Gross Anatomy of the Lungs and Pleura
By the conclusion of this exhaustive master guide, you will be deeply conversant with:
- The detailed anatomy of the Pleura and Pleural Cavities, including their recesses and embryological formation.
- The comprehensive gross anatomy of the Right and Left Lungs (lobes, fissures, surfaces, and borders).
- The vital neurovascular relations at the Root and Hilum of the lung, and adjacent mediastinal structures.
- The intricate branching of the Tracheobronchial Tree and the surgical significance of Bronchopulmonary Segments.
- The precise Surface Anatomy of the lungs and pleura (The "Rule of 6-8-10 / 8-10-12").
- High-yield clinical correlates including Thoracentesis, Bronchoscopy, Pleural Effusion, and TE Fistulas.
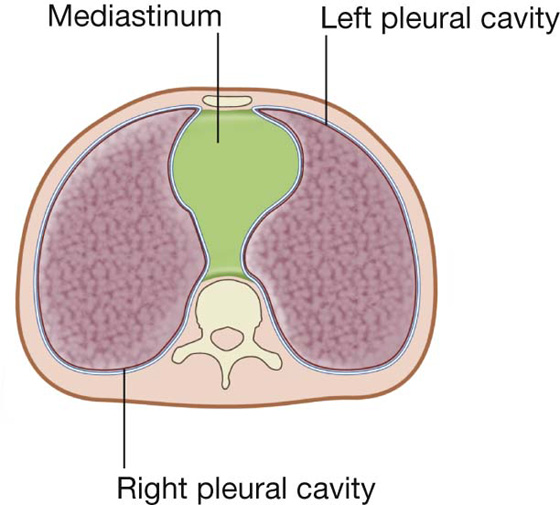
I. The Pleura and Pleural Cavities
The thoracic cavity contains two separate pleural cavities, one on either side of the centrally located Mediastinum. Each lung is independently enclosed within its own pleural cavity, ensuring that if one lung collapses (pneumothorax), the other remains functional.
1. The Two Layers of the Pleura
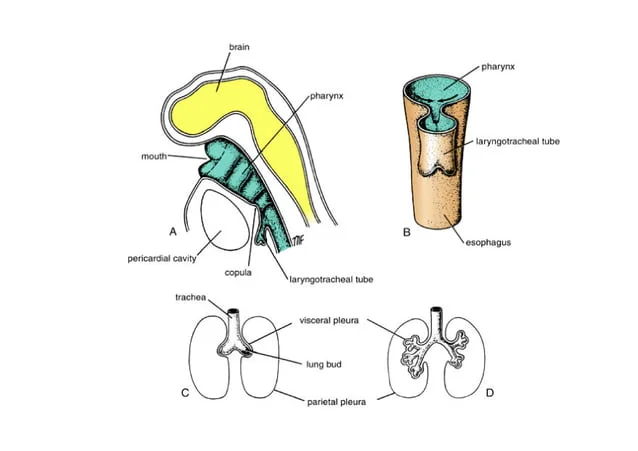
Each pleural cavity is completely lined by a continuous, serous mesothelial membrane called the Pleura. During embryological development, the growing lung bud punches into the coelomic cavity (like a fist pushing into a deflated balloon), creating two distinct layers:
- Parietal Pleura: The outer layer that intimately lines the inner surface of the thoracic wall, the superior surface of the diaphragm, and the lateral surface of the mediastinum.
- Visceral Pleura: The inner layer that directly and inextricably adheres to the outer surface of the lung, dipping deep into the fissures between the lobes.
The Reflection: The parietal pleura reflects (folds back upon itself) at the root of the lung to become continuous with the visceral pleura.
2. The Pleural Cavity (Pleural Space)
Under normal, healthy conditions, the pleural cavity is a potential space. The visceral and parietal pleura are in direct contact, separated only by a microscopic, capillary-thin layer of serous pleural fluid.
- Function of Fluid: It acts as a lubricant to allow the lungs to slide frictionlessly against the chest wall during breathing. Crucially, the surface tension of this fluid firmly holds the lung against the chest wall, preventing lung collapse.
