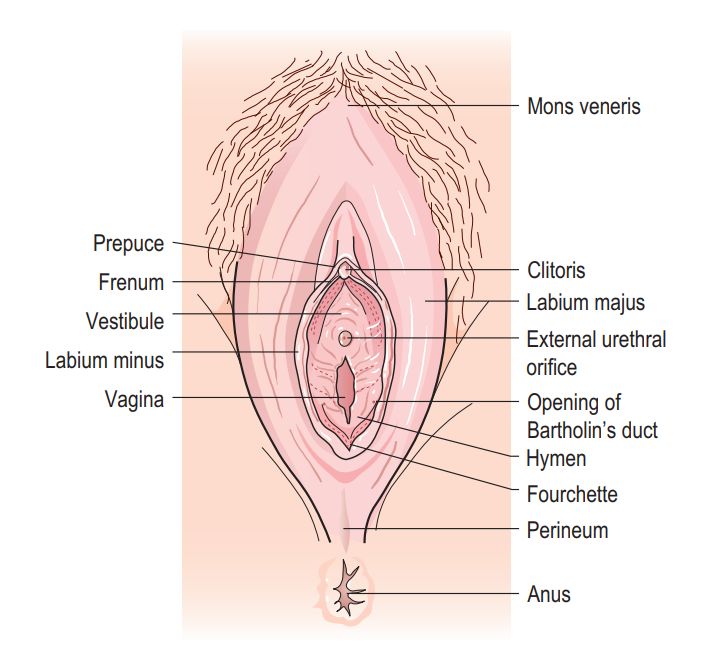
Female External Genitalia (Vulva)
The female external genitalia, collectively known as the vulva (or pudendum), encompass all the visible structures that extend from the pubic region to the perineum. These structures protect the internal reproductive organs, play a role in sexual arousal and function, and contain the openings of the urethra and vagina.
The vulva is composed of the following main structures:
- Mons Pubis (Mons Veneris)
- Labia Majora
- Labia Minora
- Clitoris
- Vestibule
- Urethral Orifice
- Vaginal Orifice
- Greater Vestibular Glands (Bartholin's Glands) (and Lesser Vestibular Glands)
1. Mons Pubis (Mons Veneris)
- Description: A rounded, fleshy prominence composed of adipose tissue (fat pad) overlying the pubic symphysis (the joint between the two pubic bones).
- Location: Anterior to the labia majora and superior to the clitoris.
- Covering: After puberty, it becomes covered with pubic hair.
- Hair Pattern:
- Female Pattern: Typically forms an inverted triangle, with a horizontal upper border (concave or convex downwards).
- Male Pattern: Tends to be diamond-shaped, extending upwards towards the umbilicus.
- Clinical Relevance: A change in female hair pattern towards a masculine distribution (hirsutism) can indicate underlying hormonal imbalances (e.g., polycystic ovary syndrome, adrenal disorders) and may be associated with infertility or other endocrine issues.
- Function: Acts as a protective cushion over the pubic bone during sexual intercourse.
2. Labia Majora
- Description: Two prominent, longitudinal, fleshy folds of skin that extend downwards and backwards from the mons pubis. They are homologous to the scrotum in males.
- Composition: Primarily composed of fat, elastic tissue, and some smooth muscle. Their outer surface is covered with pubic hair after puberty, while the inner surface is hairless and smooth.
- Extension: They unite anteriorly at the mons pubis and posteriorly, they tend to merge into the perineum, often forming a posterior commissure anterior to the anal canal.
- Erectile Tissue: The tissue within the labia majora is non-erectile.
- Function: Act as a protective barrier, enclosing and safeguarding the more delicate internal structures of the vulva (labia minora, clitoris, and vestibule).
3. Labia Minora (Nymphae)
- Description: Two smaller, hairless folds of highly vascularized, reddish-pink skin located medial to the labia majora. They are homologous to the ventral aspect of the penis in males.
- Composition: Rich in erectile tissue, blood vessels, nerve endings, and sebaceous glands, giving them a rich sensory innervation.
