The Mediastinum: Anatomy, Contents, and Clinical Topography
By the conclusion of this exhaustive anatomical master guide, you will be deeply conversant with:
- The comprehensive 3D boundaries and subdivisions of the Mediastinum.
- The exact contents (vascular, nervous, lymphatic, and visceral) of the Superior, Anterior, Middle, and Posterior Mediastinum.
- The cross-sectional topography at the T4 level (Sternal Angle / Angle of Louis) and its immense clinical significance.
- The fascial planes of the neck and how they dictate the spread of Mediastinitis.
- The pathophysiology of Mediastinal Syndrome, Mediastinal Shift, and Mediastinal Widening.
I. Introduction and General Boundaries
The Mediastinum (from Latin mediastinus, meaning "midway") is the thick, flexible, and highly dynamic central partition of the thoracic cavity. It is a broad, central compartment that completely separates the two lateral pleural cavities (which house the lungs).
It acts as the major conduit for structures passing between the neck, the thorax, and the abdomen. Because it contains vital hollow organs, massive pressurized blood vessels, and loose connective tissue, it is highly mobile, accommodating the volumetric changes of the lungs during respiration and the beating of the heart.

General Boundaries of the Entire Mediastinum:
- Anteriorly: The sternum and costal cartilages.
- Posteriorly: The bodies of the 12 thoracic vertebrae (T1 to T12).
- Laterally (Sides): The mediastinal parietal pleura (which reflects over the medial surfaces of the lungs).
- Superiorly: The superior thoracic aperture (thoracic inlet), continuous with the fascial planes of the neck.
- Inferiorly: The diaphragm.
II. Divisions of the Mediastinum: The Sternal Angle
For anatomical and surgical clarity, the mediastinum is divided into distinct compartments by a highly significant imaginary plane called the Transverse Thoracic Plane.
This imaginary horizontal line passes from the Sternal Angle (Angle of Louis) anteriorly to the intervertebral disc between T4 and T5 posteriorly.
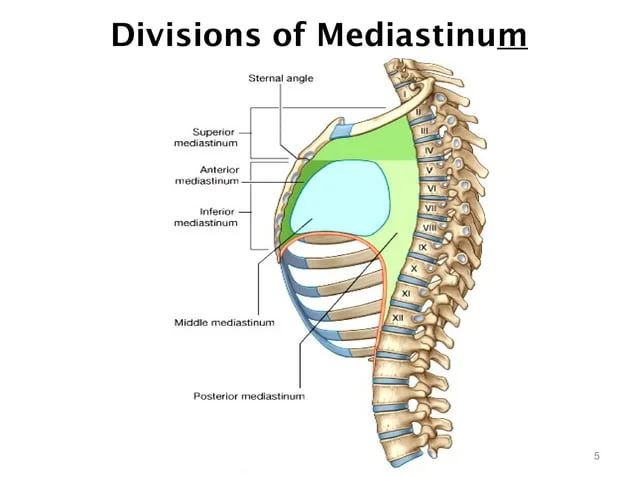
The Magic of the Sternal Angle (T4/T5 Plane)
This plane is arguably the most tested and clinically relevant landmark in thoracic anatomy. It dictates the division of the mediastinum into:
- Superior Mediastinum: Everything ABOVE the plane.
- Inferior Mediastinum: Everything BELOW the plane. The Inferior Mediastinum is further massively subdivided by the pericardial sac (the heart) into:
- Anterior Mediastinum: In front of the pericardium.
- Middle Mediastinum: The pericardium and its contents.
- Posterior Mediastinum: Behind the pericardium.
III. The Superior Mediastinum
This compartment lies deep to the manubrium of the sternum and contains the massive "great vessels" that exit and enter the heart, as well as critical nerves descending from the brain.
Boundaries:
- Anterior: Manubrium sterni (posterior surface).
- Posterior: The bodies of the first four thoracic vertebrae (T1 to T4).
- Sides (Lateral): Mediastinal pleura of the right and left lungs.
- Superior: The plane of the thoracic inlet (root of the neck).
- Inferior: The imaginary transverse thoracic plane (joining the sternal angle to the lower border of T4).