3. Pleural Recesses
The lungs do not completely fill the pleural cavities, especially during quiet expiration. This leaves empty, potential spaces where two layers of parietal pleura touch each other. These are called recesses, and they only fill with lung tissue during deep, forced inspiration.
- Costodiaphragmatic Recess: The largest and clinically most important recess. It lies inferiorly in the trough between the costal (rib) wall and the dome of the diaphragm. Fluid (like blood or pus) preferentially pools here due to gravity when a patient is standing or sitting upright.
- Costomediastinal Recess: Located anteriorly, where the costal pleura folds back to become the mediastinal pleura, notably behind the sternum (associated with the cardiac notch of the left lung).
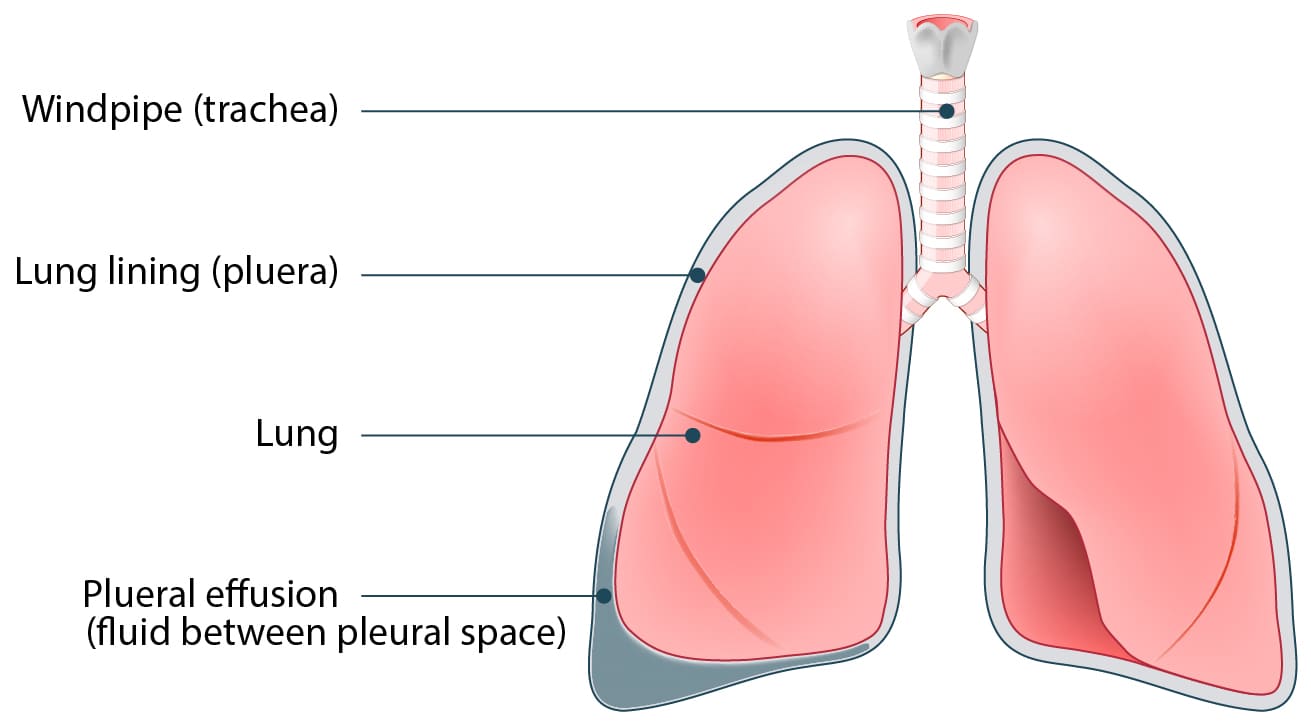
Clinical Correlate: Pleural Effusion
Pathology: A pleural effusion is the abnormal accumulation of excess fluid (serous fluid, blood, or pus) in the pleural cavity. Because the fluid takes up space, it physically compresses the underlying lung tissue.
Clinical Signs:
- Diminished or Absent Breath Sounds: The fluid blocks the acoustic transmission of air moving in the lungs.
