Chromosomal Abnormalities
These abnormalities result from errors in chromosome number (aneuploidy) or structure. They are often severe and can affect multiple organ systems, leading to distinct syndromes.
A. Aneuploidies (Abnormal Number of Chromosomes)
Aneuploidies are typically caused by non-disjunction—the failure of chromosomes to separate properly during meiosis.

Down Syndrome (Trisomy 21)
Cause: An extra copy of chromosome 21 (47, XX/XY, +21).
Incidence: ~1 in 700 live births; risk increases with maternal age.
Key Features:
- Characteristic Facial Features: Upward slanting eyes, epicanthal folds, flat nasal bridge.
- Intellectual Disability: Mild to moderate severity.
- Congenital Heart Defects: Very common (e.g., AV septal defect).
- Other Signs: Hypotonia (poor muscle tone), single palmar crease, increased risk of leukemia and early-onset Alzheimer's.
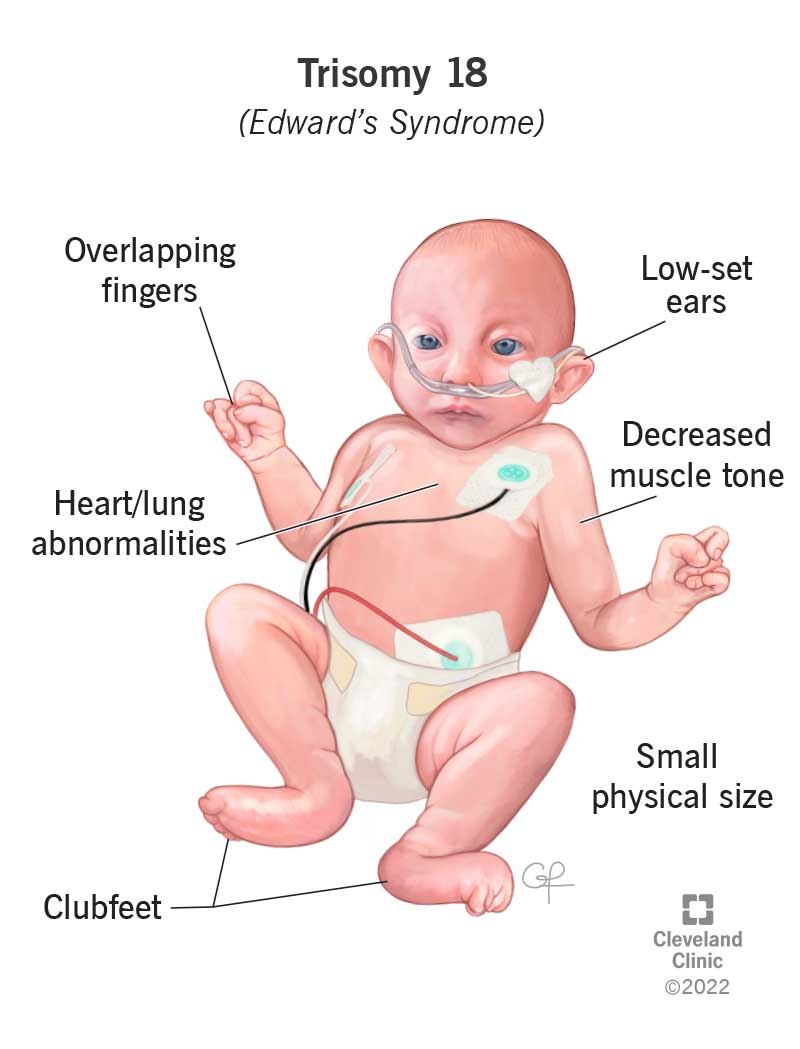
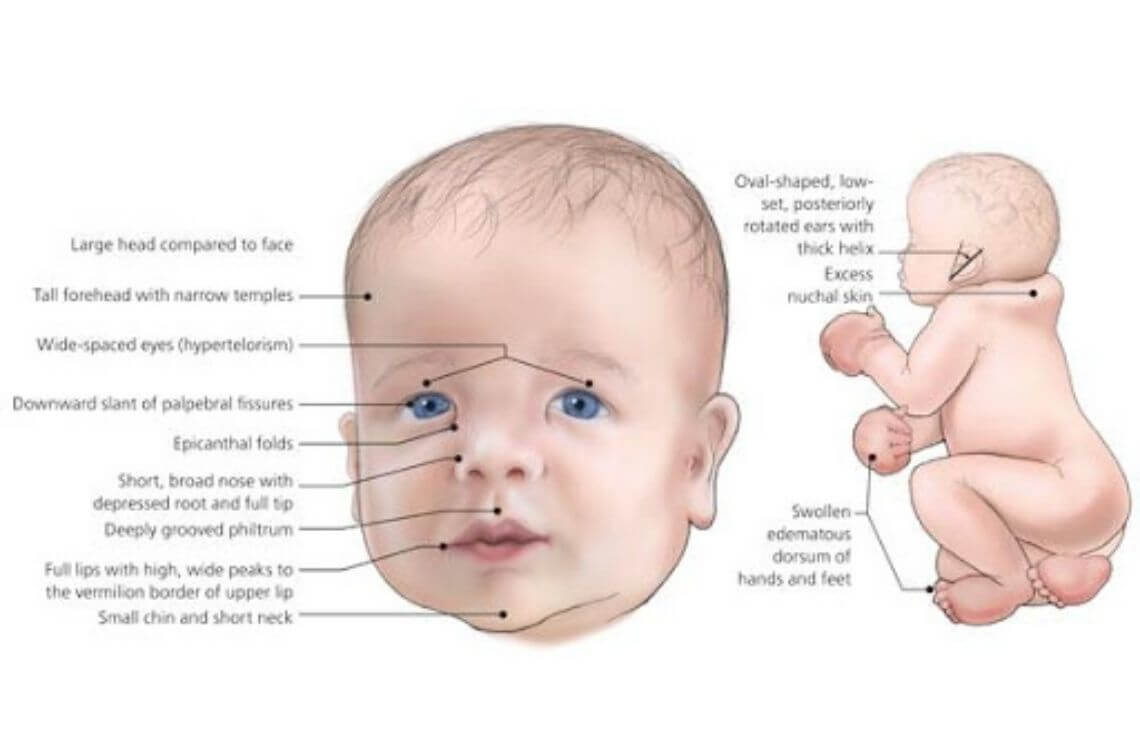
Edward Syndrome (Trisomy 18)
Cause: An extra copy of chromosome 18 (47, XX/XY, +18).
Incidence: ~1 in 5,000 live births; severe prognosis.
Key Features:
- Severe Intellectual Disability & Growth Retardation.
- Characteristic Physical Features: Small head (microcephaly), small jaw (micrognathia), low-set ears, clenched hands with overlapping fingers, rocker-bottom feet.
- Major Organ Defects: Severe heart and kidney malformations.
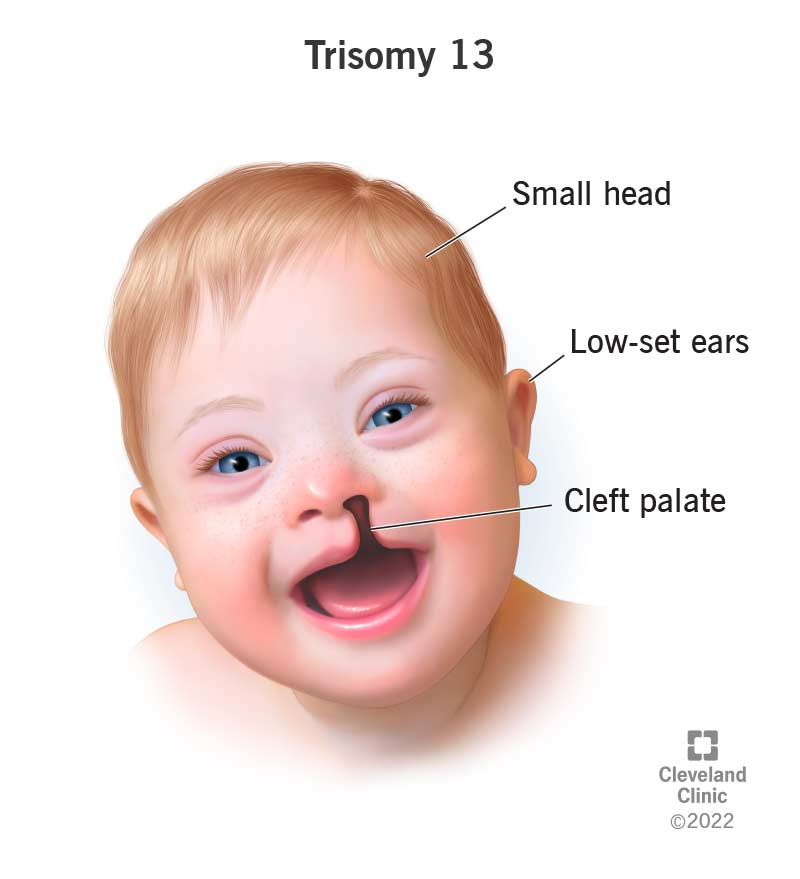
Patau Syndrome (Trisomy 13)
Cause: An extra copy of chromosome 13 (47, XX/XY, +13).