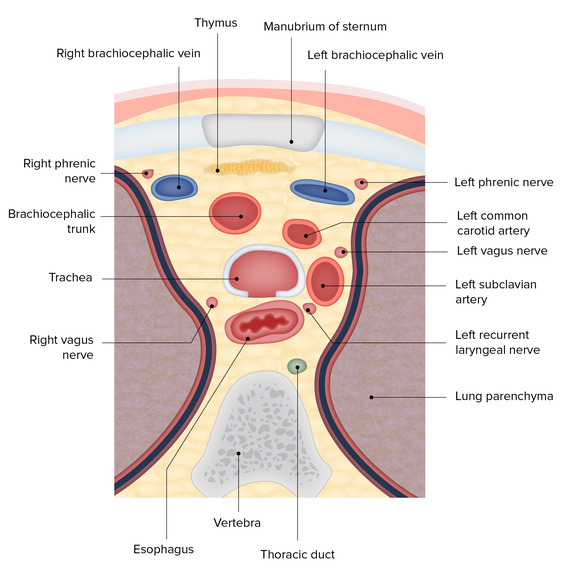
Contents of the Superior Mediastinum:
The contents are densely packed and are classically arranged in layers from anterior to posterior (Muscles/Glands → Veins → Arteries → Airways → GI Tract).
- Muscles: The origins of the infrahyoid "strap" muscles: Sternohyoid and Sternothyroid. The inferior attachments of the Longus colli muscles.
- Thymus: The lower portion of the thymus gland (highly prominent in childhood and puberty, slowly replaced by fat in adults).
- Superior Vena Cava (SVC): The upper half of the SVC resides here before entering the pericardium.
- Brachiocephalic Veins: Both the Right and Left Brachiocephalic veins (the left is much longer and crosses anterior to the major arteries).
- Left Superior Intercostal Vein: Drains the 2nd, 3rd, and 4th intercostal spaces.
- Arch of the Aorta: Curves backward over the left main bronchus.
- Brachiocephalic Artery (Trunk): The first branch of the aortic arch.
- Left Common Carotid Artery: The second branch.
- Left Subclavian Artery: The third branch.
- Trachea: Lies anterior to the esophagus, bifurcating at the very bottom of this compartment.
- Esophagus: The most posterior hollow tube, lying flat against the vertebral bodies.
- Nerves: Both Vagus Nerves (CN X), both Phrenic Nerves (C3-C5), Cardiac Nerves.
- Left Recurrent Laryngeal Nerve: A critical branch of the left vagus that hooks completely under the arch of the aorta, ascending back up in the groove between the trachea and esophagus.
- Thoracic Duct: The massive lymphatic vessel lying on the left side of the esophagus.
- Lymph Nodes: Brachiocephalic and Tracheobronchial nodes.
IV. The Inferior Mediastinum: Anterior, Middle, and Posterior
The Inferior Mediastinum extends from the transverse thoracic plane down to the diaphragm. The presence of the heart and its tough fibrous sac (the pericardium) acts as a physical barrier, dividing this vast space into three highly distinct zones.
A. The Anterior Mediastinum (The Narrowest Compartment)
This is a remarkably shallow space squeezed between the sternum and the heart.
- Boundaries:
- Anterior: Body of the sternum.
- Posterior: Pericardium (enclosing the heart).
- Sides: Mediastinal pleura.
- Superior: Imaginary plane (Sternal angle).
- Inferior: Diaphragm.
- Contents:
- Thymus: (The lower pole extending down in children/infants).
- Sternopericardial Ligaments: Tough fibrous bands that physically anchor the pericardium to the posterior aspect of the sternum, keeping the heart in place.
- Internal Thoracic Artery & Branches: (Also known as the Internal Mammary Artery, heavily used in coronary bypass surgeries).
- Lymphatics & Lymph nodes: Prepericardial lymph nodes.
