (ECA). Runs with the internal laryngeal nerve to supply the upper half.
- Inferior Laryngeal Artery: A branch of the inferior thyroid artery (Thyrocervical trunk). Runs with the RLN to supply the lower half.
- Lymphatics: Supraglottic tumors spread aggressively to upper deep cervical nodes. Glottic tumors rarely spread to nodes early on because the true vocal cords have virtually zero lymphatic drainage (a major reason glottic cancers have a high cure rate if caught early).
4.8 Clinical Pathology
- Acute Epiglottitis: Rapid, massive, fatal swelling of the epiglottis. Historically caused by H. influenzae type B (now rare due to Hib vaccine; now driven by Strep/Staph). Presents with the toxic "4 Ds": Dysphagia, Dysphonia, Drooling, and Distress. X-ray shows the "Thumbprint sign."
- Croup (Laryngotracheobronchitis): A parainfluenza viral infection causing intense subglottic edema in toddlers. Presents with a terrifying "barking seal" cough and inspiratory stridor. X-ray shows the "Steeple sign."
- Anaphylaxis: Massive histamine release causes instant angioedema (swelling) of the larynx. Requires immediate IM Epinephrine injection to survive.
- Laryngeal SCC: 95% of laryngeal cancers are Squamous Cell Carcinomas. Heavily driven by a lifetime of smoking and alcohol abuse (a synergistic, deadly combo). Glottic tumors sit on the vocal cords, altering their vibration immediately, causing early hoarseness (excellent prognosis). Supraglottic tumors do not alter the voice until they are massive and have spread to lymph nodes (poor prognosis).
- Vocal Cord Nodules: Benign, callous-like fibrotic lesions caused by severe vocal abuse (screaming, poor singing technique). Always present bilaterally exactly at the junction of the anterior 1/3 and posterior 2/3 of the cords ("Singer's nodules").
SECTION 5: CRANIAL FOSSAE AND CLINICAL DANGER ZONES
The cranial base is the rugged, perforated floor of the skull. A thorough understanding of its geography is essential for neurosurgery, ENT, and trauma medicine.
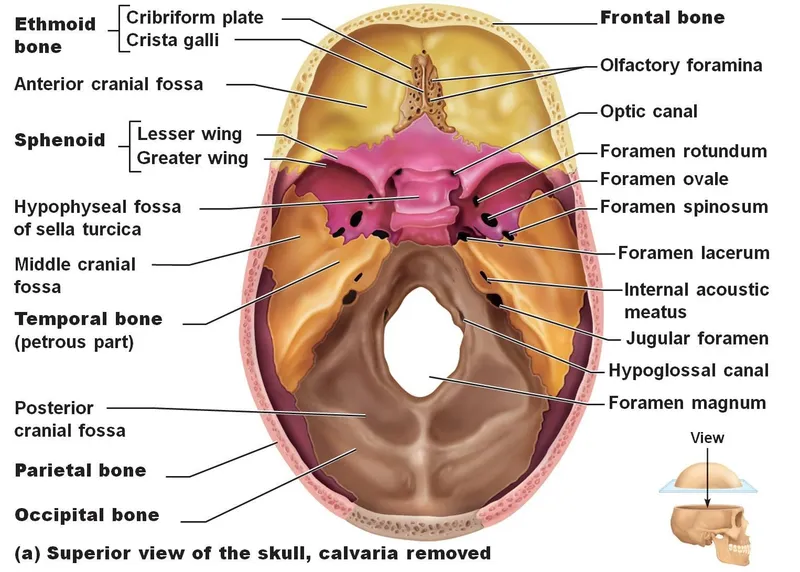
5.1 The Anterior Cranial Fossa
The highest, shallowest shelf. Houses the frontal lobes (personality, executive function) and olfactory bulbs.
- Boundaries: Frontal bone (anteriorly), lesser wing of the sphenoid and anterior clinoid processes (posteriorly).
- Foramina:
- Cribriform plate of ethmoid: Transmits delicate olfactory nerve filaments (CN I).
- Foramen cecum: A tiny blind hole transmitting a nasal emissary vein to the superior sagittal sinus.
- Clinical Relevance: The cribriform plate is terrifyingly thin. A violent blow to the face or an unrestrained car accident can fracture it, shearing the olfactory nerves (permanent anosmia) and tearing the dura mater. CSF leaks out of the nose (CSF rhinorrhea), and bacteria from the nose travel up into the brain, causing lethal bacterial meningitis.