- Anatomical Configuration:
- Anteriorly: Each labium minus splits into two folds:
- Medial Fold: Passes over the clitoris to form the frenulum of the clitoris on its undersurface.
- Lateral Fold: Passes over the clitoris to form the prepuce (hood) of the clitoris on its dorsal surface.
- Posteriorly: In nulliparous (never given birth) women, the labia minora may fuse to form a transverse fold called the fourchette anterior to the vaginal opening. This often disappears after childbirth.
- Anteriorly: Each labium minus splits into two folds:
- Erectile Tissue: The labia minora contain erectile tissue, and they engorge with blood during sexual arousal.
- Function:
- Sexual Arousal: Highly sensitive due to rich nerve supply, contributing significantly to sexual pleasure. They swell and darken during arousal.
- Protection: Further protect the urethral and vaginal orifices.
- Lubrication: Contain numerous sebaceous glands for lubrication.
- Surgical Use: The tissue's elasticity and rich blood supply make it suitable for grafting, particularly in reconstructive surgery (e.g., for facial wounds, though this is a specialized application and not its primary function).
4. Clitoris
- Description: A highly sensitive organ composed of erectile tissue, homologous to the penis in males. It is the primary organ for sexual pleasure in females.
- Location: Located anteriorly, where the labia minora converge.
- Structure:
- Fixed Root: Attached to the pubic arch. Composed of three masses of erectile tissue:
- Crura (Corpora Cavernosa): Two crura, continuous with the corpora cavernosa of the body of the clitoris, attach to the pubic rami and are covered by the ischiocavernosus muscles.
- Bulbs of the Vestibule (Corpus Spongiosum): Two masses of erectile tissue, located on either side of the vaginal orifice (split in females due to the presence of the vagina), covered by the bulbospongiosus muscles. These merge anteriorly to form the body of the clitoris.
- Free Body: Protrudes externally, composed of two corpora cavernosa and a small amount of corpus spongiosum (which forms the glans).
- Glans Clitoris: The most external, highly sensitive, pea-sized tip of the clitoris.
- Coverings: Covered by the prepuce (hood) and frenulum, formed by the labia minora.
- Fixed Root: Attached to the pubic arch. Composed of three masses of erectile tissue:
- Erection Mechanism (Similar to penis):
- Psychic and Tactile Stimulation: Pleasurable sights, sounds, smells, and touch (nipples, inner thighs, clitoris itself) trigger a parasympathetic discharge from the sacral spinal cord segments (S2, S3, S4).
- Vasodilation: This leads to the release of nitric oxide, causing vasodilation of arteries supplying the erectile tissue (corpora cavernosa and bulbs of vestibule).
- Engorgement: Increased blood flow rapidly fills the vascular spaces within the erectile tissue.
- Venous Occlusion: The engorged erectile tissue compresses the veins draining the clitoris against the surrounding tough fibrous capsule (tunica albuginea) and pelvic bones, retarding venous outflow.
- Erection: The combination of increased arterial inflow and decreased venous outflow leads to engorgement and rigidity of the clitoris.
- Function: Solely dedicated to sexual sensation and arousal.
5. Vestibule
- Description: The almond-shaped space or cleft enclosed by the labia minora.
- Boundaries:
- Laterally: Labia minora.
- Anteriorly: Clitoris.
- Posteriorly: Fourchette (if present) or posterior commissure.
- Contents/Openings: It contains the openings of several important structures:
- Urethral Orifice
- Vaginal Orifice
- Ducts of the Greater Vestibular Glands (Bartholin's Glands)
- Ducts of the Lesser Vestibular Glands (Skene's Glands/Paraurethral Glands): These small mucus-secreting glands are located around the urethral orifice.
6. Urethral Orifice (External Urethral Meatus)
- Description: The opening of the female urethra.
- Location: Located posterior to the clitoris and anterior to the vaginal orifice, typically about 2.5 cm below the clitoris. It often appears as a small, slit-like or star-shaped opening.
- Function: Serves as the sole passage for urine in females.
- Clinical Relevance:
- Infections: Its short length (about 4 cm, much shorter than in males) and close proximity to the anal canal and vaginal opening make females more susceptible to recurrent urinary tract infections (UTIs), as bacteria can easily ascend into the bladder.