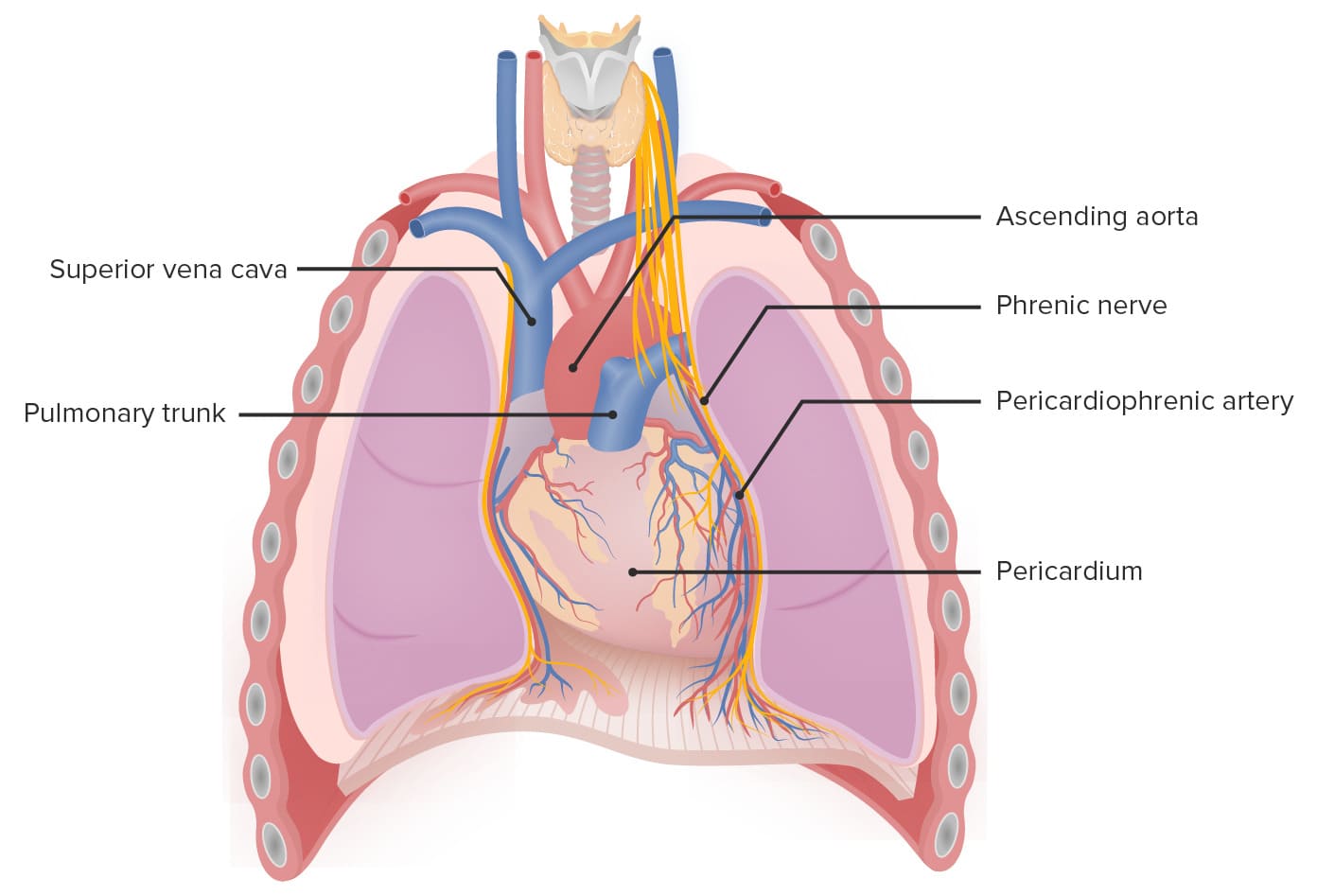
B. The Middle Mediastinum
This is the central, most vital compartment of the entire thoracic cavity. It is dominated entirely by the heart and the very beginnings of the great vessels.
- Boundaries: It is defined simply as the pericardial sac and everything contained within it, extending slightly upward to encompass the roots of the great vessels.
- Contents:
- Heart enclosed in the Pericardium.
- Arteries: Ascending Aorta (the very first segment before the arch), Pulmonary trunk with its Left & Right branches.
- Veins: Lower half of the Superior Vena Cava (SVC), the Termination (arch) of the Azygos vein as it dumps into the SVC, and the Pulmonary veins entering the left atrium.
- Nerves: Phrenic nerves (which uniquely run directly over the lateral surface of the pericardium) and the Deep Cardiac Plexus.
- Airways: The Bifurcation of the Trachea (the Carina) separating into the two principal (mainstem) bronchi.
- Lymphatics: Tracheobronchial lymph nodes (often enlarged in lung cancer and tuberculosis).
C. The Posterior Mediastinum
This is a deep, vertical passageway located right in front of the spine. It provides a safe corridor for structures traveling between the thorax and the abdomen.
- Boundaries:
- Anterior: Posterior surface of the Pericardium and the Bifurcation of the trachea.
- Posterior: Bodies of the thoracic vertebrae (T5 to T12).
- Superior: Transverse thoracic plane.
- Inferior: Diaphragm.
- Sides: Mediastinal pleura.
- Contents:
- Oesophagus (Esophagus): Descends directly behind the left atrium of the heart.
- Arteries: Descending Thoracic Aorta with its multiple branches (posterior intercostal, esophageal, bronchial, and superior phrenic arteries).
- Veins: The Azygos venous system. The Azygos vein runs on the right side of the vertebral column. The Hemiazygos and Accessory Hemiazygos veins run on the left.
- Nerves: Both Vagus nerves (which break apart to form the esophageal plexus) and the Splanchnic nerves (Greater, Lesser, and Least, which carry sympathetic fibers down to the abdomen).