5.2 The Middle Cranial Fossa
A deep, butterfly-shaped basin formed by the sphenoid and temporal bones. It cradles the temporal lobes (memory, hearing) and the entire pituitary apparatus.
- Central Part (Sella Turcica): A Turkish saddle-shaped depression housing the pituitary gland (hypophysis). The optic chiasm sits in a groove just anterior to it.
- Foramina and Exact Contents:
- Optic Canal: Optic nerve (CN II) and Ophthalmic artery.
- Superior Orbital Fissure: The great neurovascular highway to the eye. Contains CN III, IV, V1, VI, and superior ophthalmic veins.
- Foramen Rotundum: Maxillary nerve (V2).
- Foramen Ovale: Mandibular nerve (V3), accessory meningeal a., lesser petrosal nerve.
- Foramen Spinosum: Middle meningeal artery (MMA). Clinical: A fracture of the temporal bone (pterion) lacerates the MMA, causing a rapidly expanding, fatal Epidural Hematoma.
- Foramen Lacerum: Plugged with cartilage. The internal carotid artery slides OVER it.
- Carotid Canal: Internal carotid artery and its sympathetic nerve wrapper.
5.3 The Posterior Cranial Fossa
The largest, deepest, and most dangerous fossa. It houses the brainstem (pons, medulla) and the cerebellum.
- Foramina:
- Foramen Magnum: The massive central hole. Transmits the spinal cord/medulla, vertebral arteries, meninges, and the spinal root of the accessory nerve (CN XI).
- Internal Acoustic Meatus: CN VII (Facial), CN VIII (Vestibulocochlear), and labyrinthine artery.
- Jugular Foramen: CN IX, X, XI, and the internal jugular vein.
- Hypoglossal Canal: CN XII.
WARNING: Tonsillar Herniation (Coning)
The posterior fossa is a rigid, sealed vault. If a patient develops an expanding mass here (cerebellar tumor or acute hemorrhage), the intracranial pressure skyrockets. The brain has nowhere to go but down. The pressure violently forces the cerebellar tonsils down through the foramen magnum. This structurally crushes the medulla oblongata, instantly destroying the respiratory and cardiac centers, leading to sudden death if not emergently decompressed via craniotomy.
5.4 The Cavernous Sinus
These are paired, blood-filled venous labyrinths flanking the pituitary gland. They receive blood from the eyes and face.
- Contents in the Lateral Wall (Top to Bottom): Oculomotor (III), Trochlear (IV), Ophthalmic (V1), Maxillary (V2).
- Contents swimming directly IN the venous blood: The massive Internal Carotid Artery and the tiny Abducens Nerve (CN VI) hugging its inferolateral side.
5.5 The Danger Area of the Face
The "danger triangle" stretches from the bridge of the nose down to the corners of the mouth.
Why is it lethal? The facial veins draining this area are completely VALVELESS. If you pop an infected pimple or suffer a staph infection on your upper lip, the pressure forces the highly virulent bacteria to travel backward (retrograde) through the superior ophthalmic veins deep into the skull, creating a massive, septic clot inside the Cavernous Sinus.
Cavernous Sinus Thrombosis Presentation: Unbearable headache, massive bulging of the eye (proptosis), extreme conjunctival swelling (chemosis), and "painful ophthalmoplegia" (paralysis of all eye muscles). CN VI is affected FIRST because it floats unprotected in the blood pool, leading to an immediate inability to look outward (lateral gaze palsy). Requires massive IV antibiotics to survive.
5.6 Clinical Pathology summary of Skull Base Fractures
- Anterior fossa fracture: Raccoon eyes (bilateral black eyes), anosmia, CSF dripping from nose.
- Middle fossa fracture: Battle's sign (massive bruising behind the ear over the mastoid), CSF leaking from the ear, immediate facial paralysis (CN VII sheared in the temporal bone), and profound deafness/vertigo (CN VIII sheared).
- Meningitis Risk: Any skull base fracture carrying a CSF leak is an open highway for nasal/ear bacteria to flood the brain, constituting a neurosurgical emergency.
SECTION 6: FASCIAL SPACES OF THE HEAD AND NECK
The neck is organized into distinct, tough fascial tubes. These fascial layers form a smooth, friction-free environment for muscles to slide during swallowing and neck turning. However, pathologically, they create trapped "potential spaces" that act as superhighways, dictating exactly where massive bacterial infections will spread.