- Trauma: Can be traumatized during sexual intercourse or childbirth.
- Obstruction: Infections like Herpes Simplex Virus (HSV) can cause severe pain and swelling, potentially leading to dysuria or acute urinary retention if the orifice is obstructed.
7. Vaginal Orifice (Introitus)
- Description: The external opening of the vagina, located posterior to the urethral orifice and anterior to the anus.
- Covering: In virgins, it is typically partially covered by the hymen.
- Hymen:
- Description: A thin, vascularized mucous membrane that partially occludes the vaginal opening. Its shape and thickness vary widely among individuals.
- Breakage: It often ruptures or stretches during first sexual intercourse or due to other activities (e.g., tampon insertion, vigorous exercise). Remnants after rupture are called hymenal tags.
- Clinical Significance: The absence of an intact hymen is NOT a reliable indicator of non-virginity, as it can be broken by non-coital activities or may be naturally absent/very thin.
- Imperforate Hymen: A congenital condition where the hymen completely blocks the vaginal opening.
- Clinical Relevance: Can lead to menstrual blood retention (hematocolpos) at menarche, causing severe lower abdominal pain, absence of menstruation (primary amenorrhea), and a bulging bluish mass visible at the introitus. Requires surgical incision (hymenotomy) to allow drainage.
8. Greater Vestibular Glands (Bartholin's Glands)
- Description: Two small, pea-sized glands, homologous to the bulbourethral glands in males.
- Location: Located on each side of the vaginal orifice, embedded within the posterior aspect of the labia majora.
- Ducts: Their ducts open into the vestibule, specifically between the labia minora and the hymen (or its remnants), usually at the 4 o'clock and 8 o'clock positions relative to the vaginal opening.
- Function: Produce a clear, mucus-like secretion during sexual arousal to lubricate the vestibule and vaginal opening, facilitating intercourse.
- Clinical Relevance: Can become blocked, leading to a Bartholin's cyst (painless swelling) or, if infected, a Bartholin's abscess (painful, inflamed, pus-filled swelling).
Lesser Vestibular Glands (Skene's Glands / Paraurethral Glands)
- Description: Numerous small mucous glands that open into the vestibule, mainly around the urethral orifice. Homologous to the prostate gland in males.
- Function: Produce mucus that lubricates the urethral opening and vestibule. Some researchers believe they contribute to "female ejaculation."
- Clinical Relevance: Can become infected, leading to Skene's gland cysts or abscesses.
Blood Supply, Venous Drainage, and Lymphatics of the Vulva
- Arterial Supply: Primarily from branches of the internal pudendal artery and external pudendal artery.
- Clitoris: Specific branches include the deep arteries of the clitoris, artery of the bulb of the vestibule, and dorsal artery of the clitoris (all branches of the internal pudendal artery).
- Rest of the Vulva: Supplied by labial branches of both internal and external pudendal arteries.
- Venous Drainage: Venous plexuses drain into the internal pudendal veins and external pudendal veins, which then drain into the internal iliac veins and femoral veins, respectively.
- Lymphatic Drainage:
- Lymph from the skin and superficial structures of the vulva (mons pubis, labia majora, labia minora, clitoris, vestibule) drains predominantly to the superficial inguinal lymph nodes (specifically the medial group).
- Lymph from the deeper parts of the clitoris may also drain to the deep inguinal and even internal iliac lymph nodes.
- Innervation:
- Pudendal Nerve (S2-S4): Provides most of the somatic (sensory and motor) innervation to the vulva. Its branches include the dorsal nerve of the clitoris, labial nerves, and perineal nerves.
- Ilioinguinal Nerve (L1): Provides sensory innervation to the anterior labia majora and mons pubis.
- Genital Branch of Genitofemoral Nerve (L1-L2): Provides sensory innervation to the anterior labia majora.
Common Clinical Conditions of the Vulva
The vulva, being external and exposed, is susceptible to a variety of conditions, including infections, inflammatory disorders, structural anomalies, and neoplastic changes. These conditions can cause discomfort, pain, itching, and impact sexual health and quality of life.