- Collapsed Lung: The affected lung (e.g., right lung) collapses away from the chest wall.
- Tracheal Deviation: A massive effusion generates immense pressure, physically displacing the mediastinum and pushing the trachea toward the opposite, healthy side (e.g., trachea displaced to the left).
II. Gross Anatomy of the Lungs
The lungs are paired, spongy, highly elastic organs responsible for respiration. Each lung is shaped like a half-cone.
1. Defining Features
- The Apex: The blunt superior end. It projects above rib I and into the root of the neck (roughly 1 inch / 2.5 cm above the medial third of the clavicle). It is protected by the suprapleural membrane (Sibson's fascia), a thickening of the endothoracic fascia.
- The Base: The broad, concave inferior surface that rests directly upon the convex dome of the diaphragm.
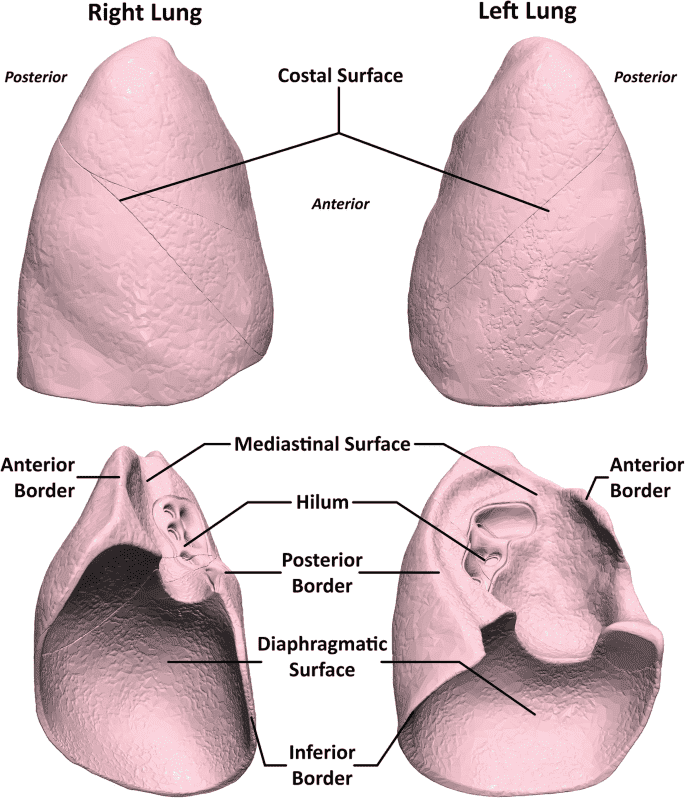
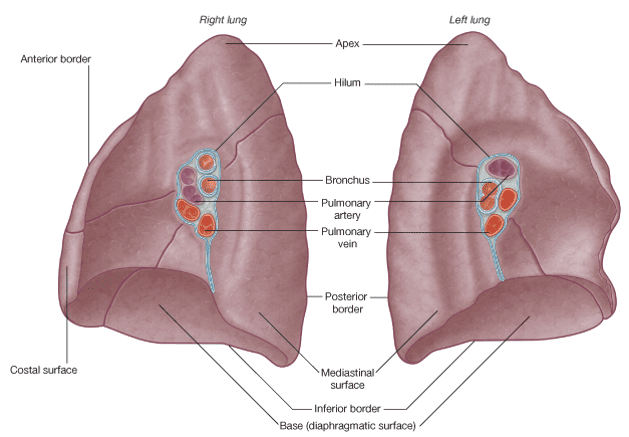
2. Surfaces and Borders
- Costal Surface: The large, smooth, convex surface lying immediately adjacent to the ribs and intercostal spaces.
- Mediastinal Surface: The medial surface facing the heart. It contains the comma-shaped Hilum (the doorway where structures enter and leave the lung).
- Inferior Border: Sharp and distinct; separates the base from the costal surface.
- Anterior Border: Sharp; separates the costal surface from the medial surface anteriorly.
- Posterior Border: Unlike the other borders, this is completely smooth and rounded, resting in the deep concavity beside the vertebral column.
