Deep Structures of the Head: High-Yield Anatomy & Clinical Correlations
By the conclusion of this exhaustive master guide, you will be deeply conversant with:
- The osteology, compartmentalization, and major foramina of the cranial fossae, including their exact neurovascular contents.
- The complex 3D boundaries, contents, and clinical significance of the Infratemporal Fossa (ITF) and Pterygopalatine Fossa (PPF).
- The intricate pathways of cranial nerves, specifically the "hitchhiking" routes of parasympathetic autonomic fibers.
- The anatomical basis for differentiating Central (UMN) vs. Peripheral (LMN) nerve lesions.
- The deep vascular networks, focusing on the Cavernous Sinus, its connections, and the fatal progression of Cavernous Sinus Thrombosis (CST).
SECTION 1: Osteology & Foramina of the Skull Base
The base of the skull is the foundational floor upon which the brain rests. It is a highly complex, perforated bony landscape that serves as the gateway between the central nervous system and the rest of the body. Pathologies here—such as fractures, tumors, or infections—have profound, often immediate life-threatening consequences.
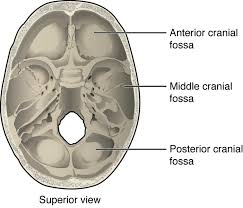
The Three Cranial Fossae
The cranial floor is organized into three distinct "terraces" or fossae, descending like steps from front to back.
Houses the frontal lobes and olfactory bulbs.
- Boundaries: Posteriorly bounded by the lesser wing of the sphenoid bone. Anteriorly bounded by the frontal bone. The midline floor is formed by the delicate, perforated cribriform plate of the ethmoid bone.
- Clinical Correlation: Severe head trauma can shear the fragile olfactory filaments passing through the cribriform plate, resulting in permanent anosmia (loss of smell). A fracture here tears the meninges, leading to CSF rhinorrhea (cerebrospinal fluid leaking from the nose).
Houses the temporal lobes and the pituitary gland.
- Boundaries: Anteriorly bounded by the lesser wing of the sphenoid. Posteriorly bounded by the thick, bony petrous ridge of the temporal bone. The floor consists of the greater wing of the sphenoid and the squamous temporal bone.
- Clinical Correlation: The pituitary gland sits squarely in the midline (sella turcica). Pituitary macroadenomas usually expand upward, compressing the optic chiasm (causing bitemporal hemianopsia/tunnel vision). Massive pressure in this fossa can cause the temporal lobe to undergo uncal herniation down through the tentorial incisura, compressing the brainstem.
Houses the cerebellum, pons, and medulla oblongata.
- Boundaries: Anteriorly bounded by the petrous ridge and the dorsum sellae. Posteriorly bounded by the occipital bone. The center features the massive opening, the foramen magnum.
- Clinical Correlation: Due to the rigid boundaries, any expanding mass (like a cerebellar tumor or hemorrhage) will cause catastrophic fatal mass effect. The pressure forces the cerebellar tonsils down through the foramen magnum (Tonsillar herniation), crushing the respiratory and cardiac centers in the medulla.
Major Foramina: Exact Contents
Mastering the exact contents of these "holes" (foramina) is crucial, as a tumor growing in a specific foramen will present with predictable deficits.
| Foramen / Opening | Location | Exact Neurovascular Contents |
|---|---|---|
| Cribriform Plate | Anterior Fossa | Olfactory nerve filaments (CN I) from the nasal mucosa. |
| Optic Canal | Middle Fossa | Optic nerve (CN II) + Ophthalmic artery (first branch of ICA). |
| Superior Orbital Fissure (SOF) | Middle Fossa | CN III (Oculomotor), CN IV (Trochlear), CN V1 (Ophthalmic division of Trigeminal), CN VI (Abducens) + sympathetic fibers + Superior ophthalmic vein. |
| Foramen Rotundum | Middle Fossa | Maxillary nerve (CN V2) passing to the Pterygopalatine Fossa. |
| Foramen Ovale | Middle Fossa | Mandibular nerve (CN V3) + Accessory meningeal artery + emissary veins. |
| Foramen Spinosum | Middle Fossa | Recurrent meningeal branch of V3 + Middle meningeal artery & vein. (Epidural hematomas originate here). |
| Internal Acoustic Meatus (IAM) | Posterior Fossa | CN VII (Facial) + CN VIII (Vestibulocochlear) + Labyrinthine artery. |
| Jugular Foramen | Posterior Fossa | Pars nervosa: CN IX (Glossopharyngeal), X (Vagus), XI (Spinal Accessory). Pars vascularis: CN X, XI + Internal jugular vein. |
| Hypoglossal Canal | Posterior Fossa | CN XII (Hypoglossal nerve). |
| Carotid Canal | Middle Fossa | Internal carotid artery (ICA - petrous and lacerum segments) + sympathetic plexus. |
CLINICAL PEARL: The Foramen Lacerum Illusion
In a dried skull, the foramen lacerum looks like a massive hole. However, in a living human, it is completely plugged and filled with cartilage. The Internal Carotid Artery (ICA) passes OVER it, sliding across the cartilage bed; it does not travel THROUGH it.