1. Pubic Lice (Pthirus Pubis, "Crabs")
- Description: An infestation of the pubic hair and surrounding coarse body hair (e.g., perineum, thighs, eyelashes, axilla) by the parasitic insect Pthirus pubis.
- Transmission: Primarily through close physical contact, most commonly sexual contact. Can also be spread through infested clothing, bedding, or towels.
- Clinical Features:
- Intense pruritus (itching): Especially at night, caused by an allergic reaction to the louse's saliva.
- Maculae caeruleae ("blue spots"): Small, bluish-gray spots on the skin where lice have fed, caused by anticoagulant in the louse's saliva.
- Visible nits (eggs): Small, oval, whitish-yellow eggs firmly attached to the hair shafts, close to the skin.
- Adult lice: Tiny (2-3 mm), crab-shaped insects that are difficult to see with the naked eye but may be spotted clinging to hairs.
- Excoriations: Skin damage from scratching, which can lead to secondary bacterial infections.
- Diagnosis: Visual identification of nits, nymphs, or adult lice.
- Treatment:
- Topical Insecticides: Permethrin (1% cream rinse), pyrethrins with piperonyl butoxide. Apply to affected areas, leave for recommended time, then wash off. Repeat in 7-10 days to kill newly hatched lice.
- Hygiene: Wash all clothing, bedding, and towels in hot water and dry on high heat, or dry clean. Items that cannot be washed should be sealed in plastic bags for two weeks.
- Treatment of Sexual Partners: All recent sexual contacts should be treated simultaneously.
- Combing: Fine-toothed combs can help remove nits.
2. Bartholin's Cyst
- Description: A fluid-filled sac that forms when the duct of a Bartholin's gland becomes obstructed.
- Etiology: Obstruction of the duct can be due to inflammation, infection, trauma, or congenital narrowing. When the duct is blocked, the mucus produced by the gland accumulates, forming a cyst.
- Clinical Features:
- Painless swelling: Typically located unilaterally at the posterior aspect of the labia majora, near the vaginal opening (4 or 8 o'clock position).
- Size: Can range from small to several centimeters, potentially causing discomfort during walking, sitting, or intercourse.
- Discomfort: Larger cysts can cause pressure or a sensation of fullness. The statement "swelling of labia majora during sexual excitement" might refer to the cyst becoming more noticeable or slightly larger due to increased blood flow, but the cyst itself is not erectile tissue.
- Diagnosis: Clinical examination.
- Treatment:
- Asymptomatic cysts: Often require no treatment.
- Symptomatic cysts:
- Sitz baths: Warm compresses can sometimes encourage drainage.
- Word Catheter Insertion: A small catheter is inserted into the cyst, inflated, and left in place for several weeks to create a new drainage pathway (marsupialization).
- Marsupialization: A surgical procedure where the cyst is incised, drained, and the edges of the cyst wall are sutured open to the skin, creating a permanent opening.
- Excision of the gland: Rarely performed due to potential for scarring and disfigurement, and risk of recurrence if not completely removed. Reserved for recurrent cases or suspicion of malignancy.
3. Bartholin's Abscess
- Description: An infection of a Bartholin's gland or cyst, leading to the formation of a pus-filled collection.
- Etiology: Most commonly results from bacterial infection of an existing Bartholin's cyst. Common causative organisms include E. coli, staphylococci, streptococci, and sexually transmitted bacteria (e.g., Neisseria gonorrhoeae, Chlamydia trachomatis).
- Clinical Features:
- Severe, throbbing pain: Unilateral, often making walking, sitting, and intercourse excruciatingly painful.
- Erythema (redness), swelling, and tenderness: Of the affected labium majora.
- Hotness (increased local temperature).
- Fever and chills: May be present if the infection is significant.
- Fluctuant mass: A pus-filled lesion that may spontaneously rupture, providing temporary relief.
- Diagnosis: Clinical examination.
- Treatment:
- Incision and Drainage (I&D): The primary treatment. A small incision is made to drain the pus.
- Word Catheter: Can be inserted after drainage to keep the site open and promote healing.