- Thoracic Duct: The largest lymphatic vessel in the body, ascending between the aorta and the azygos vein.
- Lymph nodes: Posterior mediastinal lymph nodes.
V. Applied Clinical Anatomy of the Mediastinum
Because the mediastinum is a packed compartment continuous with the neck, diseases (like infections or tumors) can spread rapidly and cause devastating compression syndromes.
Mediastinitis: The Spread of Deep Neck Infections
Mediastinitis is a life-threatening inflammation or severe bacterial infection of the connective tissues in the mediastinum. Because the deep cervical fascia of the neck extends directly down into the thorax, dental abscesses or severe throat infections can track downward with gravity into the chest.
The spread depends entirely on the specific fascial layer involved:
- Infections deep to the Prevertebral Fascia: Pus traveling under the prevertebral fascia will only reach down to T4. It cannot go beyond this point because the prevertebral fascia firmly anchors and attaches to the bone at the T4 vertebral level.
- Infections in the Pretracheal Space: Pus traveling in front of the pretracheal fascia (anteriorly) will seep directly down into the Anterior Mediastinum.
- The Danger Space (Retropharyngeal Space): Pus traveling between the pretracheal (visceral) fascia and the prevertebral fascia. This space is entirely open all the way down. Infection here will seep straight through the superior mediastinum and violently pour into the Posterior Mediastinum. This causes acute, lethal Descending Necrotizing Mediastinitis.
[Image inserted here: Sagittal diagram showing the Investing layer, Pretracheal fascia, and Prevertebral fascia acting as conduits for infection from the neck into the mediastinum]

Mediastinal Syndrome (Compression Syndrome)
Because the mediastinum is a rigid "box" bordered by the spine and sternum, any growing mass (like a massive lymphoma, an aortic aneurysm, or a bronchogenic carcinoma/lung cancer tumor) will aggressively crush the soft structures inside. This produces a cluster of severe symptoms known as Mediastinal Syndrome:
- Engorgement of veins: Compression of the Superior Vena Cava (SVC Syndrome) stops blood from draining from the head. Result: Severe facial swelling, blue lips, and violently distended jugular veins in the neck.
- Dyspnea (Difficulty breathing): Physical compression crushing the soft trachea or major bronchi.
- Dysphagia (Difficulty swallowing): Physical compression crushing the muscular esophagus against the spine.
- Hoarseness of voice: The most highly tested exam presentation! A tumor in the superior mediastinum will crush the Left Recurrent Laryngeal Nerve as it hooks under the aortic arch, paralyzing the left vocal cord and causing a raspy, hoarse voice.
Mediastinal Widening
When a physician looks at a PA Chest X-ray, the central white shadow is the mediastinum. If this shadow is vastly enlarged, it is termed Mediastinal Widening.
Common Causes: Massive hemorrhage from a traumatic car crash (aorta rupture), a dissecting aortic aneurysm expanding like a balloon, massive lymph node swelling from Hodgkin's Lymphoma, or inhalation of Anthrax spores (causing hemorrhagic mediastinitis).
Mediastinal Shift
The mediastinum is mobile. It can be pushed or pulled out of the midline, a condition called Mediastinal Shift.
- Pushed AWAY from the lesion: A massive buildup of high-pressure air (Tension Pneumothorax) or massive fluid (Pleural Effusion) in one lung acts like a battering ram, violently shoving the heart and trachea into the opposite, healthy side.
- Pulled TOWARDS the lesion: If a lung completely deflates and collapses (Atelectasis) or is surgically removed, the vacuum created physically sucks the mediastinum over to fill the empty space.
[Image inserted here: Chest X-Ray and diagram showing Mediastinal Widening and Mediastinal Shift due to unilateral pressure changes]

VI. References & Recommended Reading
- Moore, K. L., Dalley, A. F., & Agur, A. M. R. (2014). Clinically Oriented Anatomy (7th ed.). Lippincott Williams & Wilkins. (Definitive guide on mediastinal compartments and fascial plane infections).
- Standring, S. (2015). Gray's Anatomy: The Anatomical Basis of Clinical Practice (41st ed.). Elsevier. (In-depth analysis of the superior mediastinum neurovascular relationships).
- Netter, F. H. (2014). Atlas of Human Anatomy (6th ed.). Saunders. (Unparalleled visual plates for the Cross-Section at T4 and Mediastinal Shift).
- Drake, R., Vogl, A. W., & Mitchell, A. W. M. (2019). Gray's Anatomy for Students (4th ed.). Elsevier. (Excellent clinical correlates regarding Mediastinal Syndrome and Hoarseness).