Mnemonic for Middle Fossa (Lateral → Medial):
Stupid Old Rats Frequently Spin = SOF, Optic canal, foramen Rotundum, foramen Ovale, foramen Spinosum.
Skull Base Fractures & CSF Leakage
Basilar skull fractures are notoriously difficult to see on standard X-rays. Diagnosis relies heavily on highly specific clinical signs.
- Anterior Fossa Fracture (Frontal/Ethmoid bones):
- CSF Rhinorrhea: Tearing of the meninges over the cribriform plate allows cerebral spinal fluid to drip directly into the nasal cavity.
- 'Halo Sign': If bloody fluid from the nose is dripped onto filter paper or bed linen, the rapidly spreading CSF forms a clear, yellowish ring (halo) around a central dot of blood.
- Raccoon Eyes (Bilateral periorbital ecchymosis): Blood tracks down into the soft tissue around the eyes. Because the nasal cavity is heavily colonized with bacteria, these patients are at massive risk for ascending bacterial meningitis.
- Middle Fossa Fracture (Temporal bone):
- CSF Otorrhea: A fracture through the tegmen tympani (roof of the middle ear) combined with a perforated tympanic membrane (eardrum) allows CSF to leak out of the ear.
- Battle's Sign: Ecchymosis (bruising) over the mastoid process behind the ear. This is a delayed sign, taking 24–48 hours to appear.
- Nerve Deficits: The facial canal and IAM are housed in the temporal bone. Fractures here frequently severe or compress the Facial nerve (causing CN VII palsy/facial droop) and the Vestibulocochlear nerve (causing CN VIII dysfunction: extreme vertigo, tinnitus, and sensorineural hearing loss).
- Posterior Fossa Fracture: Rare, but associated with extremely high mortality due to direct brainstem compression and massive deficits in lower cranial nerves (CN IX–XII).
SECTION 2: The Infratemporal Fossa (ITF)
The Infratemporal Fossa is an irregularly shaped, completely hidden space located deep and inferior to the zygomatic arch, and deep to the ramus of the mandible. It acts as a massive distribution center for the neurovasculature of the lower jaw, chewing muscles, and teeth.
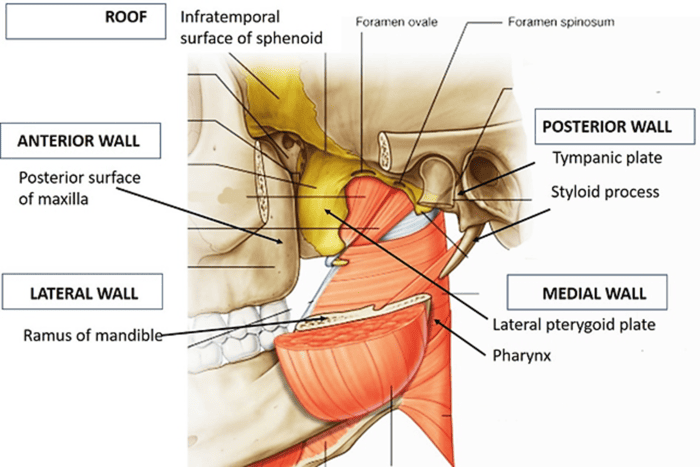
ITF Boundaries (The Inverted Pyramid)
- Superior (Roof): Infratemporal surface of the greater wing of the sphenoid. (Crucially, the foramen ovale and spinosum open down into this roof, dropping nerves and arteries into the fossa).