- Antibiotics: Often prescribed, especially if there is significant cellulitis, systemic symptoms (fever), or risk factors for STIs.
- Sitz baths: Can aid in comfort and healing post-drainage.
4. Herpes Simplex (Genital Herpes)
- Description: A sexually transmitted infection (STI) caused by the Herpes Simplex Virus (HSV), typically HSV-2, but HSV-1 (oral herpes) can also cause genital lesions. It is characterized by recurrent outbreaks of painful sores.
- Transmission: Direct skin-to-skin contact, typically during sexual activity, even when lesions are not visible (asymptomatic shedding).
- Clinical Features:
- Primary Infection: Often the most severe. Symptoms include:
- Multiple, painful vesicles (blisters): Small, fluid-filled, which quickly rupture to form shallow, exquisitely painful ulcers on the vulva, perineum, vagina, and cervix.
- Flu-like symptoms: Fever, headache, malaise, muscle aches.
- Lymphadenopathy: Tender, swollen inguinal lymph nodes.
- Dysuria: Painful urination, sometimes leading to urinary retention due to severe pain upon voiding.
- Recurrent Episodes: Less severe and shorter in duration than primary outbreaks. Often preceded by prodromal symptoms like tingling, itching, or burning at the site of future lesions. Lesions tend to be fewer and localized.
- Factors Triggering Recurrence: Stress, illness, fever, sunlight, menstruation, trauma, sexual intercourse. The statement "oral, vaginal and haematogenous" for transmission is partly misleading; haematogenous spread is rare in typical genital herpes. Oral transmission usually refers to oral-genital contact.
- Primary Infection: Often the most severe. Symptoms include:
- Diagnosis: Viral culture, PCR, or antigen detection from fluid in vesicles or ulcers. Serology for HSV antibodies can determine past exposure.
- Treatment:
- Antiviral Medications: Acyclovir, valacyclovir, famciclovir. These do not cure herpes but can reduce the severity and frequency of outbreaks, promote healing, and suppress viral shedding.
- Episodic Therapy: Taken at the onset of an outbreak or prodromal symptoms.
- Suppressive Therapy: Taken daily to prevent outbreaks, especially for frequent or severe recurrences.
- Symptomatic Relief: Pain relievers (NSAIDs), topical anesthetics (e.g., lidocaine cream), sitz baths, loose clothing.
- Antiviral Medications: Acyclovir, valacyclovir, famciclovir. These do not cure herpes but can reduce the severity and frequency of outbreaks, promote healing, and suppress viral shedding.
5. Genital Warts (Condylomata Acuminata)
- Description: Benign epithelial growths on the vulva, perineum, vagina, cervix, or anus, caused by infection with the Human Papillomavirus (HPV), particularly low-risk types (e.g., HPV 6 and 11).
- Transmission: Primarily through sexual contact.
- Clinical Features:
- Warty growths: Can be flesh-colored, whitish, or reddish-brown. They can be small or large, solitary or clustered, and may have a cauliflower-like appearance.
- Location: Commonly found on the labia, perineum, perianal area, vagina, and cervix.
- Symptoms: Often asymptomatic, but can cause itching, burning, discomfort, bleeding, or pain during intercourse.
- Diagnosis: Clinical appearance. Biopsy may be performed for atypical lesions or if there's uncertainty.
- Treatment: Aims to remove visible warts and alleviate symptoms, but does not eradicate the underlying HPV infection.
- Patient-applied treatments: Imiquimod cream (immune response modifier), podofilox solution/gel (cytotoxic agent).
- Clinician-applied treatments:
- Trichloroacetic Acid (TCA): Chemical cautery.
- Cryotherapy: Freezing with liquid nitrogen.
- Surgical Excision: Cutting out the warts.
- Electrocautery: Burning off the warts.
- Laser Therapy: Vaporizing the warts.
- Prevention: HPV vaccination (Gardasil 9) is highly effective in preventing infection with the most common high-risk HPV types (associated with cancer) and low-risk types (associated with genital warts).