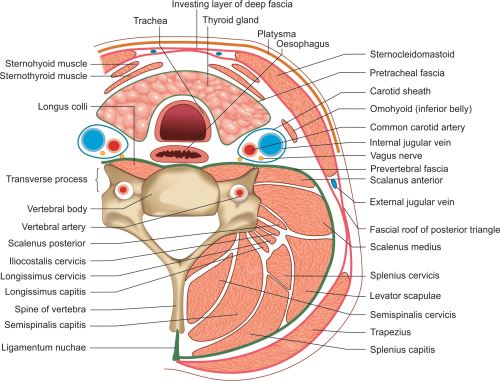
6.1 Overview of Cervical Fascia
- Superficial Cervical Fascia: Loose fat containing the paper-thin platysma muscle and superficial veins/nerves.
- Deep Cervical Fascia (Three Layers):
- 1. Investing Fascia: The outermost heavy wrapper. Completely encircles the neck, splitting to tightly enclose the sternocleidomastoid and trapezius muscles.
- 2. Pretracheal Fascia: The visceral wrapper in the anterior neck. Encloses the trachea, esophagus, and the entire thyroid gland. (This is why the thyroid gland moves up and down when a patient swallows).
- 3. Prevertebral Fascia: The tough posterior wrapper. Completely covers the cervical spine and deep back muscles. Crucially, it extends uninterrupted from the base of the skull all the way down into the deep chest (T3).
- The Carotid Sheath: Formed by contributions from all three layers. A dense tubular sheath containing the Internal Jugular Vein, Common/Internal Carotid Artery, and Vagus Nerve (CN X).
6.2 The Submandibular Space
Located under the jaw, strictly divided by the mylohyoid muscle sling.
- Submandibular Space (Proper): Below the mylohyoid. Contains the superficial bulk of the submandibular gland, facial artery, and intense lymph node clusters.
- Sublingual Space: Above the mylohyoid, sitting directly under the tongue mucosa. Contains the sublingual gland and lingual nerve.
- Clinical: Infection of the lower molars blows through the thin medial cortex of the mandible, instantly flooding both spaces with necrotic pus, causing the deadly Ludwig's angina (massive bilateral swelling pushing the tongue backward to occlude the airway).
6.3 The Parapharyngeal Space
An inverted pyramid-shaped void lateral to the pharynx. It is physically split in half by the styloid process and its attached muscles.
- Prestyloid Compartment: Anterior. Contains fat, the internal maxillary artery, and trigeminal nerve branches. Infection here causes severe trismus (lockjaw) because it inflames the adjacent medial pterygoid muscle.
- Poststyloid Compartment: Posterior. A highly critical area housing the entire Carotid Sheath (ICA, IJV, CN IX, X, XI, XII). A raging infection here will physically erode the wall of the carotid artery (causing massive fatal hemorrhage into the throat) or cause a septic clot in the jugular vein (Lemierre's syndrome).
6.4 The Retropharyngeal Space
Located directly between the back of the pharynx (buccopharyngeal fascia) and the prevertebral fascia. It contains fat and lymph nodes that usually atrophy by age 5.
Clinical Relevance: This is the most dangerous space in the neck. It is a completely open highway extending from the skull base straight down into the chest. A Retropharyngeal Abscess (from a child's strep throat or an adult swallowing a sharp fish bone that pierces the throat) will utilize gravity to spread massive amounts of pus straight down into the chest cavity, causing an invariably fatal, rotting acute mediastinitis.
6.5 The Prevertebral Space
Located posterior to the prevertebral fascia, directly resting against the bones of the cervical spine.
Clinical: Infections here are usually cold abscesses resulting from spinal tuberculosis (Pott's disease) or vertebral osteomyelitis. The bulging pus sac can push so far forward that it compresses the airway or crushes the sympathetic chain (causing Horner's syndrome).
6.6 Clinical Pathology: Deep Neck Space Infections
These are terrifying surgical emergencies. They do not remain localized; they rapidly melt through fascial planes.
- Sources: 90% arise from untreated dental decay, tonsillitis, or penetrating trauma (swallowing a chicken bone).
- Pathogens: Highly aggressive, rotting polymicrobial swarms (Streptococcus, MRSA, and highly destructive foul-smelling anaerobes like Fusobacterium and Prevotella).
- Clinical Features: High fever, severe neck pain, profound difficulty swallowing (dysphagia) or agonizing pain upon swallowing (odynophagia), uncontrolled drooling, severe trismus, and inspiratory stridor.
- Management Workflow:
- Secure the Airway: The absolute first priority. The swollen neck anatomy makes traditional intubation nearly impossible; an awake fiberoptic intubation or immediate surgical tracheostomy is often required to save the patient's life.