- Medial: Lateral pterygoid plate; tensor/levator veli palatini muscles; superior pharyngeal constrictor. It is continuous with the Pterygopalatine Fossa (PPF) deeper inside via the pterygomaxillary fissure.
- Lateral: The inner surface of the ramus of the mandible; coronoid and condylar processes.
- Anterior: Posterior surface of the maxilla (which forms the posterior wall of the maxillary sinus).
- Posterior: Medially bounded by the carotid sheath structures; laterally bounded by the styloid process & tympanic part of the temporal bone.
- Inferior: Unlike the roof, there is no distinct bony floor. It is functionally bounded by the attachment of the medial pterygoid muscle to the mandible.
The Pterygoid Muscles (Muscles of Mastication)
The ITF is packed with the two pterygoid muscles, which are vital for complex chewing motions.
- Origin: Two heads. Superior head arises from the infratemporal surface of the greater wing of sphenoid. Inferior head arises from the lateral surface of the lateral pterygoid plate.
- Insertion: Superior head inserts into the articular disc and capsule of the TMJ. Inferior head inserts into the neck of the mandibular condyle.
- Action: Bilateral contraction causes protrusion (pushing the jaw forward). Unilateral contraction produces contralateral side-to-side grinding (moves jaw to the opposite side).
- Nerve: Nerve to lateral pterygoid (branch from the anterior division of CN V3).
- Origin: Deep head arises from the medial surface of the lateral pterygoid plate. Superficial head arises from the maxillary tuberosity and pyramidal process.
- Insertion: Medial surface of the mandibular ramus/angle (specifically the pterygoid tuberosity).
- Action: Strongly elevates the mandible (closes the mouth); assists in grinding; stabilizes the condyle during movement.
- Nerve: Nerve to medial pterygoid (direct branch from the main trunk of CN V3).
CLINICAL PEARL for Exam Day:
Lateral opens (Lowers/Protrudes the jaw); Medial closes (Elevates the jaw). The lateral pterygoid is the primary muscle responsible for opening the mouth against resistance.
Mandibular Nerve (CN V3): Course & Branches
The largest division of the trigeminal nerve drops through the foramen ovale directly into the ITF. It immediately splits into distinct motor and sensory networks.
- Main Trunk (before bifurcation): Gives off motor branches (Nerve to medial pterygoid, Nerve to tensor tympani, Nerve to tensor veli palatini) and one sensory branch, the Meningeal branch (nervus spinosus), which travels back up through the foramen spinosum to innervate the dura of the middle cranial fossa.
- Anterior Division (Mainly Motor):
- Masseteric nerve → innervates masseter muscle.
- Deep temporal nerves → innervate temporalis muscle.
- Nerve to lateral pterygoid.
- Buccal nerve: The ONLY sensory branch of the anterior division. Supplies sensation to the skin of the cheek, buccal mucosa, and posterior lower molar gingiva.
- Posterior Division (Mainly Sensory):
- Auriculotemporal nerve: Famously splits into two roots to wrap around the middle meningeal artery. Supplies sensation to the temple and auricle. Critically, it acts as a "hitchhiking" highway, carrying postganglionic parasympathetic fibers from the otic ganglion to the parotid gland.
- Lingual nerve: Provides general sensation (touch, pain, temperature) to the anterior 2/3 of the tongue. Deep in the ITF, it is joined by the chorda tympani.
- Inferior alveolar nerve (IAN): Enters the mandibular foramen to supply all the lower teeth. It emerges from the mental foramen as the mental nerve to supply the chin and lower lip. Before entering the bone, it gives off a motor branch: the nerve to the mylohyoid (supplies mylohyoid and anterior belly of digastric).
Chorda Tympani (CN VII) & Maxillary Artery
- Chorda Tympani: A special branch of the Facial Nerve.
- Origin: Branches off the facial nerve within the facial canal (~6 mm above the stylomastoid foramen).
- Course: Crosses the tympanic cavity (middle ear), exits the skull via the petrotympanic fissure, and drops into the ITF to join the lingual nerve.
- Functions: Carries special sensory fibers (Taste) from the anterior 2/3 of the tongue, and preganglionic parasympathetic secretomotor fibers destined for the submandibular & sublingual salivary glands.