3. Right vs. Left Lung: Key Anatomical Differences
The two lungs are not perfectly symmetrical. The heart, occupying the left side of the chest, severely alters the structure of the left lung.
| Feature | Right Lung | Left Lung |
|---|---|---|
| Size & Weight | Larger, heavier, and shorter (because the liver pushes the right hemidiaphragm up). | Smaller and narrower (due to the presence of the heart). |
| Lobes | Three (3): Superior, Middle, and Inferior lobes. | Two (2): Superior and Inferior lobes. |
| Fissures | Two (2): 1. Oblique Fissure. 2. Horizontal Fissure (separates superior from middle lobe). |
One (1): 1. Oblique Fissure only. |
| Unique Features | Relatively uniform anterior border. | Contains the Cardiac Notch (a deep indentation on the anterior border) and the Lingula (a tongue-like projection below the notch, homologous to the right middle lobe). |
III. The Root, Hilum, and Mediastinal Relations
The lung does not float freely; it remains firmly anchored to the mediastinum by its Root.
1. The Root and the Hilum
- The Root: A short, tubular collection of structures (airway, blood vessels, lymphatics, nerves) connecting the lung to the mediastinum.
- The Hilum: The actual geographical depression (the "doorway") on the mediastinal surface of the lung through which the root structures pass.
The Pulmonary Ligament: A thin, blade-like fold of pleura that projects inferiorly from the root. It provides dead space, allowing the pulmonary veins to distend comfortably when cardiac output increases during exercise.
The Nerves Around the Root
This is highly tested anatomical topography:
- The Phrenic Nerve (which innervates the diaphragm) passes immediately ANTERIOR to the root of the lung.
- The Vagus Nerve (Parasympathetic control) passes immediately POSTERIOR to the root of the lung.
Contents of the Hilum
Generally, the arrangement inside the hilum is standard:
- Pulmonary Artery: Superior.
- Pulmonary Veins (2): Inferior and anterior.
- Main Bronchus: Posterior.
*Right Lung Exception: On the right side, the superior lobar bronchus branches incredibly early (within the root itself). Thus, the bronchus sits superior to the pulmonary artery, earning the specific name Eparterial Bronchus.
2. Mediastinal Impressions (The Imprints on the Lungs)
Because the lungs are soft and spongy, the surrounding vital organs press firmly into their mediastinal surfaces, leaving distinct indentations visible on cadavers.
| Right Lung Impressions | Left Lung Impressions |
|---|---|
| The Heart: Right Atrium. | The Heart: Left Ventricle (creating a massive, deep cardiac impression). |
| Venous Systems: Superior Vena Cava (SVC) Inferior Vena Cava (IVC) Azygos Vein (Arches gracefully over the root of the right lung to join the SVC). |
Arterial Systems: Aortic Arch (Arches gracefully over the root of the left lung). Descending Thoracic Aorta. |
| Other Structures: Esophagus (lies behind the root). Right Subclavian Artery and Vein (arching over the cervical dome into the axilla). |
Other Structures: Esophagus. Left Subclavian Artery and Left Brachiocephalic Vein (arching over the cervical dome). |
IV. The Tracheobronchial Tree
The airway acts as an inverted tree, distributing air from the atmosphere deep into the microscopic alveolar sacs for gas exchange.
1. The Trachea
- A flexible tube originating at vertebral level C6 (lower neck).
- It descends into the mediastinum and physically bifurcates (splits) at vertebral level T4 (The Sternal Angle) into the right and left main bronchi. The internal ridge at this split is called the Carina.
- Structurally held open by 'C-shaped' transverse hyaline cartilage rings. The open 'C' faces posteriorly, filled entirely with the smooth Trachealis muscle, which yields to allow food to travel down the adjacent esophagus without obstruction.
2. Right vs. Left Main Bronchi
The anatomical difference between the main bronchi dictates the pathophysiology of foreign body aspiration.
- Right Main Bronchus: Wider in diameter, shorter in length, and takes a much more vertical course downwards.