- Aggressive Antibiotics: Massive IV doses covering both aerobes and heavy anaerobes (e.g., Ampicillin-sulbactam, Piperacillin-tazobactam).
- CT Imaging with Contrast: To map the exact location of the pus loculations.
- Wide Surgical Drainage: The neck is sliced open externally or intra-orally to physically evacuate the gallons of pus and necrotic tissue. Remove the infected tooth or tonsil that started the fire.
SECTION 7: THE EAR AND TEMPORAL BONE PASSAGEWAYS
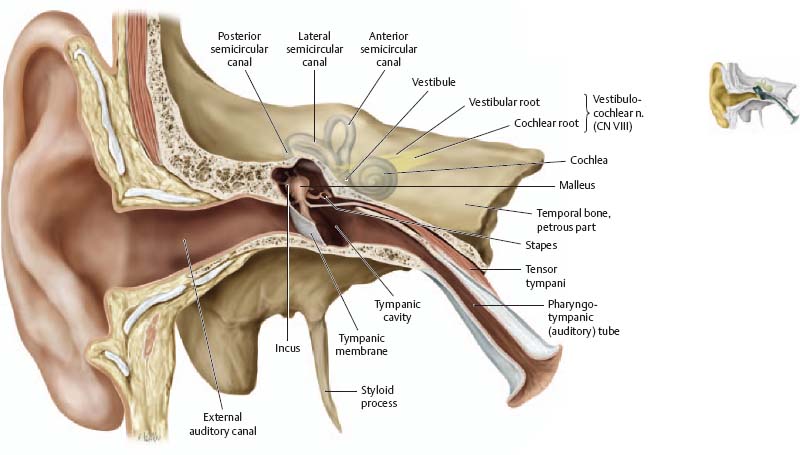
7.1 External Ear and External Auditory Canal
The acoustic funnel. The Auricle (pinna) is composed of highly malleable elastic cartilage.
The External Auditory Canal is an S-shaped tube (~3 cm). The outer 1/3 is cartilage lined with ceruminous glands (producing protective earwax) and thick hairs to trap bugs. The inner 2/3 is solid bone.
Clinical Pearl: The deep posterior-inferior floor of the ear canal is innervated directly by Arnold's nerve, a sensitive branch of the Vagus Nerve (CN X). Jamming a Q-tip or an otoscope too deep into the ear can trigger a massive vagal reflex, instantly dropping the patient's heart rate (bradycardia) and causing them to pass out (vasovagal syncope) or violently cough.
7.2 Middle Ear Cavity (Tympanic Cavity)
A tiny, 6-sided air-filled room blasted into the dense petrous temporal bone, designed to mechanically amplify sound waves.
- Roof: Tegmen tympani (a paper-thin plate of bone separating the ear from the brain's temporal lobe). Chronic ear infections can erode this, dumping pus directly into the cranial vault, causing deadly brain abscesses.
- Floor: Jugular wall (a thin plate separating the ear from the massive jugular vein).
- Anterior Wall: Carotid wall (the internal carotid artery pulses right next to it) and the opening of the Eustachian tube.
- Posterior Wall: Mastoid wall (has a hole called the aditus ad antrum, leading straight into the mastoid air cells).
- Medial Wall: The dense wall of the inner ear, featuring the oval and round windows.
- Lateral Wall: The vibrating Tympanic Membrane (eardrum).
Contents: The ossicles (Malleus, Incus, Stapes). To protect the fragile inner ear from deafeningly loud noises, two tiny muscles act as shock absorbers: The Tensor Tympani (V3) locks the malleus, and the Stapedius (CN VII) violently yanks the stapes away from the oval window. (Paralysis of CN VII causes hyperacusis—normal sounds become agonizingly loud).
7.3 Mastoid Air Cells
A honeycomb of air pockets inside the mastoid bone.
Clinical Relevance: Mastoiditis. When acute otitis media goes untreated, the pus fills the middle ear, overflows through the posterior wall (aditus ad antrum), and infects the mastoid bone. The child presents with a high fever, agonizing pain, and a massive, swollen red lump behind the ear that physically pushes the auricle forward. It can rapidly melt through the bone to cause meningitis or facial nerve paralysis.
7.4 Internal Auditory Meatus and Inner Ear
- Internal Auditory Meatus: The bony tunnel carrying CN VII, CN VIII, and the labyrinthine artery from the brainstem to the ear. Acoustic Neuroma (Vestibular Schwannoma) is a slow-growing, benign tumor of CN VIII wrapping around this canal. As it expands, it crushes the nerve, causing unilateral, permanent sensorineural hearing loss, roaring tinnitus, and severe vertigo. As it grows larger, it crushes the adjacent Facial nerve, causing facial paralysis.