- Clinical Scenario: If a patient suffers a severe injury to the proximal lingual nerve high in the ITF, they lose BOTH general sensation and taste on the anterior tongue. However, if they have middle ear surgery and suffer an isolated injury to the chorda tympani, they will complain of loss of taste only, while general touch/pain sensation remains perfectly intact.
- Maxillary Artery: The massive terminal branch of the External Carotid Artery. It is anatomically divided into 3 parts relative to its position to the lateral pterygoid muscle.
- 1st Part (Mandibular): Deep auricular, anterior tympanic, middle meningeal, inferior alveolar arteries.
- 2nd Part (Pterygoid): Muscular branches: Masseteric, deep temporal, pterygoid, buccal arteries.
- 3rd Part (Pterygopalatine): Passes through the pterygomaxillary fissure into the PPF. Branches: Posterior superior alveolar, infraorbital, descending palatine, sphenopalatine arteries.
Pterygoid Venous Plexus & TMJ Dislocation
The Pterygoid Venous Plexus is a vast network of veins surrounding the maxillary artery and lateral pterygoid muscle. It anastomoses anteriorly with the facial vein.
Crucially, it connects directly upward to the cavernous sinus inside the skull via emissary veins passing through the foramen ovale. CLINICAL: This is why the "Danger Triangle of the Face" (upper lip, nose, medial canthus) is so lethal. Squeezing a pimple or suffering an infection here allows bacteria to travel backward (retrograde) through valveless veins into the pterygoid plexus, and ultimately into the brain, causing cavernous sinus thrombosis.
The Temporomandibular Joint (TMJ) is a unique synovial, modified hinge joint separated by a biconcave fibrocartilage disc into a superior gliding compartment and an inferior hinge compartment.
Clinical Scenario: TMJ Dislocation
When a person yawns excessively wide, takes a massive bite of food, or laughs violently, the condyle of the mandible glides too far forward and slips completely anterior to the articular tubercle. The jaw becomes locked wide open.
Why can't the patient just close their mouth? The intense pain triggers an immediate, massive reflex spasm of the powerful elevator muscles (masseter, temporalis, medial pterygoid). These spasming muscles pull the dislocated condyle tightly up against the bone, locking it in the dislocated position. A physician must manually push the jaw downward (to overcome the muscle spasm) and then backward to reduce the joint.
SECTION 3: The Pterygopalatine Fossa (PPF)
If the ITF is the distribution center for the lower jaw, the Pterygopalatine Fossa (PPF) is the highly protected, central "Grand Central Station" for neurovascular supply to the mid-face, nasal cavity, palate, and orbit.
PPF Boundaries & 3D Geometry
The PPF is a tiny inverted pyramid (only 2 cm deep and 1 cm wide) located deep to the ITF, and directly posterior to the maxilla.
- Anterior: Posterior wall of the maxilla (maxillary tuberosity).
- Posterior: Pterygoid process & greater wing of the sphenoid. (This wall is perforated by the foramen rotundum, pterygoid/Vidian canal, and palatovaginal canal).
- Medial: Perpendicular plate of the palatine bone. (Contains the sphenopalatine foramen opening into the nose).
- Lateral: There is NO bony wall here! It freely communicates with the ITF via the open pterygomaxillary fissure.
- Superior (Roof): Greater wing of sphenoid. The inferior orbital fissure opens here.
- Inferior: Pyramidal process of the palatine bone, where the fossa tapers down into the greater palatine canal.
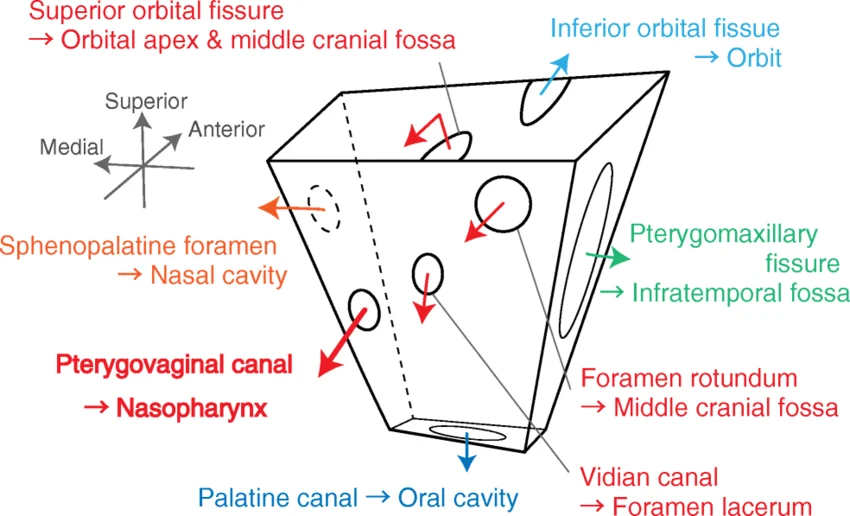
The Seven Pathways/Openings of the PPF
Every major nerve and vessel entering or leaving the PPF must pass through one of these seven "gates".