6. Herpes Zoster (Shingles)
- Description: A painful viral rash caused by the reactivation of the Varicella-Zoster Virus (VZV), the same virus that causes chickenpox.
- Etiology: After a primary chickenpox infection, VZV remains latent in the dorsal root ganglia. Reactivation occurs when the immune system is weakened (e.g., by age, stress, illness, immunosuppression).
- Clinical Features:
- Prodromal Phase: Often involves localized pain, tingling, itching, or numbness in the affected dermatome for several days before the rash appears.
- Painful rash: Characterized by a band-like (dermatomal) distribution of vesicles on an erythematous base. The lesions do not cross the midline, as they are confined to the sensory distribution of a single or contiguous nerve.
- Location: While it can affect any dermatome, if it affects the sacral dermatomes (S2-S4), it can appear on the vulva or perineum, causing intense pain.
- Resolution: Vesicles progress to pustules, crust over, and heal within 2-4 weeks.
- Complications: Post-herpetic neuralgia (PHN): Persistent pain in the affected dermatome even after the rash has healed, especially common in older individuals.
- Diagnosis: Clinical appearance. Viral culture or PCR can confirm.
- Treatment:
- Antiviral Medications: Acyclovir, valacyclovir, famciclovir. These are most effective if started within 72 hours of rash onset, reducing pain, shortening the duration of the rash, and decreasing the risk of PHN.
- Pain Management: NSAIDs, neuropathic pain medications (gabapentin, pregabalin) for PHN.
- Vaccination: The shingles vaccine (Shingrix) is highly effective in preventing herpes zoster and PHN in adults over 50.
7. Imperforate Hymen
- Description: A congenital anomaly where the hymen completely obstructs the vaginal opening, without any natural perforations.
- Etiology: Failure of the central portion of the hymen to canalize during fetal development.
- Clinical Features (typically present at puberty):
- Primary amenorrhea: Absence of menstruation by age 15-16, despite normal secondary sexual characteristics.
- Cyclic abdominal or pelvic pain: Due to the accumulation of menstrual blood within the vagina (hematocolpos), uterus (hematometra), and potentially fallopian tubes (hematosalpinx).
- Bulging bluish mass: Visible at the introitus, especially if hematocolpos is significant.
- Urinary symptoms: Pressure on the bladder can lead to urinary frequency or retention.
- Back pain.
- Diagnosis: Clinical examination. Ultrasound can confirm the presence of accumulated blood.
- Treatment: Surgical incision (hymenotomy or hymenectomy): A crucial procedure to create an opening and allow drainage of accumulated menstrual blood. This typically provides immediate relief of symptoms.
8. Disorders of Sexual Development (DSD) / Ambiguous Genitalia (formerly Hermaphroditism)
- Description: As mentioned in the male external genitalia section, these are congenital conditions where there is a discrepancy between the external genitalia and the internal reproductive organs or chromosomal sex. The term "hermaphroditism" is outdated and replaced by DSD.
- Clinical Features in the Vulva: This can manifest as ambiguous genitalia at birth, where the external genitalia are not clearly male or female. For example, in a female (XX karyotype) with congenital adrenal hyperplasia, there might be significant virilization leading to clitoromegaly (enlarged clitoris resembling a small penis) and fusion of the labia, making the gender assignment difficult.
- Diagnosis and Management: Requires a multidisciplinary team involving geneticists, endocrinologists, neonatologists, and surgeons to determine chromosomal sex, gonadal sex, and internal anatomy, followed by appropriate medical, surgical, and psychological management, with careful consideration of gender identity.
Female Internal Genitalia
The female internal genitalia are located within the pelvic cavity and are essential for reproduction. They include the organs responsible for producing ova (eggs), facilitating fertilization, nurturing a developing fetus, and enabling childbirth.
The internal genitalia are composed of:
- Ovaries (Gonads)
- Uterine Tubes (Fallopian Tubes or Oviducts)
- Uterus
- Vagina
1. Ovaries (Female Gonads)
- Description: Paired, almond-shaped organs, typically whitish or grayish in color, located on either side of the uterus, within the pelvic cavity. They are homologous to the testes in males.