- Inner Ear (Labyrinth): Houses the Cochlea (the snail-shaped organ of hearing) and the Vestibular Apparatus (semicircular canals and utricle/saccule, governing 3D spatial balance and acceleration).
7.5 Eustachian Tube (Pharyngotympanic Tube)
A 4 cm muscular tube connecting the middle ear directly to the nasopharynx. Its job is to equalize atmospheric pressure (so your eardrum doesn't blow out on an airplane) and drain normal middle-ear mucus down into the throat.
It is actively yanked open by the Tensor veli palatini (V3) and Levator veli palatini (X) when you swallow or yawn.
Clinical Pearl: Eustachian tube dysfunction (from allergy swelling) traps air in the middle ear. The oxygen is absorbed, creating a vacuum that sucks fluid out of the tissues, filling the ear with thick, sterile glue-like fluid ("Glue ear" / Otitis Media with Effusion), causing massive conductive hearing loss in toddlers.
7.6 Clinical Pathology: Otitis Media and Complications
- Acute Otitis Media (AOM): A furious, pus-filled bacterial infection (Strep pneumoniae, H. influenzae, M. catarrhalis) trapped behind the eardrum. The eardrum bulges outward, turns furious red, and is incredibly painful.
- Cholesteatoma: A destructive, expanding cyst made of trapped, rotting, keratinizing squamous skin cells. It acts like a slow-moving tumor, chemically eroding the delicate ossicles (causing deafness) and melting through the bony facial canal or inner ear.
- Gradenigo's Syndrome: The infection tracks deep into the petrous apex of the skull, causing severe ear pain, crushing the Abducens nerve (CN VI palsy - cannot look outward), and causing intense retro-orbital eye pain.
SECTION 8: THE ORBIT AND OPTIC PATHWAY
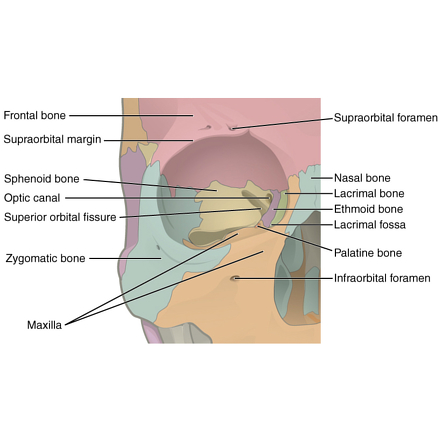
8.1 Bony Orbit and Foramina
A rigid, protective, pyramid-shaped bony vault made of 7 fused bones.
- Roof: Frontal bone. Separates the eye from the brain.
- Floor: Maxilla. Forms the roof of the maxillary sinus.
- Medial Wall: Formed mostly by the Lamina Papyracea of the ethmoid bone. It is as thin as a sheet of paper. Sinus infections blast straight through this wall to infect the eye.
- Lateral Wall: Thick, dense zygomatic bone. The strongest wall, designed to take a punch.
8.2 Orbital Contents and Innervation
Houses the globe, the lacrimal (tear) gland, massive fat pads (shock absorbers), and the extraocular muscles driving eye movement.
The Motor Formula (LR6-SO4-R3):
- Lateral Rectus: Abducens Nerve (CN VI). Pulls the eye strictly outward.
- Superior Oblique: Trochlear Nerve (CN IV). Runs through a pulley. Pulls the eye down and inward (reading a book).
- All the Rest: Oculomotor Nerve (CN III). Superior, inferior, medial recti, inferior oblique, and the muscle that lifts the eyelid (levator palpebrae).
8.3 Optic Canal and Superior Orbital Fissure
- Optic Canal: Transmits the massive Optic Nerve (CN II) and the Ophthalmic artery. Because the optic nerve is actually an outgrowth of the brain, it is tightly wrapped in all three meningeal layers (Dura, Arachnoid, Pia).
Clinical: This means the subarachnoid space (and its CSF) extends all the way to the back of the eyeball. If pressure skyrockets inside the skull (brain bleed, tumor), that pressure is transmitted straight down the optic nerve sheath, squeezing the central retinal vein and causing the optic disc to swell violently (Papilledema). - Superior Orbital Fissure (SOF): The massive lateral slit transmitting CN III, IV, V1, VI, and the ophthalmic veins.