- Foramen Rotundum → Middle Cranial Fossa: Transmits the Maxillary nerve (CN V2) into the PPF.
- Pterygomaxillary Fissure → Infratemporal Fossa: The lateral door. Transmits the posterior superior alveolar nerve and allows the terminal 3rd part of the maxillary artery to enter.
- Pterygoid (Vidian) Canal → Middle Cranial Fossa/Foramen Lacerum: Transmits the nerve, artery, and vein of the pterygoid canal.
- Palatovaginal (Pharyngeal) Canal → Nasopharynx: Transmits pharyngeal branches of the maxillary nerve & artery.
- Inferior Orbital Fissure → Orbit: The ceiling door. Transmits the zygomatic nerve, and the infraorbital artery & vein.
- Greater Palatine Canal → Oral Cavity: The floor drain. Transmits the greater & lesser palatine nerves, and descending palatine artery & vein to supply the roof of the mouth.
- Sphenopalatine Foramen → Nasal Cavity (Superior Meatus): The medial door. Transmits the sphenopalatine artery & vein, and the nasopalatine nerve to supply the inside of the nose.
Maxillary Nerve (CN V2) in the PPF
The maxillary nerve is a purely sensory nerve. It enters the PPF through the foramen rotundum and explodes into a web of branches:
- Zygomatic Nerve: Enters the orbit via the inferior orbital fissure, splitting into zygomaticotemporal & zygomaticofacial branches. Crucially, it acts as a courier, carrying hitchhiking parasympathetic fibers from the pterygopalatine ganglion up to the lacrimal gland (to make tears).
- Posterior Superior Alveolar Nerve: Exits sideways via the pterygomaxillary fissure to plunge into the maxilla, innervating the upper molars and gingiva.
- Ganglionic Branches: Two short, stout branches that physically suspend the pterygopalatine ganglion from the nerve trunk.
- Infraorbital Nerve: The direct anatomical continuation of V2. It shoots forward into the orbit via the inferior orbital fissure, runs along the orbital floor in the infraorbital groove and canal, and emerges onto the face at the infraorbital foramen. It provides sensory supply to the lower eyelid, lateral nose, upper lip, and cheek skin. Along the way, it drops down the middle & anterior superior alveolar nerves to supply the upper premolars, canines, and incisors.
The Pterygopalatine Ganglion
This is the LARGEST parasympathetic ganglion in the head. It is physically suspended in the PPF from the maxillary nerve.
- Sensory Root: Passing through from the maxillary nerve (V2).
- Parasympathetic Root: Preganglionic fibers from the facial nerve (CN VII). They travel as the greater petrosal nerve, which synapses in this ganglion.
- Sympathetic Root: Postganglionic fibers from the internal carotid plexus traveling as the deep petrosal nerve.
- The Combined Root: The greater petrosal (parasympathetic) and deep petrosal (sympathetic) nerves merge together inside the skull to form the Nerve of the Pterygoid Canal (Vidian nerve), which enters the back of the PPF to plug into the ganglion.
- Function: The ganglion acts as an autonomic switchboard. Its parasympathetic outputs drive heavy secretion from the lacrimal (tear) gland, and the mucosal glands of the nose and palate. The sympathetic fibers cause vasoconstriction in these same areas to reduce blood flow and secretions.
Sphenopalatine Artery & Severe Epistaxis (Nosebleeds)
The Sphenopalatine Artery is the massive terminal branch of the maxillary artery. It bursts through the sphenopalatine foramen directly onto the lateral wall of the nasal cavity. It is the major supplier of blood to the highly vascular nasal mucosa.