- Left Main Bronchus: Narrower in diameter, longer, and takes a more horizontal course (because it must reach over the beating heart).
Foreign Body Aspiration
Because the right main bronchus is wider and acts almost as a direct vertical continuation of the trachea, inhaled foreign bodies (e.g., coins, peanuts, teeth) tend to lodge overwhelmingly on the RIGHT side rather than the left. Specifically, they often fall deep into the posterior basal segment of the right lower lobe.
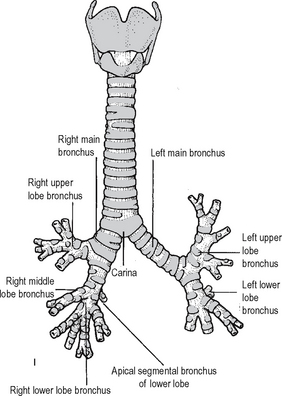
3. Bronchial Branching
The airways divide in a strict, highly organized hierarchy:
- Main (Primary) Bronchi: Enter the hilum.
- Lobar (Secondary) Bronchi: Supply each lobe. (3 on the right, 2 on the left).
- Segmental (Tertiary) Bronchi: Supply the bronchopulmonary segments.
- Bronchioles: Microscopic divisions. Crucial Histology Note: The walls of bronchi are held open by discontinuous plates of cartilage. However, cartilage is completely absent in bronchioles. Bronchioles rely entirely on thick layers of smooth muscle (which is the exact tissue that clamps shut during an Asthma attack).
- Terminal Bronchioles → Respiratory Bronchioles → Alveolar Ducts → Alveolar Sacs → Alveoli (where definitive gas exchange occurs).
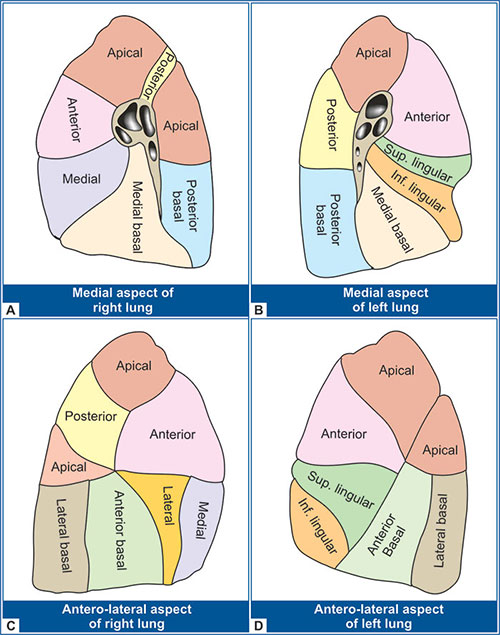
V. Bronchopulmonary Segments
A Bronchopulmonary Segment is the area of lung supplied by a specific segmental (tertiary) bronchus and its accompanying pulmonary artery branch. They are heavily tested and highly relevant for thoracic surgeons.
Defining Characteristics
- Shape: Shaped like an irregular pyramid or cone. The apex points toward the root of the lung, and the base projects peripherally onto the pleural surface.
- Vascular Supply: The segmental bronchus and the pulmonary artery run centrally through the core of the segment. However, the Pulmonary Veins run intersegmentally (in the connective tissue margins between the segments). The veins act as natural surgical boundaries.
- Clinical Significance: A bronchopulmonary segment is the smallest functionally independent region of a lung. Therefore, if a patient has a localized tumor or abscess, a surgeon can isolate and cleanly remove just that single affected segment (a Segmentectomy) without affecting the blood or air supply to any adjacent, healthy lung tissue.
Nomenclature of the Segments
There are typically ten (10) segments in each lung, though some fuse in the left lung due to its smaller size.
- Superior Lobe: Apical, Posterior, Anterior.
- Middle Lobe: Lateral, Medial.
- Inferior Lobe: Superior, Medial basal, Anterior basal, Lateral basal, Posterior basal.
- Superior Lobe: Apicoposterior (fused), Anterior, Superior lingular, Inferior lingular.
- Inferior Lobe: Superior, Anteromedial basal (fused), Lateral basal, Posterior basal.