Clinical: SOF Syndrome involves a tumor or fracture crushing this slit. The patient loses all ability to move the eye (total ophthalmoplegia), the eyelid droops shut, and the cornea is totally numb. Crucially, vision remains perfectly 20/20 because the optic nerve in the separate optic canal is entirely spared. (If vision is lost, it upgrades to Orbital Apex Syndrome).
8.4 Clinical Pathology
Blowout Fracture: A baseball or fist hits the eye directly. The globe doesn't pop; instead, the massive hydraulic pressure is transferred backward. The pressure predictably shatters the absolute weakest point: the Orbital Floor (Maxilla).
The orbital fat and the Inferior Rectus muscle herniate downward into the maxillary sinus, getting trapped in the broken bone shards like a bear trap.
Presentation: The eye sinks backward (enophthalmos). When the patient tries to look UP, the trapped muscle yanks the eye back down, causing severe vertical diplopia (double vision). The fracture also crushes the infraorbital nerve, rendering the patient's entire cheek completely numb.
A horrific, vision-threatening bacterial infection trapped deep behind the orbital septum, almost always tracking through the paper-thin medial wall from an untreated ethmoid sinus infection. The eye turns bright red, swells massively, violently bulges outward (proptosis), and becomes completely frozen and agonizing to move (painful ophthalmoplegia). Vision begins to rapidly degrade as the optic nerve is stretched and choked by the pus. Requires emergent IV antibiotics and urgent surgical decompression to prevent permanent, irreversible blindness.
SECTION 9: THE INFRATEMPORAL FOSSA AND PTERYGOPALATINE FOSSA
9.1 Boundaries and Contents of the Infratemporal Fossa (ITF)
An irregular, deeply hidden space below the zygomatic arch and completely shielded laterally by the thick ramus of the mandible. It acts as the major mechanical and neurovascular junction box for the lower jaw.
- Muscles: Packed with the mighty muscles of mastication—the Medial and Lateral Pterygoids, and the inserting tendon of the Temporalis muscle.
- Vessels: The labyrinthine Pterygoid Venous Plexus and the thick, twisting Maxillary Artery.
- Nerves: The heavy Mandibular Nerve (V3), the Chorda Tympani (jumping on board), and the Otic ganglion.
9.2 The Pterygopalatine Fossa (PPF) and Foramina
A tiny, inverted pyramid-shaped void tucked deeply between the pterygoid plates and the back of the maxilla. It is the ultimate crossroads, sporting 7 highly specific doors leading to entirely different regions of the head.
The Communications:
- Foramen Rotundum: The back door. Lets the Maxillary nerve (V2) in from the brain.
- Pterygoid (Vidian) Canal: A posterior tunnel bringing in heavy autonomic fibers (the nerve of the pterygoid canal) to drive the ganglion.
- Inferior Orbital Fissure: The skylight. Shoots nerves and vessels straight up into the floor of the eye socket.
- Sphenopalatine Foramen: The medial side door. Blasts the massive sphenopalatine artery straight into the nasal cavity (the source of lethal posterior nosebleeds).
- Pterygopalatine Canal: The floor drain. Drops the greater and lesser palatine nerves/arteries straight down to supply the roof of the mouth.
Clinical Pearl: Because V2 branches exclusively through this tiny 1cm box, oral surgeons and pain specialists can insert a long needle high into the mouth and flood the PPF with local anesthetic. This single Pterygopalatine Ganglion Block instantly numbs the entire mid-face, upper teeth, nasal cavity, and palate simultaneously, providing immense relief for severe trigeminal neuralgia.
9.3 Maxillary Artery and Mandibular Nerve (V3)
Divided into three segments as it weaves through the ITF:
- 1st Part (Mandibular): Drops the Middle Meningeal Artery up through the foramen spinosum, and the Inferior Alveolar Artery down into the jawbone to feed the teeth.
- 2nd Part (Pterygoid): Feeds all the chewing muscles (Masseteric, deep temporal, buccal).
- 3rd Part (Pterygopalatine): Enters the PPF to supply the face, nose, and palate.
The only Trigeminal division carrying motor fibers (driving the chewing muscles). Its massive sensory branches dominate the lower face:
- Auriculotemporal Nerve: Loops around the middle meningeal artery. Supplies the temple and the TMJ joint.
- Lingual Nerve: Carries general sensation for the anterior 2/3 of the tongue. It acts as a taxi cab for the Chorda Tympani (which brings taste and saliva commands).
- Inferior Alveolar Nerve: Dives straight into the bone of the jaw to provide profound sensation to all lower teeth, emerging at the chin as the mental nerve.