Clinical Emergency: It is rightfully nicknamed the 'Artery of Epistaxis'. While childhood nosebleeds usually occur from the front of the nose (Kiesselbach's plexus/Little's area) and stop with simple pinching, POSTERIOR nosebleeds are massive, arterial, and life-threatening. The blood pours down the back of the patient's throat.
Treatment: First-line treatment involves deep nasal cautery, heavy topical vasoconstrictors, or intense balloon packing. In refractory, uncontrollable cases, surgeons must perform an endoscopic sphenopalatine artery ligation or transmaxillary embolization to permanently tie off the bleeder at its source.
SECTION 4: Cranial Nerves & Autonomic Pathways
Understanding the deep pathways of cranial nerves is vital for localizing brainstem and skull base lesions.
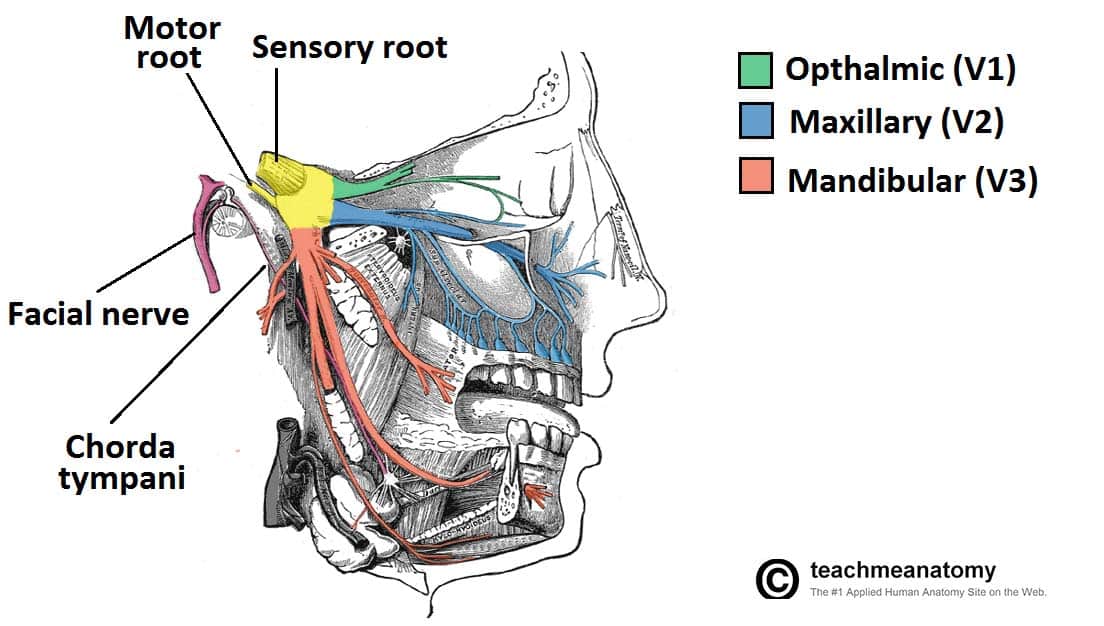
1. Trigeminal Nerve (CN V) Pathway
The great sensory nerve of the face and motor nerve of chewing.
- Emerges from the ventrolateral pons, crosses the prepontine cistern, and enters Meckel's cave (a dural pouch in the petrous apex). Here lies the massive Trigeminal (Gasserian) ganglion holding all the sensory cell bodies.
- V1 (Ophthalmic): Exits via the superior orbital fissure into the orbit. Supplies the upper face, cornea, nasal cavity, and forehead. It travels embedded in the lateral wall of the cavernous sinus.
- V2 (Maxillary): Exits via the foramen rotundum into the PPF. Supplies the mid-face. Also travels embedded in the lateral wall/inferior aspect of the cavernous sinus.
- V3 (Mandibular): Exits via the foramen ovale into the ITF. This is the only division containing motor fibers (to the muscles of mastication).
2. Facial Nerve (CN VII) Pathway
- Emerges at the cerebellopontine angle (CPA), travels through the internal acoustic meatus alongside CN VIII, and enters the tortuous facial canal within the petrous temporal bone.
- Features the Geniculate Ganglion (1st sensory ganglion for taste).
- Key branches inside the canal:
- Greater Petrosal Nerve: Exits at the hiatus, drives the PPF ganglion.
- Nerve to Stapedius: Motor to the tiny stapedius muscle in the ear (dampens loud noises).