VI. Blood Supply, Lymphatics, and Innervation
1. The Dual Blood Supply of the Lungs
The lungs have a unique, dual vascular system serving two entirely different purposes.
A. Pulmonary Circulation (For Gas Exchange)
- Carries deoxygenated blood from the right ventricle via the Pulmonary Trunk into the Left and Right Pulmonary Arteries.
- Gas exchange occurs at the alveolar capillary beds.
- Freshly oxygenated blood returns to the left atrium of the heart via the Pulmonary Veins (typically two veins per lung).
B. Bronchial Circulation (For Nutrition)
- This is the systemic "nutritive" vascular system that physically keeps the lung tissue alive. It supplies highly oxygenated blood to the bronchial walls, glands, large vessels, and the visceral pleura.
- Arterial Origin:
- Right Bronchial Artery: Usually a single artery arising from the third posterior intercostal artery (or occasionally from the upper left bronchial artery).
- Left Bronchial Arteries: Usually two arteries arising directly from the anterior surface of the descending thoracic aorta.
- Venous Drainage: The bronchial veins drain into the Azygos vein (on the right) and the Hemiazygos / Superior Intercostal vein (on the left). Some deep bronchial drainage empties directly into the pulmonary veins, mixing slightly deoxygenated blood with freshly oxygenated blood before returning to the heart.
2. Innervation of the Lungs
The lungs are innervated by the Autonomic Nervous System via the Anterior and Posterior Pulmonary Plexuses, located around the tracheal bifurcation and lung roots.
- Parasympathetic (Vagus Nerve): Stimulates bronchoconstriction, highly increases glandular mucus secretion (secretomotor), and causes vasodilation of pulmonary vessels.
- Sympathetic (Sympathetic Trunk): Stimulates massive bronchodilation (relaxes airways), inhibits glandular secretion, and causes vasoconstriction.
3. Lymphatic Drainage
Lymphatic fluid from the lungs is drained via superficial (subpleural) and deep plexuses. The progression of lymph flow is sequential:
Pulmonary Nodes → Bronchopulmonary (Hilar) Nodes → Tracheobronchial (Carinal) Nodes → Paratracheal Nodes → Bronchomediastinal Trunks (which finally empty into the Subclavian Veins).
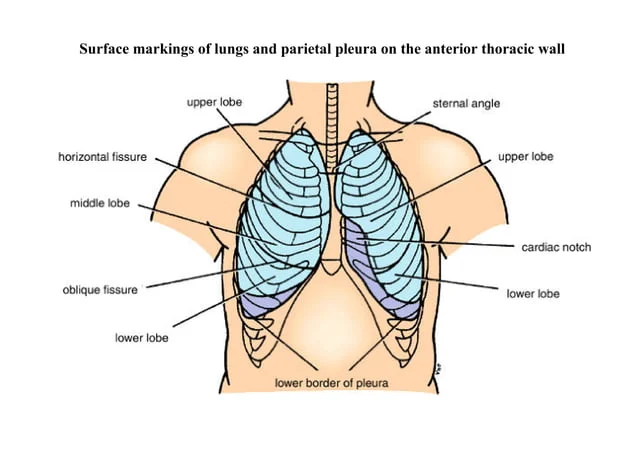
VII. Surface Anatomy: Mapping the Lungs on the Chest Wall
Physicians must memorize exactly where the invisible lungs and pleural cavities lie beneath the skin for safe clinical examination (auscultation, percussion) and surgical procedures (needle taps).
1. The Apices and Anterior Borders
- Apex: Projects roughly 1 inch (2.5 cm) above the medial third of the clavicle into the neck.
- Right Anterior Border: Runs directly downward behind the sternoclavicular joint, meeting the midline at the sternal angle, and continues straight down until the xiphisternal joint (6th costal cartilage).
- Left Anterior Border: Has a similar initial course, but at the level of the 4th costal cartilage, it aggressively deviates laterally to form the Cardiac Notch, continuing down to the 6th rib.