9.4 Clinical Relevance
- Mandibular Fractures: The jaw acts like a bony ring. If it takes a massive blow, it almost always breaks in two places simultaneously (e.g., a punch to the chin shatters the chin AND snaps the delicate condylar necks near the ear). The fracture frequently shears the Inferior Alveolar Nerve trapped inside the bone, leaving the patient with a completely numb lower lip and chin.
- TMJ Disorders: The TMJ is a unique synovial joint featuring an intervening fibrocartilaginous disc. In TMJ dysfunction, this disc slips out of place, causing loud, painful popping and clicking every time the jaw opens.
- Juvenile Nasopharyngeal Angiofibroma (JNA): A highly aggressive, bleeding, benign tumor that occurs almost exclusively in adolescent males. It originates exactly at the sphenopalatine foramen and aggressively invades the PPF, nasal cavity, and orbit. Biopsying this tumor in a clinic is strictly contraindicated, as the patient can exsanguinate (bleed to death) in minutes due to its intense vascularity.
SECTION 10: INTEGRATED CLINICAL CASES AND REVIEW
10.1 Case 1: Sinusitis Complications
Presentation: A 7-year-old boy presents with 5 days of severe nasal congestion, purulent rhinorrhea, and high fever (39.2 C). Overnight, his right eye swelled violently. It is bright red, bulging forward (proptosis), and he screams in agony when asked to look left or right.
Diagnosis: Acute ethmoid sinusitis progressing to Orbital Cellulitis (postseptal infection).
Pathophysiology: The bacterial infection in the honeycomb ethmoid sinuses melted straight through the paper-thin Lamina Papyracea bone, dumping gallons of pus directly into the fat and muscle cone behind the eye.
Management: This is a vision-threatening emergency. Order an immediate STAT CT scan of the orbits. Start massive broad-spectrum IV antibiotics (Ceftriaxone + Metronidazole). An ophthalmologist must be consulted for emergent surgical drainage if a large abscess is crushing the optic nerve.
Monitor heavily for the deadliest complication: the infection tracking backwards via ophthalmic veins to cause Cavernous Sinus Thrombosis.
10.2 Case 2: Airway Obstruction
Presentation: A terrified 4-year-old unvaccinated girl is rushed into the ER. She awoke suddenly, gasping for air. She is sitting straight up in the "tripod position," leaning forward with her chin thrust out, violently drooling because she cannot swallow her own saliva. She has a high fever and a muffled, thick "hot potato" voice.
Diagnosis: Acute Epiglottitis.
Pathophysiology: A furious bacterial infection (likely Haemophilus influenzae type B) has caused the epiglottis to swell to the size of a thumb, acting like a physical cork plugging the top of the windpipe.
Management: ABSOLUTE AIRWAY EMERGENCY. Do NOT force a tongue depressor into her mouth to look; the stress and gag reflex will cause the airway to instantly spasm shut, killing the child. Keep her perfectly calm in her mother's arms. Rush her to the operating room. An anesthesiologist and ENT surgeon must perform a highly controlled fiberoptic intubation. If the throat is completely sealed shut with swelling, the surgeon must immediately slash the neck and perform an emergent cricothyroidotomy through the cricothyroid membrane to establish a breathing tube. Follow with heavy IV Ceftriaxone.
10.3 Case 3: Deep Neck Space Infection
Presentation: A 55-year-old poorly controlled diabetic male presents with 3 days of agonizing, worsening neck swelling and dysphagia. He had a severely decayed, painful lower molar pulled by a street dentist one week ago. On exam, the underside of his jaw is massively swollen bilaterally, feeling as hard as a wooden board (a "bull neck"). His tongue is pushed so far up and backward that he is choking on it and demonstrating severe inspiratory stridor.
Diagnosis: Ludwig's Angina (massive bilateral cellulitis of the submandibular, sublingual, and submental fascial spaces).
Pathophysiology: A highly virulent, rotting polymicrobial infection (Strep, Staph, and foul anaerobes) exploded out of the infected molar root, dropping below the mylohyoid line directly into the neck's fascial spaces. The expanding pus physically displaces the massive tongue backward into the pharynx.
Management: Airway protection is the absolute paramount concern; the patient is minutes away from suffocation. Requires an awake fiberoptic intubation or immediate surgical tracheostomy under local anesthesia. Blast with broad-spectrum IV antibiotics (e.g., Piperacillin-tazobactam). Obtain a STAT neck CT. The surgeon must make wide, deep external incisions under the jaw to physically drain the pressurized pus, and completely extract the remaining rotting dental fragments. Transfer to the ICU for relentless airway monitoring.