- Chorda Tympani: Exits via the petrotympanic fissure (taste + salivary glands).
- Exit: Plunges out of the skull base through the stylomastoid foramen to fan out across the face, supplying motor innervation to all muscles of facial expression.
3. Glossopharyngeal Nerve (CN IX) Pathway
- Emerges from the postolivary sulcus of the medulla. Exits the skull through the anteromedial pars nervosa of the Jugular Foramen.
- Gives off the Tympanic Nerve (Jacobson's nerve), which re-enters the skull to form a plexus in the middle ear, eventually emerging as the Lesser Petrosal Nerve to drive the otic ganglion (parotid gland secretion).
- Also provides the Carotid nerve (monitoring blood pressure/oxygen at the carotid sinus/body), pharyngeal motor branches, and sensory branches for the posterior 1/3 of the tongue (taste and general touch/gag reflex).
Parasympathetic 'Hitchhiking' Pathways
Autonomic parasympathetic nerves are lazy; once they leave their specific ganglia, they refuse to build their own roads. Instead, they physically jump onto the thick, established branches of the Trigeminal Nerve (CN V) to reach their target organs. This is called "hitchhiking."
| Parasympathetic Ganglion | Origin Nerve | Hitchhiking Route / Trigeminal Carrier | Final Target |
|---|---|---|---|
| Ciliary Ganglion | CN III (Oculomotor / Edinger-Westphal nucleus) | Hitchhikes via the Short Ciliary Nerves (branches of V1). | Sphincter pupillae (constricts pupil) & Ciliary muscle (lens accommodation). |
| Pterygopalatine Ganglion | CN VII (Facial / Superior salivatory nucleus) | Hitchhikes via Zygomatic/Lacrimal branches (of V2). | Lacrimal gland (tears), nasal, and palatine mucosal glands. |
| Otic Ganglion | CN IX (Glossopharyngeal / Inferior salivatory nucleus) | Hitchhikes via the Auriculotemporal nerve (branch of V3). | Parotid salivary gland (spit). |
| Submandibular Ganglion | CN VII (Facial / Superior salivatory nucleus via Chorda tympani) | Hitchhikes via the Lingual nerve (branch of V3). | Submandibular & sublingual salivary glands. |
Central (UMN) vs. Peripheral (LMN) Lesions
Distinguishing where a nerve is damaged is critical for separating a massive stroke from a benign localized nerve palsy.
FACIAL NERVE (CN VII):
- Central (Upper Motor Neuron / Stroke): The forehead is cortically innervated by BOTH the left and right sides of the brain. Therefore, a stroke on one side of the brain results in Contralateral lower facial paralysis ONLY. The patient's mouth droops, but they can still wrinkle their forehead because the undamaged opposite side of the brain is keeping the upper face alive.
- Peripheral (Lower Motor Neuron / Bell's Palsy): The nerve is damaged after the fibers have merged in the brainstem. This causes Ipsilateral COMPLETE facial paralysis. The patient cannot wrinkle their forehead, close their eye, or smile on that entire half of the face. Associated with hyperacusis (loud sounds due to stapedius paralysis) and loss of anterior taste.
TRIGEMINAL NERVE (CN V):
- Central: Contralateral hemifacial sensory loss. When asked to open the mouth, the jaw deviates TOWARD the side of the brain lesion (because the contralateral pterygoid muscles are paralyzed).
- Peripheral: Ipsilateral sensory loss. The jaw deviates TOWARD the paralyzed side of the face (the weak lateral pterygoid is overpowered by the healthy side pushing the jaw over).
GLOSSOPHARYNGEAL (CN IX):
- Peripheral: Results in ipsilateral loss of taste on the posterior 1/3 of the tongue, decreased parotid secretion (dry mouth), and an absent carotid sinus reflex.
SECTION 5: Deep Vascular & Venous Systems
Cavernous Sinus Anatomy
The cavernous sinuses are paired, complex, blood-filled dural venous spaces sitting deep in the skull on either side of the sella turcica (pituitary fossa). They stretch from the superior orbital fissure anteriorly to the petrous apex posteriorly.
Boundaries:
- Medial: Body of the sphenoid, separated from the pituitary fossa by a thin dural membrane.
- Lateral: A thick dural wall containing embedded cranial nerves (CN III, IV, V1, V2).
- Superior/Inferior: Anterior clinoid process above; greater wing of sphenoid below.