- Size: In young, reproductive-aged women, each ovary measures approximately 3-5 cm (1.5-2 inches) in length, 2-3 cm (1 inch) in width, and 1-1.5 cm (1/3 inch) in thickness. After menopause, due to hormonal changes, they tend to shrink and become less active.
- Function: The ovaries have two primary functions:
- Oogenesis: Production and release of female gametes (ova or eggs). Females are born with a finite, lifelong supply of primordial follicles, each containing an immature oocyte. This process begins before birth and continues until menopause.
- Hormone Production: Secrete crucial female sex hormones, primarily:
- Estrogen: Responsible for the development of female secondary sexual characteristics, growth of the uterine lining, and regulation of the menstrual cycle.
- Progesterone: Primarily involved in preparing the uterus for pregnancy, maintaining pregnancy, and regulating the menstrual cycle.
- (Also produce small amounts of androgens).
- Location and Support: Suspended in the pelvic cavity by several ligaments:
- Suspensory Ligament of the Ovary: Connects the ovary to the lateral pelvic wall, containing the ovarian artery and vein.
- Ovarian Ligament: Connects the ovary to the lateral aspect of the uterus.
- Mesovarium: A fold of peritoneum that attaches the ovary to the posterior surface of the broad ligament.
- Microscopic Structure: Consists of an outer cortex (containing ovarian follicles at various stages of development) and an inner medulla (containing blood vessels, nerves, and lymphatic vessels).
2. Uterine Tubes (Fallopian Tubes or Oviducts)
- Description: Paired, muscular tubes that extend from the superior lateral aspects of the uterus towards the ovaries, but do not directly attach to them. They provide a passageway for the ovum from the ovary to the uterus and are the typical site of fertilization.
- Length and Width: Measure approximately 10-13 cm (4-5 inches) in length. Their width varies, being widest at the ovarian end (infundibulum, about 1 inch) and narrowest where they enter the uterine wall (isthmus, diameter of a thin spaghetti strand).
- Segments (from lateral to medial):
- Infundibulum: The funnel-shaped, most lateral part, opening into the peritoneal cavity. It is fringed with finger-like projections called fimbriae.
- Fimbriae: Ciliated projections that sweep over the surface of the ovary. During ovulation, they become more active and swell, helping to "catch" the released ovum.
- Ampulla: The longest and widest part of the tube, where fertilization typically occurs.
- Isthmus: A narrower, thick-walled segment connecting the ampulla to the uterus.
- Interstitial (or Intramural) Part: The segment that passes through the muscular wall of the uterus.
- Infundibulum: The funnel-shaped, most lateral part, opening into the peritoneal cavity. It is fringed with finger-like projections called fimbriae.
- Wall Structure: Composed of three layers:
- Mucosa: Lined with ciliated columnar epithelial cells and secretory (peg) cells. The cilia beat in waves towards the uterus, moving the ovum, while peg cells provide nourishment for the ovum and sperm.
- Muscularis: Smooth muscle layers that contract rhythmically (peristalsis) to help propel the ovum towards the uterus.
- Serosa: Outer peritoneal covering.
- Function:
- Ovum Transport: Fimbriae capture the ovum after ovulation, and the coordinated action of cilia and muscular peristalsis transports it towards the uterus.
- Site of Fertilization: The ampulla is the most common site where sperm meets and fertilizes the ovum.
- Sperm Capacitation: The tubal environment contributes to the capacitation of sperm, enabling them to fertilize the ovum.
- Clinical Relevance: Blockage of the fallopian tubes (e.g., due to pelvic inflammatory disease, endometriosis) can lead to infertility. Ectopic pregnancy (implantation of a fertilized egg outside the uterus, most commonly in the fallopian tube) is a significant clinical concern.
3. Uterus
- Description: A hollow, thick-walled, pear-shaped muscular organ located in the pelvic cavity, between the bladder (anteriorly) and the rectum (posteriorly). It is where a fertilized egg implants and develops during pregnancy.
- Size (non-gravid): Approximately 7.5 cm (3 inches) long, 5 cm (2 inches) wide, and 2.5 cm (1 inch) thick.