10.4 High-Yield Summary Tables
| Nasal Meatus / Recess | Structures Draining Into It |
|---|---|
| Superior Meatus | Posterior ethmoidal air cells |
| Middle Meatus | Frontal sinus, Maxillary sinus, Anterior & Middle ethmoidal air cells |
| Inferior Meatus | Nasolacrimal duct (Tears) |
| Sphenoethmoidal Recess | Sphenoid sinus |
| Region of Tongue | General Sensation (Touch/Pain) | Special Sensation (Taste) |
|---|---|---|
| Anterior 2/3 | Lingual nerve (V3) | Chorda tympani (CN VII) |
| Posterior 1/3 | Glossopharyngeal nerve (CN IX) | Glossopharyngeal nerve (CN IX) |
| Extreme Posterior (Vallecula) | Internal laryngeal nerve (CN X) | Internal laryngeal nerve (CN X) |
| Motor Innervation | Hypoglossal nerve (CN XII) innervates all muscles EXCEPT Palatoglossus (Vagus nerve, CN X) | |
| Nerve Branch | Specific Path / Motor Function | Sensory Territory |
|---|---|---|
| Superior Laryngeal Nerve (Internal Branch) | Pierces thyrohyoid membrane. No motor function. | Sensation ABOVE the vocal folds (Supraglottis) + taste from epiglottis. |
| Superior Laryngeal Nerve (External Branch) | Motor strictly to the Cricothyroid muscle (tenses cords). | None |
| Recurrent Laryngeal Nerve (RLN) | Left loops under aortic arch; Right loops under subclavian. Motor to ALL other intrinsic muscles. | Sensation BELOW the vocal folds (Infraglottis/Subglottis). |
| Fossa | Foramen | Key Neurovascular Contents |
|---|---|---|
| Anterior Fossa | Cribriform plate | Olfactory nerve filaments (CN I) |
| Foramen cecum | Nasal emissary vein to superior sagittal sinus | |
| Middle Fossa | Optic canal | Optic nerve (CN II), Ophthalmic artery |
| Superior orbital fissure | CN III, CN IV, V1 (Ophthalmic), CN VI, Ophthalmic veins | |
| Foramen rotundum | Maxillary nerve (V2) | |
| Foramen ovale | Mandibular nerve (V3), Accessory meningeal artery | |
| Foramen spinosum | Middle meningeal artery and vein | |
| Carotid canal | Internal carotid artery (petrous segment) | |
| Posterior Fossa | Foramen magnum | Medulla oblongata, Vertebral arteries, CN XI spinal roots |
| Internal acoustic meatus | CN VII (Facial), CN VIII (Vestibulocochlear), Labyrinthine artery | |
| Jugular foramen | CN IX, CN X, CN XI, Internal jugular vein | |
| Hypoglossal canal | Hypoglossal nerve (CN XII) | |
| Condylar canal | Condylar emissary vein |
| Location within Sinus | Anatomical Structures |
|---|---|
| Lateral Wall (Embedded in Dura, Superior to Inferior) |
1. Oculomotor nerve (CN III) 2. Trochlear nerve (CN IV) 3. Ophthalmic division of trigeminal (V1) 4. Maxillary division of trigeminal (V2) |
| Center (Free floating within venous blood pool) |
1. Internal carotid artery (with wrapped sympathetic plexus) 2. Abducens nerve (CN VI) - sits inferolateral to the ICA |
References and Evidence-Based Guidelines
- Standring, S. (2020). Gray's Anatomy: The Anatomical Basis of Clinical Practice (42nd ed.). Elsevier. (Definitive reference for deep skull base fossae, cranial nerve pathways, and fascial planes).
- Moore, K. L., Dalley, A. F., & Agur, A. M. R. (2017). Clinically Oriented Anatomy (8th ed.). Lippincott Williams & Wilkins. (Key resource for the clinical correlations of airway obstruction, TMJ dislocation, and orbital blow-out fractures).
- Netter, F. H. (2018). Atlas of Human Anatomy (7th ed.). Elsevier. (Visual spatial referencing for the intricate 3D anatomy of the Pterygopalatine and Infratemporal fossae).
- Flint, P. W., et al. (2020). Cummings Otolaryngology: Head and Neck Surgery (7th ed.). Elsevier. (Advanced clinical pathology referencing for deep neck space infections, Ludwig's Angina, and Cavernous Sinus Thrombosis).