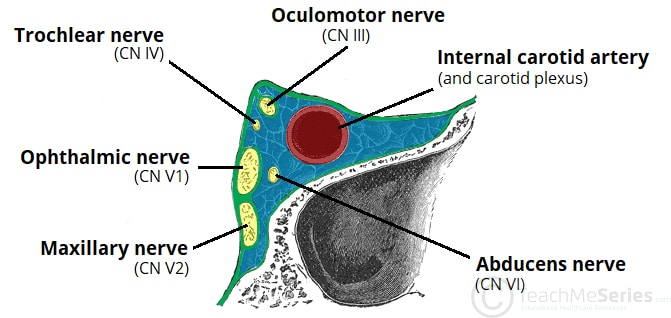
Exact Contents (Mnemonic 'O TOM CAT'):
The nerves are strictly organized. The lateral wall holds them in descending vertical order. The most critical structures float completely free and unprotected in the center of the venous blood pool.
- O = Oculomotor (CN III) — lateral wall, superior.
- T = Trochlear (CN IV) — lateral wall.
- O = Ophthalmic (V1) — lateral wall.
- M = Maxillary (V2) — lateral wall, inferolateral.
- C = Carotid artery (ICA) — WITHIN the sinus blood pool.
- A = Abducens (CN VI) — WITHIN the sinus blood pool, hugging the inferolateral edge of the ICA.
- T = Trochlear (sympathetic plexus wrapped around the ICA).
Internal Carotid Artery (ICA) Course
The ICA takes a massive, twisting journey to supply the brain.
- Cervical Segment: Travels straight up the neck within the carotid triangle. Crucially, it gives off NO branches in the neck (unlike the external carotid).
- Petrous Segment: Enters the carotid canal in the temporal bone. Makes a sharp 90° turn, running vertically then horizontally. Gives off small caroticotympanic arteries.
- Lacerum Segment: Glides cleanly over the cartilage-filled foramen lacerum; it does NOT dive through it.
- Cavernous Segment: Plunges directly through the cavernous sinus. This is the ONLY artery in the human body completely surrounded by venous blood. Gives off the meningohypophyseal trunk and is densely wrapped in a sympathetic neural plexus.
- Clinoid & Ophthalmic Segments: Emerges from the sinus through dural rings near the anterior clinoid process. Gives off the vital Ophthalmic artery, which follows the optic nerve into the orbit.
- Communicating Segment: Terminates by splitting into the anterior and middle cerebral arteries (the major blood supply to the cerebral cortex).
Clinical Emergency: Cavernous Sinus Thrombosis (CST)
Pathophysiology: The veins of the face and orbits (ophthalmic veins, pterygoid plexus) are valveless. This permits bidirectional blood flow. A severe, untreated bacterial infection on the face (the "Danger Triangle") or inside the orbit can spread backward, deep into the skull, causing a massive, septic blood clot (thrombophlebitis) to form inside the cavernous sinus.
Clinical Presentation & Progression:
- Early Signs: Blinding headache, severe periorbital edema (swollen eyes), chemosis (conjunctival swelling), proptosis (bulging eyes), and high spiking fevers.
- Cranial Nerve Deficits (Occur in a strict, specific order):
- 1. CN VI (ABDUCENS) is affected FIRST. Why? Because it runs entirely free and unprotected directly within the infected venous blood pool of the sinus. The patient loses the ability to look outward (lateral gaze palsy).
- 2. CN III, IV, V1: The infection then eats into the lateral dural wall. The patient develops a fully "down and out" paralyzed eye, severe ptosis (drooping eyelid), and diplopia (double vision).
- 3. V2: Produces numb anesthesia across the cheek and upper jaw.
- Sympathetic Plexus Damage: The clot crushes the sympathetic nerves wrapped around the ICA, producing a classic Horner's syndrome (miosis/constricted pupil, ptosis, anhidrosis/lack of sweat on that side of the face).
- Bilateral Spread: Because the left and right cavernous sinuses are connected across the midline via intercavernous sinuses, 20–30% of cases will rapidly spread to involve the opposite eye.
Lethal Complications: If not aggressively treated with IV antibiotics and anticoagulation, CST leads to meningitis, brain abscesses, profound sepsis, permanent blindness, pituitary insufficiency (due to ischemia of the gland), and death.