2. The Inferior Borders: "The Rule of 6, 8, 10 / 8, 10, 12"
The inferior border of the lung rests higher than the inferior border of the parietal pleura (creating the empty costodiaphragmatic recess). You must memorize these descending anatomical lines:
| Anatomical Landmark Line | Inferior Border of LUNG | Inferior Border of PLEURA |
|---|---|---|
| Midclavicular Line (Anterior) | Rib 6 | Rib 8 |
| Midaxillary Line (Lateral/Armpit) | Rib 8 | Rib 10 |
| Paravertebral/Scapular Line (Posterior) | Rib 10 (Vertebra T10) | Rib 12 (Vertebra T12) |
The difference between these two lines exactly represents the depth of the Costodiaphragmatic Recess.
3. Surface Markings of the Fissures
- Oblique Fissure (Both Lungs): Marked by drawing a line from the spinous process of T3 or T4 posteriorly, sloping downwards and laterally, crossing the 5th intercostal space at the midaxillary line, and ending anteriorly at the 6th costochondral junction.
- Horizontal Fissure (Right Lung Only): Marked by drawing a horizontal line starting anteriorly at the 4th costal cartilage, wrapping laterally to meet the oblique fissure in the midaxillary line.
VIII. Clinical & Embryological Correlates
Thoracentesis (Pleural Tap)
To safely drain a pleural effusion, a needle is inserted into the 8th or 9th intercostal space in the midaxillary line (safely targeting the costodiaphragmatic recess without hitting the lung). Crucial anatomical rule: The needle must be inserted immediately SUPERIOR to the lower rib to avoid severing the intercostal Vein, Artery, and Nerve (VAN) which hide in the costal groove on the inferior margin of the upper rib.
Structures pierced by the needle:
Skin → Superficial fascia → Serratus anterior muscle → External Intercostal muscle → Internal Intercostal muscle → Innermost Intercostal muscle → Endothoracic fascia → Parietal pleura.
Bronchoscopy
Patients with endobronchial lesions (tumors) undergo bronchoscopic evaluation. The flexible tube passes: Nose → Oropharynx → Vocal Cords → Trachea → Carina.
Pathology sign: A widened, flattened, or distorted Carina on bronchoscopy is a terrifying clinical sign. It strongly indicates that the Tracheobronchial (subcarinal) lymph nodes—located immediately beneath the bifurcation—are massively enlarged, usually due to metastatic lung cancer pushing upward against the airway.
Tracheoesophageal Fistulas (TEF)
During embryogenesis, the respiratory system grows out of the foregut. A common tube (the laryngotracheal tube) must perfectly separate from the esophagus via a septum. If this separation fails, the baby is born with a Tracheoesophageal Fistula (an abnormal connection between the windpipe and stomach tube). When the newborn attempts to feed, milk pours directly into the lungs, causing immediate, catastrophic choking and severe aspiration pneumonia. It requires emergency surgical repair.
The Mechanics of Respiration
To inhale, the thorax must expand to drop intrathoracic pressure, sucking air in. The thoracic cage expands in three highly distinct dimensions simultaneously:
- Anteroposterior Expansion (The Pump-Handle): Contraction of muscles lifts the sternum upward and outward, like a water pump handle. Driven by the upper ribs.
- Lateral Expansion (The Bucket-Handle): The middle and lower ribs swing outward and upward laterally, exactly like lifting the curved handle of a bucket.
- Vertical Expansion: The dome-shaped diaphragm aggressively contracts and descends downward into the abdomen, massive elongating the vertical axis of the thoracic cavity.
IX. References and Recommended Reading
- Drake, R. L., Vogl, A. W., & Mitchell, A. W. M. Gray's Anatomy for Students (Current Edition). Elsevier / Student Consult. (Primary source for all anatomical diagrams, pleural reflections, and surface anatomy referenced herein).
- Moore, K. L., Dalley, A. F., & Agur, A. M. R. Clinically Oriented Anatomy. Lippincott Williams & Wilkins. (Excellent clinical correlates regarding thoracentesis pathways and bronchopulmonary segmentectomies).
- Netter, F. H. Atlas of Human Anatomy. Elsevier. (Gold standard for visualizing hilar structures and mediastinal impressions).