- Support: Held in place by various ligaments, including the broad ligament, round ligament, uterosacral ligaments, and cardinal ligaments.
- Parts of the Uterus:
- Fundus: The dome-shaped, superior-most portion of the uterus, above the openings of the fallopian tubes. This is the primary site of implantation for a normal pregnancy.
- Body (Corpus): The main, largest part of the uterus, extending from the fundus to the isthmus.
- Isthmus: A constricted, narrow region between the body and the cervix.
- Cervix: The lowermost, cylindrical portion of the uterus that projects into the vagina.
- Wall Structure (Three Layers):
- Perimetrium: The outermost serous layer, part of the peritoneum.
- Myometrium: The thick, muscular middle layer, composed of interlacing bundles of smooth muscle. It is responsible for uterine contractions during labor and menstruation. It expands significantly during pregnancy (10-20 times its normal size) to accommodate the growing fetus.
- Endometrium: The inner lining of the uterine cavity, a vascular and glandular mucous membrane. It undergoes cyclical changes in response to ovarian hormones (estrogen and progesterone).
- Function: Thickens during the menstrual cycle to prepare for the implantation of a fertilized egg. If fertilization and implantation do not occur, the superficial layer of the endometrium (stratum functionalis) is shed during menstruation. If implantation occurs, the endometrium forms the maternal part of the placenta.
- Function:
- Implantation and Gestation: Provides a suitable environment for the implantation of a fertilized egg and supports fetal development throughout pregnancy.
- Childbirth: Its strong muscular contractions (myometrium) are crucial for expelling the fetus during labor.
- Menstruation: Sheds its inner lining if pregnancy does not occur.
4. The Cervix
- Description: The narrow, cylindrical lower portion of the uterus that connects the uterus to the vagina. It acts as a gateway between the uterine cavity and the vaginal canal.
- Parts:
- Ectocervix: The portion that protrudes into the vagina, covered by stratified squamous epithelium.
- Endocervix: The canal leading into the uterus, lined by columnar glandular epithelium.
- Transformation Zone: The area where the squamous epithelium of the ectocervix meets the columnar epithelium of the endocervix. This area is highly susceptible to HPV infection and cervical cancer.
- Cervical Mucus: The endocervical glands produce cervical mucus, which changes in quality and quantity throughout the menstrual cycle, primarily influenced by estrogen and progesterone levels:
- High Estrogen (around ovulation): Mucus becomes thin, watery, clear, and "stretchy" (spinnbarkeit). This creates a "friendly environment" for sperm, facilitating their passage into the uterus.
- High Progesterone (after ovulation, during luteal phase): Mucus becomes thick, viscous, and opaque, forming a "mucus plug" that hinders sperm entry and protects the uterine cavity from infection.
- Function:
- Sperm Transport and Barrier: Regulates sperm entry into the uterus.
- Protection: Acts as a physical and chemical barrier against infection ascending from the vagina into the uterus.
- Childbirth: During labor, the cervix effaces (thins) and dilates (opens) significantly (up to 10 cm or roughly 50 times its normal width), allowing the baby to exit the uterus into the vagina.
5. The Vagina
- Description: A muscular, elastic tube (sheath-like, from Latin "vagin") that extends from the cervix to the vulva (external genitalia).
- Length: Typically 7-10 cm (3-4 inches) long.
- Structure:
- Muscular Wall: Composed of smooth muscle with an inner layer of stratified squamous epithelium, arranged in transverse folds called rugae, which allow for significant distension during childbirth and intercourse.
- No Glands: The vaginal wall itself does not contain glands. Lubrication primarily comes from cervical mucus, transudation across the vaginal walls during arousal, and secretions from the greater and lesser vestibular glands.
- Function:
- Sexual Intercourse: Receives the penis and sperm during coitus. Its elasticity and rugae accommodate the penis.
- Birth Canal: Serves as the passageway for the baby during vaginal delivery.
- Menstrual Flow: Provides an exit route for menstrual blood from the uterus.
- Protection: Its acidic environment (due to lactic acid produced by normal bacterial flora, primarily Lactobacillus) helps protect against pathogenic infections.