Incidence: ~1 in 16,000 live births; severe prognosis.
Key Features:
- Major CNS Malformations: Holoprosencephaly (failure of forebrain to divide).
- Facial Anomalies: Cleft lip and/or palate, small or absent eyes.
- Polydactyly (extra fingers or toes).
- Severe heart and renal defects.

Turner Syndrome (Monosomy X)
Cause: Affects females; absence of one X chromosome (45, XO).
Incidence: ~1 in 2,500 live female births.
Key Features:
- Short Stature and Webbed Neck.
- Ovarian Dysgenesis: Underdeveloped ovaries leading to infertility.
- Broad Chest with widely spaced nipples.
- Heart Defects: Coarctation of the aorta is common.
- Normal intelligence, but may have specific spatial learning difficulties.

Klinefelter Syndrome
Cause: Affects males; an extra X chromosome (47, XXY).
Incidence: ~1 in 500-1,000 live male births.
Key Features:
- Tall Stature.
- Hypogonadism: Small testes, leading to infertility and reduced testosterone.
- Gynecomastia (breast development).
- Increased risk of learning difficulties (often language-based).
- Frequently undiagnosed until puberty or an infertility workup.
B. Structural Chromosomal Abnormalities
These involve changes in the structure of a chromosome, such as deletions, duplications, or translocations. An important example is:
Cri-du-chat Syndrome
Caused by a deletion on the short arm of chromosome 5. It is characterized by severe intellectual disability, microcephaly, and a distinctive high-pitched, cat-like cry in infancy.